
Abstract
Background
Exercise is recommended for cardiac patients irrespective of beta-blockers. Percentages of maximal heart rate (%HRmax) and heart rate reserve (%HRR) are widely used to determine training intensities. The purpose of this study was to investigate the influence of chronic cardioselective beta blockade on the %HRmax and %HRR model.
Methods
Ten healthy male subjects randomly received oral placebo or beta-blocker bisoprolol (5 mg/day) for 2 weeks using a double-blind, crossover design. In the second week, the subjects performed a cardiopulmonary exercise test until exhaustion to determine the aerobic (AeT) and anaerobic (AnT) threshold.
Results
No significant differences were found for absolute and relative values of oxygen consumption, power output and ratings of perceived exertion at AeT, AnT and maximum workload. Mean HR was significantly (P < 0.05) lower at rest (−15 ± 5 bpm), AeT (−19 ± 8 bpm), AnT (− 22 ± 10 bpm) and maximal workload (−19 ± 11 bpm) with bisoprolol compared to placebo. Percentage of maximal heart rate (%HRmax) was significantly (P < 0.05) reduced at rest (43 versus 39%), AeT (64 versus 60%) and AnT (86 versus 82%), a trend for a reduction was found for %HRR at AnT (75 versus 71%, P=0.07).
Conclusions
Exercise prescription using %HRmax or %HRR methods are of limited accuracy for patients taking beta-blockers. Although %HRmax and %HRR are easy to determine and therefore attractive, we suggest that the most precise exercise prescription would depend on AeT and AnT. Percentages of maximal oxygen consumption or maximal workload or ratings of perceived exertion may be suggested as a substitute. Alternatively, upper limits for %HRmax and %HRR should be lower for patients taking beta-blockers.
Keywords
Introduction
Beta-adrenoceptor blockers are widely prescribed for the treatment of cardiovascular disorders including arterial hypertension, coronary heart disease and congestive heart failure. Patients suffering from these conditions may be relatively young and also physically active. Furthermore, patients are often advised to participate in physical activity and/or cardiac rehabilitation programmes [1–3].
The use of heart rate as an index of training intensities has been widely accepted for the general population and for patients with cardiovascular diseases [3–5]. For the description of training intensities, the percent of maximal heart rate (%HRmax) or the relative intensity of the heart rate reserve (%HRR) is widely used for athletes, healthy sedentary subjects, and patients [3, 5]. Training intensity is one decisive factor for improving maximal oxygen consumption, and several recommendations have been made on the basis of %HRmax or %HRR. The American College of Sports Medicine [1] and the American Heart Association [3] have recommended training intensities between 55% and 65 to 85% (90%) of maximal heart rate (HRmax), or between 40% and 50 to 80% (85%) of heart rate reserve (HRR). These guidelines follow the latest textbooks, with upper limits for %HRmax and %HRR set at 85–90% and 80–85%, respectively [1, 6, 7].
Recently, the validity of the percentage maximum concept for equating training intensity has been questioned [8–10]. The accuracy of the %HRmax and %HRR methods relies on a functional relationship between cardiorespiratory and metabolic markers [1, 6] and may therefore not be applicable under certain circumstances. Furthermore, data have been presented that show that the use of standard HR intensity guidelines results in differing levels of metabolic stress across subjects [11].
Beta-blockers have substantial influence on haemodynamic parameters with reduction of blood pressure and HR at rest and during exercise. Therefore, absolute HR values are reduced for exercise prescription. However, there are no data on the influence of chronic beta-adrenergic blockade on the relative training intensities suggested by the guidelines [1, 3].
In this context, the aim of the present study was to observe the influence of chronic beta-adrenergic blockade on the percentage of maximal heart rate (%HRmax) and the heart rate reserve (%HRR) at submaximal parameters of exercise performance in healthy male subjects.
Subjects and methods
To compare the effects of bisoprolol versus a placebo on HR, statistical power calculations were performed before testing. It was estimated that a minimum of eight subjects were required to achieve a 90% power (β-error 0.10) to detect 10% differences of HR with an α-error of 0.01. The study protocol was approved by the Institutional Ethics Committee of the Karl-Franzens University, Graz, Austria.
Cardiopulmonary exercise testing
Ten healthy male subjects (age 23 ±3 years; height 181 ± 6 cm; weight 76 ± 6 kg) were informed of the nature, risks and benefits of the investigation and gave their written informed consent to participate in the study. Subjects randomly received oral bisoprolol (5 mg/day) or placebo according to a randomized, double-blind, crossover protocol. Each treatment period lasted 2 weeks, with a washout phase of 1–3 weeks between the two treatment periods. Cardiopulmonary exercise testing was performed in the second week of each period. Subjects completed a maximal incremental exercise test on an electronically braked cycle ergometer (Ergoline 900; Schiller, Dresden, Germany). Before testing, subjects sat quietly for 10 min on the cycle ergometer, then underwent an exercise workload of 40 Watts (W) followed by an increase of 20 W every minute thereafter. Values for HR were monitored continuously and stored at 5-s intervals (Sporttester PE4000, Polar Electro, Kempele, Finland). A 12-lead ECG (Schiller, Dresden, Germany) was used to monitor and record the signals; a physician supervised each test. Additionally, ratings of perceived exertion [12] were determined every minute during the cardiopulmonary exercise test.
During the ergometer test, subjects wore an airtight mask over the nose and mouth. The analysers were calibrated with gases of known concentration before each test. Oxygen consumption, carbon dioxide production and ventilation were measured in breath-by-breath mode by an open-air spirometry system (Metamax; Cortex, Leipzig, Germany) and mean values were stored at 10-s intervals. The respiratory equivalents for oxygen consumption (ventilation/oxygen consumption) and carbon dioxide production (ventilation/carbon dioxide production) were calculated offline. The subjects were encouraged to continue until exhaustion and highest level of oxygen uptake achieved during the test was defined as VO2max regardless of whether a VO2 plateau had been established. In all circumstances maximum respiratory exchange rate exceeded 1.10. The HRR was calculated as HRmax-resting HR (measured during the last minute in the pre-exercise period) [1].
Two submaximal values based on a three-phase model [13, 14] were analysed with a computer-aided linear regression break point analysis [9, 15]. The aerobic threshold (AeT) was assessed as the first turn point for the respiratory equivalent for oxygen consumption without a simultaneous increase in the respiratory equivalent for carbon dioxide production between the first workload step and 75% of maximal workload. The anaerobic threshold (AnT) was assessed as the nadir for the respiratory equivalent for carbon dioxide production between AeT and maximal workload [13, 15, 16].
Statistics
Data are reported as mean ± SD values. Paired Student's t-test was used to determine significant differences between bisoprolol and placebo for all measured and calculated variables. Repeated measures ANOVA was performed for multiple comparisons, post hoc analysis was performed by using the Tukey multiple comparison test. The level of significance was set at alpha P < 0.05.
Results
No significant differences between bisoprolol and placebo were found for absolute values of oxygen consumption at rest as well as oxygen consumption and power output at AeT, AnT and at maximal power output. Moreover, the percentages of oxygen consumption and workload in relation to maximal values were not significantly different at rest and submaximal values either (Table 1). No significant difference was found for the respiratory equivalents for oxygen consumption and carbon dioxide production during the cardiopulmonary exercise test.
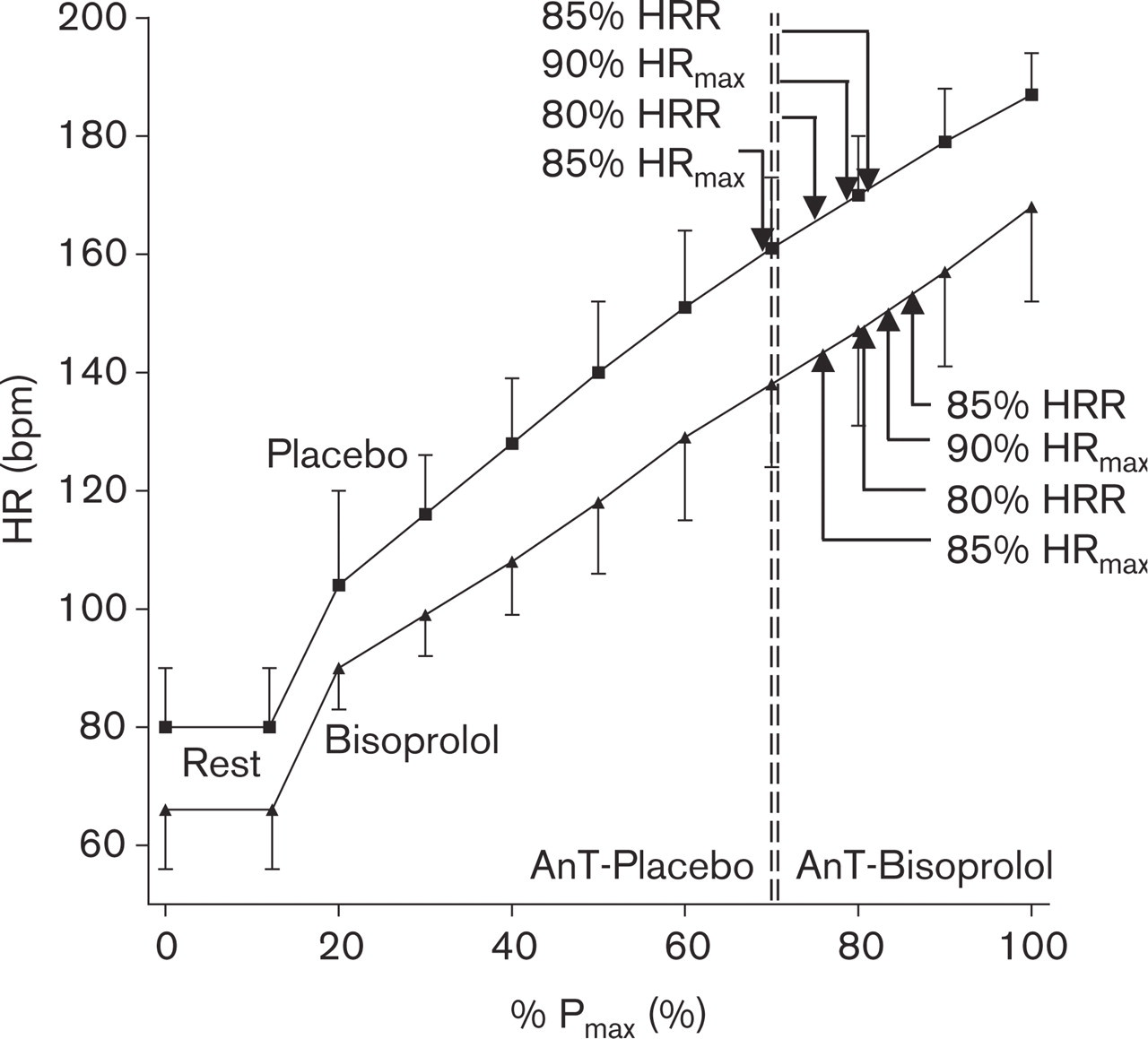
Figure 1 shows the mean HR-response to cardiopulmonary exercise testing in relation to maximal power output (%Pmax) with placebo and bisoprolol. Dotted lines indicate the anaerobic threshold (AnT). Mean HR was significantly lower at rest (−15 ± 5 bpm), at AeT (−19 ± 8 bpm), at AnT (−22 ± 10 bpm) and at maximal power output (−19 ± 11 bpm) with bisoprolol than with placebo (Table 1, Fig. 1). No significant difference was found for maximal heart rate reserve (HRR) with bisoprolol (102 ± 14) and placebo (107 ± 10), respectively, however, there was a significant difference for the percentage of HR compared to HRmax at rest, AeT, and AnT. Furthermore, the relative intensity for the HRR was moderately lower for bisoprolol than for placebo.
A comparison of calculated upper limits of target-HR using recommended training intensities by the guidelines [1, 3] and HR at AnT determined by cardiopulmonary exercise testing is shown in Table 2. ANOVA showed significant differences between measured HR at AnT and calculated target-HR at 90%HRmax and 85%HRR for placebo and at 90%HRmax, 85%HRR and 80%HRR for bisoprolol.
There were no significant differences for ratings of perceived exertion at AeT (11.1 ± 0.9 versus 11.3 ± 1.4), AnT (16.7 ± 1.4 versus 15.9 ± 1.7) and maximal power output (20 ± 0.0 versus 20 ± 0.0) after either bisoprolol or placebo.
Discussion
The main finding was that chronic beta-adrenergic receptor blockade with 5 mg bisoprolol did not show any reduction in oxygen consumption and power output at AeT, AnT and maximal workload in this group of young healthy male subjects. Besides the significant reduction in absolute values of HR under every workload there was also a significant reduction of %HR at rest and at submaximal values compared to HRmax. Moreover, %HRR showed a trend towards a reduction at AnT.
Several reports have been published indicating a negative effect of acute β-adrenergic blockade on oxygen uptake [17]. However, chronic administration of cardioselective beta-blockade has been reported to show no negative impact on maximal exercise capacity [18–20]. Central and peripheral mechanisms may serve as a physiological explanation. Although we did not measure left ventricular function or cardiac output, we may suggest that the reduced HR is at least partially compensated by an elevation in stroke volume [21–23] and an improvement in left ventricular diastolic filling [24]. Moreover, it has been reported that even if muscle blood flow is reduced as a result of a lower cardiac output during beta-blockade, the VO2 of the working muscles remains the same because of an increased oxygen extraction during submaximal or maximal power output [21, 22].
Absolute HR values were reduced, which is one of the desired effects of beta-blockers. The logical impact of the prescription of training intensities is a reduction of absolute values of training heart rate. There has however, only been marginal investigation of the influence of beta-blockade on relative intensity using the %HRmax or %HRR method [25]. We found a decrease in %HRmax and %HRR, however percent of maximal oxygen consumption and maximal workload and ratings of perceived exertion at AeT and AnT were not affected. The findings of Wittke and Kemmler [19], who found no significant change of the relationship of oxygen consumption to workload during an incremental exercise test after selective beta blockade, support our findings. Additionally, in line with our findings, Gordon et al. [25] found an altered relationship of percentage of maximal heart rate to percentage of maximal oxygen consumption in 12 healthy men receiving the cardioselective beta-blocker atenolol.
Effect of cardioselective beta-blockade on cardiorespiratory variables at rest, aerobic threshold (AeT), anaerobic threshold (AnT) and maximal power output
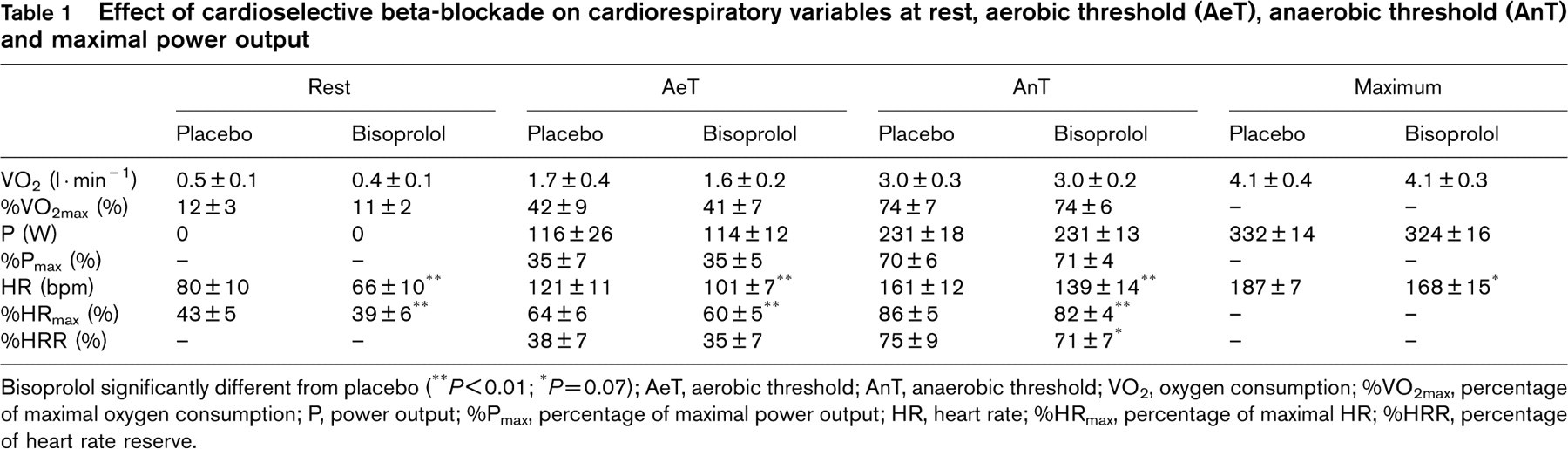
Bisoprolol significantly different from placebo (∗∗P < 0.01; ∗P=0.07); AeT, aerobic threshold; AnT, anaerobic threshold; VO2, oxygen consumption; %VO2max, percentage of maximal oxygen consumption; P, power output; %Pmax, percentage of maximal power output; HR, heart rate; %HRmax, percentage of maximal HR; %HRR, percentage of heart rate reserve.
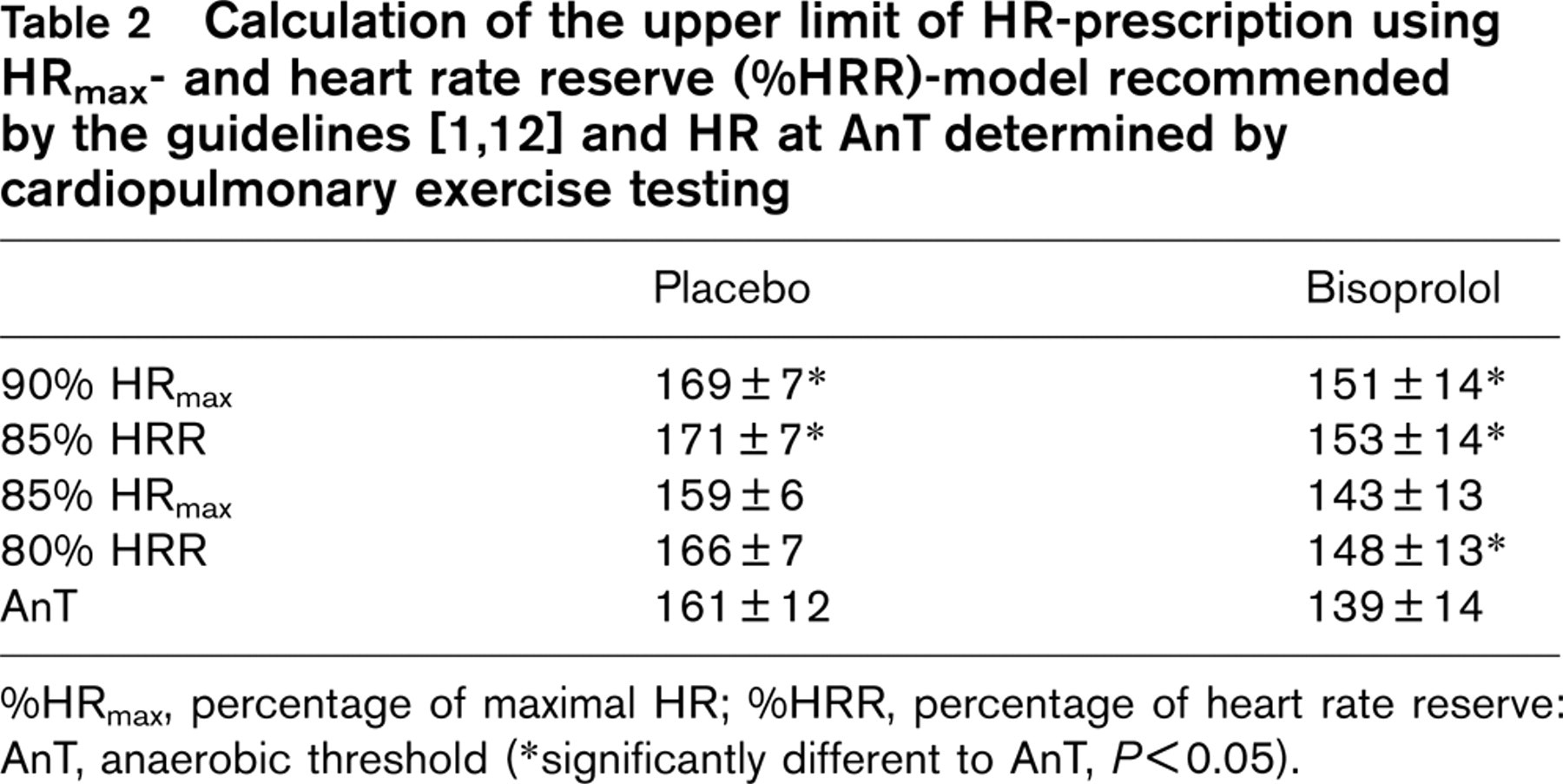
%HRmax, percentage of maximal HR; %HRR, percentage of heart rate reserve: AnT, anaerobic threshold (∗significantly different to AnT, P < 0.05).
Although changes in %HRmax and %HRR were small, our findings have substantial impact for training prescription with regard to the upper limit of exercise training intensity in patients receiving beta-blockers. Differences in target HR can extent up to 14bpm in subjects taking bisoprolol as shown in Table 2.
Exercise is recommended for the general population [5], and especially for persons with cardiovascular disease [2, 3]. Physical training is also recommended for patients receiving beta-blockers [26] and training has been reported to have positive effects on physical performance in these patients [27, 28]. To obtain a training effect, a lower limit of exercise intensity must be reached [1, 6] but patients must be cautioned to avoid harmful overexertion. An elevated risk of sudden cardiac death with vigorous exertion compared to lighter or no exertion has been shown [29]. Accordingly, upper limits for exercise prescription in cardiac patients are recommended [29]. It has been shown that the anaerobic threshold determined with analysis of blood lactate [10, 15, 30, 31], heart rate [10, 15, 30] or respiratory variables [10, 32, 33] gives an indicator for diminished ventricular function above that exercise load. In addition, for patients with coronary heart disease it has been shown, that norepinephrine and blood lactate concentrations are higher during endurance exercise above the AnT than at maximum functional capacity in an incremental test [31]. In support of our findings, it was concluded that endurance exercise with intensities > 70% of maximum functional capacity could overload the cardiac patient and increases the risk of arrhythmia and ischaemia [31]. Guidelines [1, 3] recommend intensities up to 85%HRR after an initial starting intensity of 40–60%HRR. Assuming that 85% of HRmax or 80% of HRR [2, 3] is the maximal training intensity, our results indicate that this intensity of exercise is in the range or even above the AnT (i.e., within one load step) without beta blockade and may be too high for patients using beta blockers (Table 2, Fig. 1).
Physiological explanation
A parallel reduction of HR during cardiopulmonary exercise testing including resting values to the same absolute extent would result in an unchanged absolute value of HRR. In contrast, the same percentage of HRR would not result in the same percentage of HRmax. This can explain the difference of %HRmax using bisoprolol, but not of %HRR.
A second problem is that the relationship of HR to power output is not linear. Brooks et al. [6] and Foster et al. [8] critically noted the implications of the curvilinear relationship between HR and oxygen consumption during heavy exercise. Hofmann et al. [9] found different patterns for the HR workload relationship in healthy students. HRmax was not significantly different among groups, but %HRmax and HR at anaerobic threshold were different between groups, implying that the %HRmax method, based on a straight percentage of HRmax, was inaccurate in determining a comparable target HR. Similar to our group of subjects, percentage of maximal power output values were found to be much more stable than %HRmax values [9]. This was also shown for cardiovascular patients [10, 15] using metabolic and respiratory turn points as the reference set point. As we found non-significant but higher HR-differences at AeT and AnT between placebo and bisoprolol compared to resting and maximum values (Table 1, Fig. 1), we may suggest that the response of HR to power output changed during the cardiopulmonary exercise test. Our study shows that the physiological effort at AeT and AnT is not different with and without bisoprolol. A greater difference in HR at AnT than at maximal workload would lead to a more pronounced decline in HR with placebo relative to bisoprolol. This finding may be explained from the pharmacological point of view to be due to the competitive antagonism of beta-blockers [34]. It has been shown that there is no or only a slight increase in the catecholamines epinephrine and norepinephrine at low intensity levels but a sharp increase at the anaerobic threshold [30, 31, 35]. We argue that the high levels of catecholamines at highest workload reduce the efficiency of beta-blockers relative to lower intensity levels.
In our study, the subjective perception of exercise was not significantly different at AeT and AnT, indicating that rating of perceived exertion values are valid indicators of exercise intensity in young male subjects [23] using a beta-blocker, as also shown for hypertensive patients [18]. Although there was a slight increase for ratings of perceived exertion at AnT with bisoprolol, this difference did not reach statistical significance. Assuming a true difference in ratings of perceived exertion at AnT, exercise prescription based on ratings of perceived exertion as suggested by some authors [1, 18, 23] would further decrease the %HRmax and %HRR. Therefore, patients can safely engage in exercise as long as they exercise within prudent and prescribed levels of intensity using ratings of perceived exertion.
One criticism is that only young healthy subjects, who are not normally treated with beta-blockers, were investigated in this study. However the pharmacological mechanisms of cardioselective adrenoceptor blockade are similar in patients and healthy subjects with regard to the HR response. Furthermore, it has been shown that the effects on exercise haemodynamics and maximal exercise capacity tolerance obtained in normotensive subjects are comparable to the effects in hypertensive patients [36]. It has also been shown that the maximal sustainable workload was not different for beta-blockade and calcium-antagonism for hypertensive patients [18] and healthy subjects [25]. Therefore, studying the effect of various anti-hypertensive medications on exercise tolerance in healthy volunteers is seen as an adequate methodology [23].
Conclusion
A training prescription using the %HRmax or %HRR method is dependent on the relationship of HR to workload and oxygen consumption, respectively. Chronic beta-blockade changes this relationship. Although %HRmax and %HRR concepts are attractive and easily applied, we suggest that determination of the aerobic and anaerobic thresholds is more accurate for the prescription of training intensities. The percentage of maximal oxygen uptake and maximal workload method or ratings of perceived exertion may be suggested as optional methods. Alternatively, the %HRmax or %HRR method should be modified for patients using beta-blockers, especially with respect to the upper limit of exercise training intensity.