
Abstract
Background
Epidemiological studies suggest an unclear effect of alcohol consumption on cardiovascular risk. This ambiguity is likely related to the quantity of alcohol consumed in populations studied. The aim of this work was to evaluate the association between chronic alcohol consumption and several clinical and biochemical parameters related to coronary risk, in cardiovascular disease free men and women.
Methods
The ‘ATTICA’ study is a population-based cohort, which randomly enrolled 750 men and 883 women (18-88 years old) from area around Athens, during 2001-2002. We investigated the association between alcohol consumption and arterial blood pressure, fibrinogen levels, glucose concentration, total cholesterol, HDL and LDL, apolipoprotein A1 and B, Lp(a), uric acid, leucocyte count, triglycerides, C-reactive protein and homocysteine levels.
Results
Multivariate analysis, after controlling for several potential confounders, revealed a J-shaped association between alcohol intake (none, 1-2, 3-4, 5+ wine glasses/day) and uric acid, C-reactive protein, homocysteine, fibrinogen, triglycerides, apolipoproteins A1 and B, HDL and total cholesterols, blood glucose levels, leucocyte count and arterial blood pressure levels (only in males). The most beneficial values of all these biochemical and clinical parameters were found in alcohol intake of 100-200 ml (12% alcohol), even after adjustment for various potential confounders.
Conclusions
The controversial association between alcohol intake and cardiovascular disease seems to be partially explained by the J-shaped relation of several biochemical parameters related to atherosclerosis and the amount of alcoholic beverages consumed.
Introduction
Although alcohol consumption may be considered as a component of diet, it is addressed separately owing to special interest in the association of some levels of intake, in comparison with other food items, with lower risks of coronary heart disease and stroke. The association between alcohol consumption and the development of coronary heart disease (CHD) is complex and not fully understood [1–6]. Some of the health benefits may be mediated by genetic factors [7]. Observational studies support that light to moderate alcohol consumption is associated with lower risk of myocardial infarction and cardiovascular death. In contrast, heavier alcohol consumption is associated with no change or even an increase in coronary risk [1, 2]. Additionally, investigators have shown linear and U-shaped associations between alcohol consumption and various lipidaemic and thrombogenic factors [4–6]. Moreover, some suggested that only wine, especially red, might be more beneficial than beer or spirits [7]. However, it remains controversial whether alcohol or any type of alcoholic beverage confers any health advantage over wine, red or white, as well as the pathway by which alcohol consumption may influence human health.
The purpose of this study was to investigate the association between chronic alcohol consumption, in various quantities, and several characteristics of the participants, such as arterial blood pressures, serum concentrations of total cholesterol, HDL-cholesterol, LDL-cholesterol, triglycerides, uric acid, leucocyte count, apolipoprotein A1 and B, lipoprotein-a (Lp(a)), fibrinogen levels, homocysteine plasma levels and high sensitivity C-reactive protein levels (hs-CRP), in a population-based sample of adults representative of a Mediterranean country, Greece.
Methods
Study design
The ‘ATTICA’ project is a health and nutrition survey carried out in the province of Attica, where Athens is a major metropolis, during 2001-2002. A stratified sample of 750 males and 883 females was drawn from the general population, aged 18 years or over, excluding people living in institutions. The stratification was based on the age—sex—city distribution provided by the National Statistical Service according to the census of 2000. There were only minor differences in distribution by sex and age between the study population and the target population. The study design anticipates enrolling only one participant per household. The sampling was random. The number of the participants was determined by power analysis, and chosen to evaluate: 1) differences in coronary relative risk of greater than 10%, and 2) differences between the investigated parameters greater than 20%, achieving statistical power <0.80 at P >0.05. The participation rate is about 68%. The analyses presented in this work are based on individuals with complete data for all variables and without any clinical evidence of coronary heart disease, stroke or any atherosclerotic disease. All participants were interviewed by trained personnel who used a standard questionnaire.
Investigated parameters
The questionnaire included demographic characteristics (age, sex, financial status and education), detailed medical history, daily dietary habits (using a validated nutrient questionnaire provided by the Division of Nutrition, Department of Epidemiology, Athens Medical School) and lifestyle habits, such as smoking status and regular physical activity. The daily alcohol intake was assessed in a 7-day food record. All alcohol consumed was adjusted to 100 ml of 12% ethanol concentration.
Regarding the rest of the investigated parameters, the educational level of the participants (as an index of social status) was classified into three groups on the basis of self-administered questionnaires. Group I members had received education up to high school. These participants reported comprehensive school, trade school or technical institute/school as their basic education, but had not passed senior high school. Group II members had completed senior high school, but had not attained a university education. Group III members had studied at, or graduated from, university or college, or a technical school for at least two years. Information about smoking habits was collected using a standardized questionnaire developed for the study. Current smokers were defined as those who smoked at least one cigarette per day. Never smokers were those who had never tried a cigarette in their life and former smokers were defined as those who had stopped smoking more than one year previously. For the multivariate statistical analyses cigarette smoking was quantified in pack-years (cigarette packs per day × years of smoking), adjusted for a nicotine content of 0.8 mg/ cigarette. All participants were classified at entry according to their regular physical activity. Class 1 were sedentary, engaging in little exercise; class 2 were moderately active during a substantial part of the day; and class 3 performed hard physical work much of the time. Classification was based on the responses to questions about the occupation and usual activities, including part-time jobs and notable nonoccupational exercise. Height was measured, to the nearest 0.5 cm, without shoes, back square against the wall tape, eyes looking straight ahead (visual axis is horizontal when the top of external auditory meatus is level with the inferior margin of bony orbit), with a right-angle triangle resting of the scalp against the wall. Weight was measured with a lever balance, to the nearest 100 g, without shoes, in light undergarments. We also measured waist to hip ratio. Body mass index was measured as weight (in kilograms) divided by standing height (in m2). Obesity was defined as body mass index <29.9 kg/m2.
Arterial blood pressure was measured at the end of the physical examination with the subject in sitting position. Blood pressure was taken with the right arm relaxed and well supported by a table, at an angle of 45° from the trunk. The systolic blood pressure level was determined by the first perception of sound (of tapping quality). The diastolic blood pressure I (or phase IV) level was determined when the sounds cease to be tapping in quality and become fully muffed. Changes in loudness were not considered. Blood samples were collected from the antecubital vein between 8-10 a.m., in a sitting position after 12 hours of fasting and avoiding alcohol. For the determination of plasma fibrinogen blood was anticoagulated with 3.8% trisodium citrate (9:1 vol/vol) and cooled on ice until centrifugation. For determination of homocysteine, blood was collected in a cool vacutainer containing EDTA, which was stored on ice for a maximun of 2 h until centrifugation at 3000 g for 5 min at 4°C. All the other biochemical examinations (uric acid, urea, creatinine, total cholesterol, LDL-cholesterol, HDL-cholesterol, triglycerides) were measured using chromatographic enzymic method in a Technicon automatic analyser RA 1000. Apolipoproteins A1 and B, Lp(a), hs-CRP levels, as well as fibrinogen levels were measured by a BNII Dade Behring automatic nephelometry. Finally plasma homocysteine levels were measured with an automatic Abott Axsym analyser, which is based on the technology of polarized immunofluorescence (FPIA). The intra- and inter-assay coefficients of variation of fibrinogen did not exceed 9%, homocysteine 8%, total cholesterol 8%. Hypertension was defined as a systolic blood pressure ≥ 140 mmHg, a diastolic blood pressure ≥ 90 mmHg, or the use of any antihypertensive medication; hypercholesterolaemia was defined as total cholesterol levels greater than 220 mg/dl or the use of antilipidaemic medication; and diabetes mellitus as a fasting blood sugar 125 mg/dl or the use of antidiabetic medication.
Statistical analysis
Continuous variables are presented as mean values ± one standard deviation, while qualitative variables are presented as absolute and relative frequencies. Associations between categorical variables were tested by the use of contingency tables and the calculation of chi-squared test. Comparisons between normally distributed continuous variables and categorical were performed by the calculation of Student's t-test and one-way or multi-way Analysis of Variance (ANOVA or MANOVA), after controlling for homoscedacity. In the case of asymmetric continuous variables the tested hypotheses were based on the calculations of nonparametric tests, such as Mann—Whitney and Kruskal—Wallis. Finally, correlations between continuous variables were tested through multiple regression analysis after the adjustment for the potential confounders and interactions. The J-shaped association between the exposure variable (alcohol intake) and the clinical and biochemical markers was illustrated by connecting the mean values of the investigated parameters using cubic splines. Spline is a function such that each of the intervals [0,1-2], [1-2, 3-4], and [3-4, + 5] wine glasses per day, produces a cubic polynomial, after taking into account the effect of age, gender, physical activity status, education level and smoking habits of the participants [8]. All reported P-values are based on two-sided tests and compared with a significance level of 5%. SPSS 10.1 software was used for all the statistical calculations.
Results
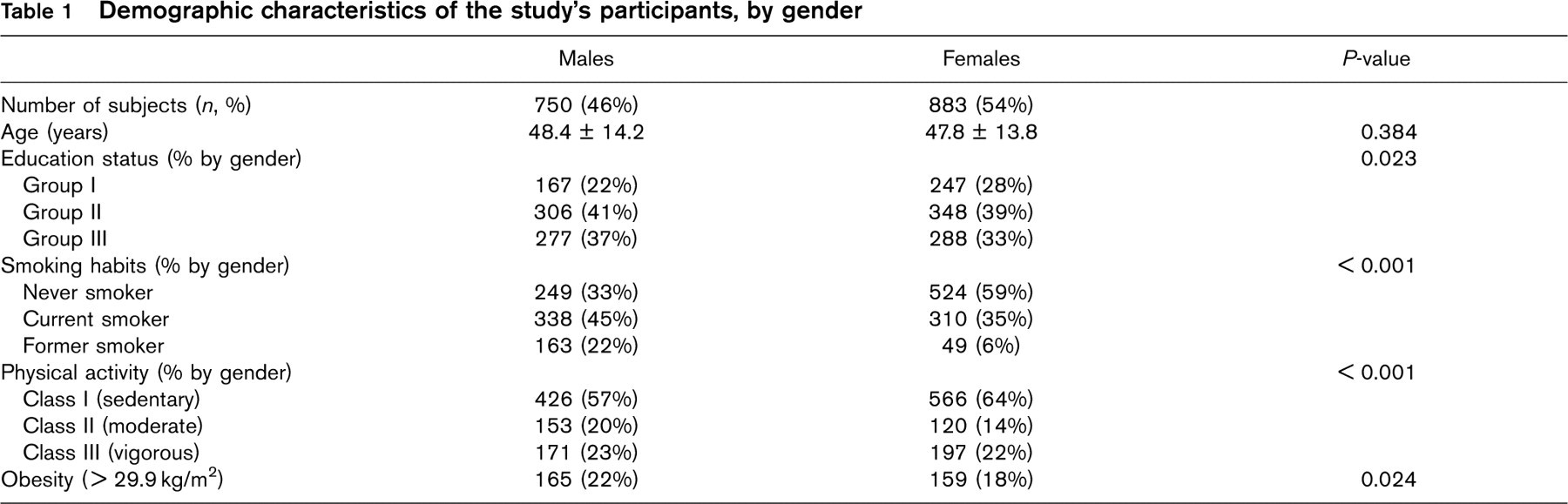
The distribution of the demographic and conventional cardiovascular risk factors, by gender, is presented in Table 1. Males and females were of similar age, while educational status was higher in males (P >0.05). Males were more likely to smoke, be physically active and obese (Table 1). There were no significant differences in the prevalence of hypercholesterolaemia (299 (39.9%) vs. 329 (37.3%), P = 0.28), and diabetes mellitus (54 (7.6%) vs. 56 (6.7%), P = 0.48), while hypertension was more frequent in males (207 (28%) vs. 170 (19%), P >0.001).
Nutrient analysis revealed that alcohol abstinence within the recorded 7-day period was higher in females (87% vs. 62%, P >0.001, for females and males respectively). The age—sex-adjusted distribution of daily alcohol consumption is presented in Figure 1. Middle-aged male participants (45-65 years old) seem to consume higher alcoholic quantities compared with younger or older individuals (P = 0.002), while no statistically significant differences were observed between alcohol consumption and age in females (P = 0.598). Additionally, males consume higher quantities of alcoholic beverages compared with females (P >0.001).
Demographic characteristics of the study's participants, by gender
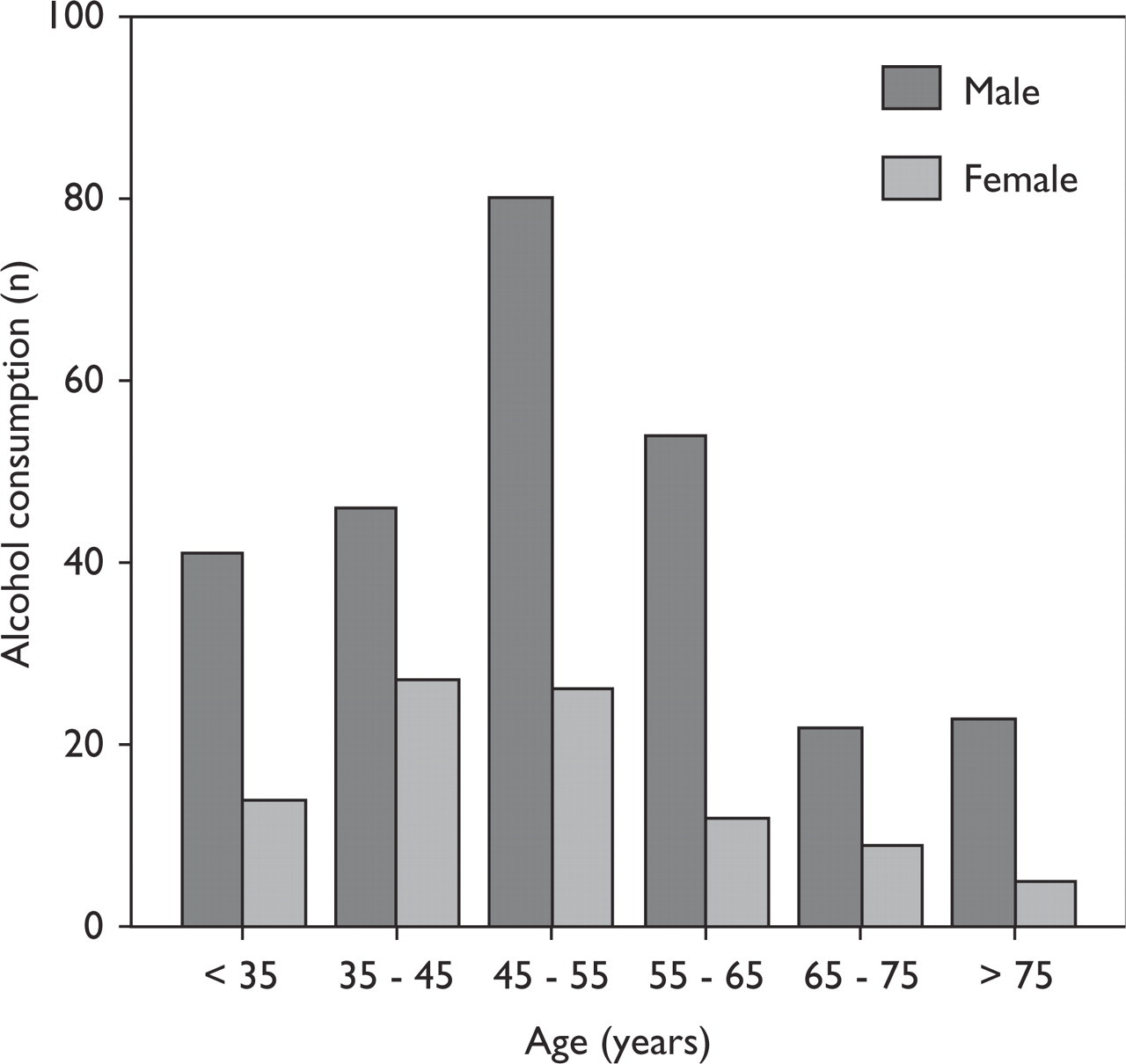
Age-gender adjusted distribution of alcohol consumption (≥ 1 wine glass/day).
No association was found between alcohol consumption and physical activity, obesity or educational status, since both physically active and inactive (active: 225 (25%) vs. inactive: 172 (23%), P = 0.288), obese or normal/over-weight (> 29.9 kg/m2: 79 (25%) vs. ≤ 29.9 kg/m2: 301 (23%), P = 0.549), as well as low, middle and highly educated participants (low: 104 (25%) vs. middle: 160 (25%) vs. high: 123 (22%), P = 0.082), reported consuming similar quantities of alcohol. On the other hand, current smokers were more likely to define as alcohol drinkers compared with never or former smokers (current: 188 (29%) vs. never: 108 (14%), vs. former: 91 (43%), P >0.001).
Multivariate analysis, after controlling for the observed interactions between alcohol consumption and age, gender and smoking habits, revealed a J-shaped association between alcohol quantities consumed (none, 1-2, 3-4, 5 + wine glasses of 100 ml/day) and triglycerides, HDL-cholesterol, apolipoprotein A1 and B, Lp(a) (in males), fibrinogen, homocysteine, C-reactive protein, fasting blood glucose, uric acid and white blood cell counts, in both genders. Moreover, a positive association was observed between arterial blood pressures (only in males) and total cholesterol levels (in males), while no association was found between alcohol consumption and LDL cholesterol levels (Table 1). The most beneficial values of all these biochemical and clinical parameters were found in daily alcohol intake of 100-200 ml (12% alcohol), even after adjustment for various potential confounders described above. Figure 2 illustrates some of the observed J-shaped associations, between alcohol quantities and homocysteine, C-reactive protein, leucocyte count and fibrinogen levels (mean; 95% confidence interval).
Discussion
In the present work we evaluated the dose-response relationships between alcohol consumption and lipid levels, inflammatory and haemostatic factors, in a large sample from the general adult population, who were free of cardiovascular disease. It seems that there is a variant relation, in both genders, between almost all these markers and the reported quantities of alcohol consumed. This might be partially explained by the controversial effect of alcohol consumption on coronary risk reported by several investigators in the past [9, 13–16]. Moreover, the most beneficial impact of alcohol consumption on inflammatory, haemostatic and biochemical factors was found in daily alcohol intake of 100-200 ml (12% alcohol).
Elevated plasma concentrations of homocysteine have been suggested to be a new risk factor of atherosclerotic vascular disease amenable to preventive actions [17–24], but its role as a marker of atherosclerosis is still ambiguous [20–22]. At this point it should be mentioned that earlier studies [9, 10] suggest that age, hypertension, body mass index, serum triglyceride levels, coffee and alcohol consumption were associated with homocysteine levels and might partially influence its effect on coronary risk [20–22]. In this study, after controlling for several potential confounders, we observed a consistent J-shaped association between alcohol consumption and homocys-teine levels, in both genders, with a marked increase in homocysteine levels in higher alcohol intake (Figure 2). Other investigators have also indicated similar relationships between homocysteine and alcohol consumption [22–24]. All these studies suggest an alcohol—homocysteine ‘paradox', whereby alcohol consumption known to be cardioprotective — especially in moderate consumption — elevated homocysteine levels, which is considered to be a cardiovascular disease risk factor. Alternatively, slight raised homocysteine concentrations might be beneficial.
During recent years many mechanisms have been suggested related to lipoproteins, apolipoproteins and HDL cholesterol by which moderate alcohol intake could alter the risk of coronary heart disease [25, 26]. In this study, we revealed that moderate alcohol consumption was associated with higher levels of apolipoprotein A1, HDL-cholesterol, triglycerides and lower levels of Lp(a) (only in males). The most beneficial effects of alcohol consumption were, again, prominent in moderate levels.
Several studies suggest that among inflammatory factors fibrinogen levels play a significant role in the development of atherosclerosis [27, 28]. However, lifestyle factors, including smoking and alcohol consumption, might influence the role of fibrinogen on cardiovascular risk. The present study showed that moderate consumption of alcohol is associated with significantly lower fibrinogen levels. It is interesting that even higher alcohol intake was related to similar fibrinogen levels than the alcohol abstinence (Table 2). As inflammation is considered to have a crucial role in both initiation and progression of atherosclerosis [27] and fibrinogen is an important acute-phase reactant, our findings might partially explain the mechanisms by which moderate alcohol intake can lower coronary risk. In concordance to our findings a cross-sectional study in 4967 French males and females found a strong and independent U-shaped association between alcohol consumption and fibrinogen levels [6]. Also, in an analysis of the Framingham Offspring Study [17], alcohol consumption was found to have complex associations with several haemostatic parameters.
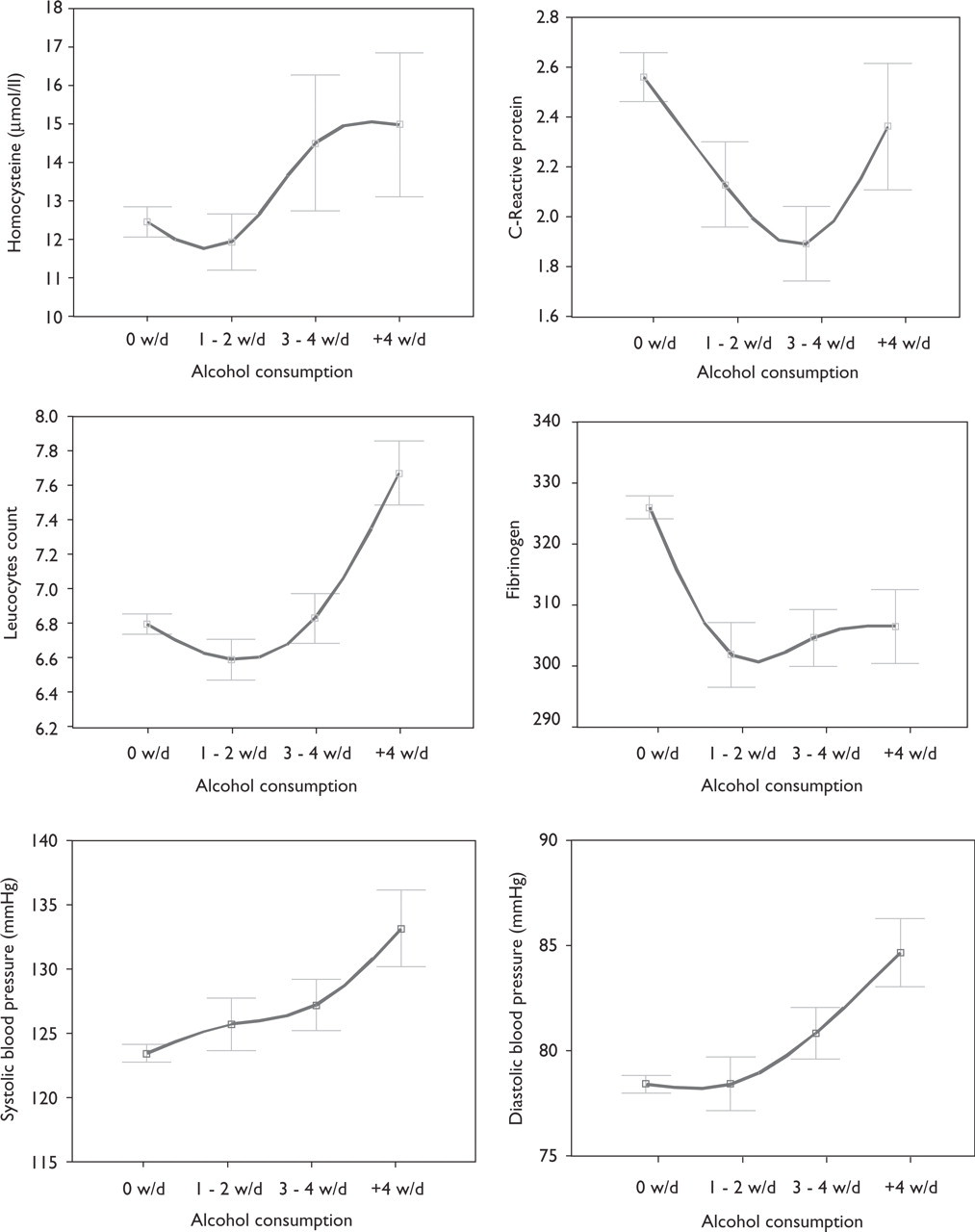
Mean values and 95% confidence interval of homocysteine, C-reactive protein, leucocytes count, fibrinogen and arterial blood pressures, by alcohol consumption; continuous line represents the spline function.
Descriptive characteristics (mean value ± standard deviation) of lipid levels, inflammatory and haemostatic factors, by alcohol consumption level, in males/females
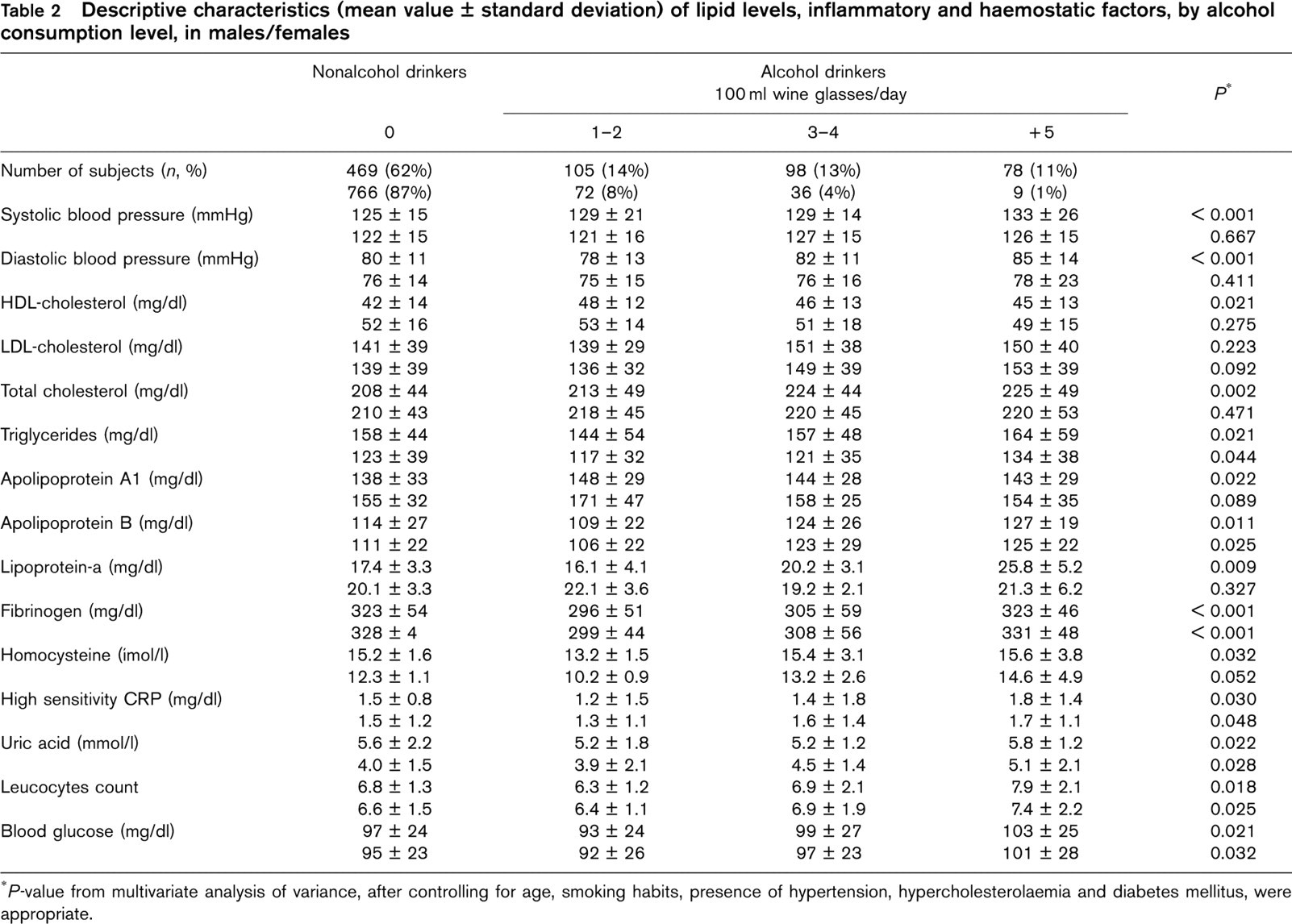
∗P-value from multivariate analysis of variance, after controlling for age, smoking habits, presence of hypertension, hypercholesterolaemia and diabetes mellitus, were appropriate.
There is increasing evidence that atherosclerosis is an inflammatory disease and among other factors total leucocyte count and C-reactive protein levels are considered as independent risk factors for coronary heart disease [28–29]. Following the J-shaped curve, moderate alcohol consumption is associated with lower levels of C-reactive protein and leucocyte count, even after adjustment for various risk factors as diabetes mellitus, smoking habits and hypertension status (Table 2). In the Physician Health Study a U-shaped relation was found between alcohol intake and subsequent total mortality in men with previous myocardial infarction [30]. In the process of atherosclerosis, besides the local procedures in the arterial wall, systematically measurable markers of inflammation have been consistently associated with clinical endpoints [30]. Thus, it seems that a moderate intake of ethanol can beneficially modulate inflammatory response.
Finally, several investigators suggest that daily intake of more than moderate amounts of alcoholic beverages is a risk factor for the development of hypertension [9–13]. In our study alcohol consumption showed a linear association with systolic blood pressure levels and a J-shaped association with diastolic blood pressure levels (Table 2), confirming the hypothesis put forward by other investigators.
In conclusion, in this study we observed a, clear, dose-response relation (J-shape) between several biological markers and alcohol intake, suggesting that these cardioprotective effects may represent a link to lower cardiovascular and overall morbidity and mortality. However, it is hard to claim that our findings suggest causal evidence, and further investigation is needed in order to confirm or refute our hypothesis.
Limitations
The population studied in this work is homogeneous and may reflect lifestyle habits in similar cultures, like Western Europe, Mediterranean countries, etc. Thus, our findings could not extrapolate into other populations without further investigation and consideration. This study as a cross-sectional one cannot establish causal relations but only generate hypotheses. Also, the numbers of participants in categories of high alcohol intake (+ 5 wine glasses per day) were small, and the impression of beneficial effects in some parameters in even higher alcohol consumption may be misleading. Although this analysis has been adjusted for several known confounders, we have not investigated the impact of diet, folate intake, coffee and tea consumption; all of which have mediated effects on serum homocysteine levels. Additionally, misreporting of alcohol consumption due to social class can be a potential confounder.
Footnotes
Acknowledgements
The ATTICA study was supported by research grants from the Hellenic Cardiological Society (HCS2002) and the Hellenic Heart Foundation (HHF2001-HHF2002). The authors would like to thank the investigators of ‘ATTICA’ study: Dr A. Katinioti (physical examination), Dr S. Vellas (physical examination), Ms M. Toutouza (data management), Mr E. Kambaxis (nutritional evaluation), Ms K. Paliou (nutritional evaluation), Ms C. Tselika (technical support), Ms S. Poulopoulou (technical support) and Ms K. Vasiliadou (technical support).