
Abstract
Background
Vascular mortality is increasing in economically developing countries but reliable data about the determinants of cardiovascular disease are few. The International Collaborative Study of Cardiovascular Disease in Asia (InterASIA) was designed to obtain precise estimates of cardiovascular risk factor levels in the adult population of Thailand.
Design
A complex sample survey.
Methods
Data from a structured questionnaire, brief physical examination and a blood sample were collected from 5305 individuals aged 35 years or older (response rate 68%). Mean risk factor levels were calculated for eight groups defined by age and sex in 18 representative urban and rural areas of Thailand. Population risk factor levels were calculated by applying sampling weights derived from the 2000 Thai Census and allowing for the complex sampling design.
Results
The estimated mean (standard error) population blood pressure was 120/76 (0.7/0.5) mmHg, mean serum total cholesterol was 5.2 (0.06) mmol/l, mean body mass index was 24 (0.2) kg/m2, mean fasting plasma glucose was 5.6 (0.06) mmol/l, the proportion with diabetes 9.6 (1)% and the proportion of current smokers was 25 (3)%. There were estimated to be 5.1 (0.5) million individuals with high blood pressure, 4.4 (0.4) million with high total cholesterol, 8.9 (0.8) million overweight or obese, 2.4 (0.2) million with diabetes and 6.2 (0.9) million current smokers. Mean levels of all major risk factors, except smoking, were worse in urban compared with rural areas. However, except for total cholesterol, the absolute numbers of individuals with abnormal risk factor levels were highest in rural areas.
Conclusions
Absolute levels of cardiovascular risk factors in Thailand are high. Effective risk factor control strategies that target both rural and urban areas of Thailand have the potential to avert much premature cardiovascular disease. Eur J Cardiovasc Prevention Rehab 10:249–257 © 2003 Lippincott Williams & Wilkins.
Keywords
Introduction
Cardiovascular diseases are the leading causes of death worldwide, accounting for an estimated 14 million deaths in 1990, the majority of which (9 million) occurred in economically developing countries [1]. While there is evidence that cardiovascular disease rates have ceased to rise in some high-income countries [2–4] deaths from cardiovascular causes are increasing in most other populations. It is estimated that, worldwide, 25 million people will die from cardiovascular diseases each year by 2020, and that an even larger proportion of these deaths (19 million, 76%) will occur in low- and middle-income countries [1].
Over the last few decades, cardiovascular diseases have emerged as a leading cause of death in Asia, in large part because of rapid economic growth, urbanization and ageing of the population [5, 6]. Coronary heart disease has been the leading cause of death in Thailand since 1989, and coronary mortality rates have increased each year since then [7]. By 1998, cardiovascular diseases accounted for over 54,000 deaths in Thailand (17% of the estimated 318,000 total deaths) [8].
Precise data about the determinants of cardiovascular diseases may greatly facilitate the development of appropriate strategies for prevention, but few such data exist for Thailand. The International Collaborative Study of Cardiovascular Disease in Asia (InterASIA) was designed to obtain estimates of the levels of major cardiovascular risk factors, and the prevalence of vascular diseases, among representative samples of the adult populations of Thailand and the People's Republic of China. This report summarizes the principal findings about cardiovascular risk factors in the Thai component of the study.
Methods
InterASIA was conducted collaboratively between academic institutions in Australia, China, Thailand and the United States of America (see Acknowledgements). The Thai component of the study was approved by the Institutional Review Board at Mahidol University, Bangkok and by the local ethics committee at each of the collaborating centres in Thailand. All participants provided written, informed, consent and the study was conducted in line with the Declaration of Helsinki and subsequent amendments. Data collection was conducted between May and October 2000.
Details about Thailand
Thailand comprises the capital, Bangkok and four regions (North, South, Northeast and Central Thailand), each made up of a number of provinces (Fig. 1). Bangkok and each regional province are further divided into political districts, which, in turn, are made up of enumeration districts (EDs). In urban areas, EDs are based on city blocks and are classified on socio-economic grounds as slum or non-slum. Similarly, in rural areas, EDs are based upon village units and are classified as undeveloped, developing or developed. Classification of the development status of urban and rural EDs is based on comprehensive development criteria defined by the Department of Community Development of the Thai Ministry of the Interior (http://www.porchor.moi.go.th/N2C/N2c4.html). Based on the 2000 Thai National Population and Housing Census [9], the total population of Thailand was estimated to be 60.6 million, of whom 25.0 million people were aged 35 years or older. Among those aged 35 years or over, the mean age was 50.3 years, 52% were female and 69% lived in rural areas.
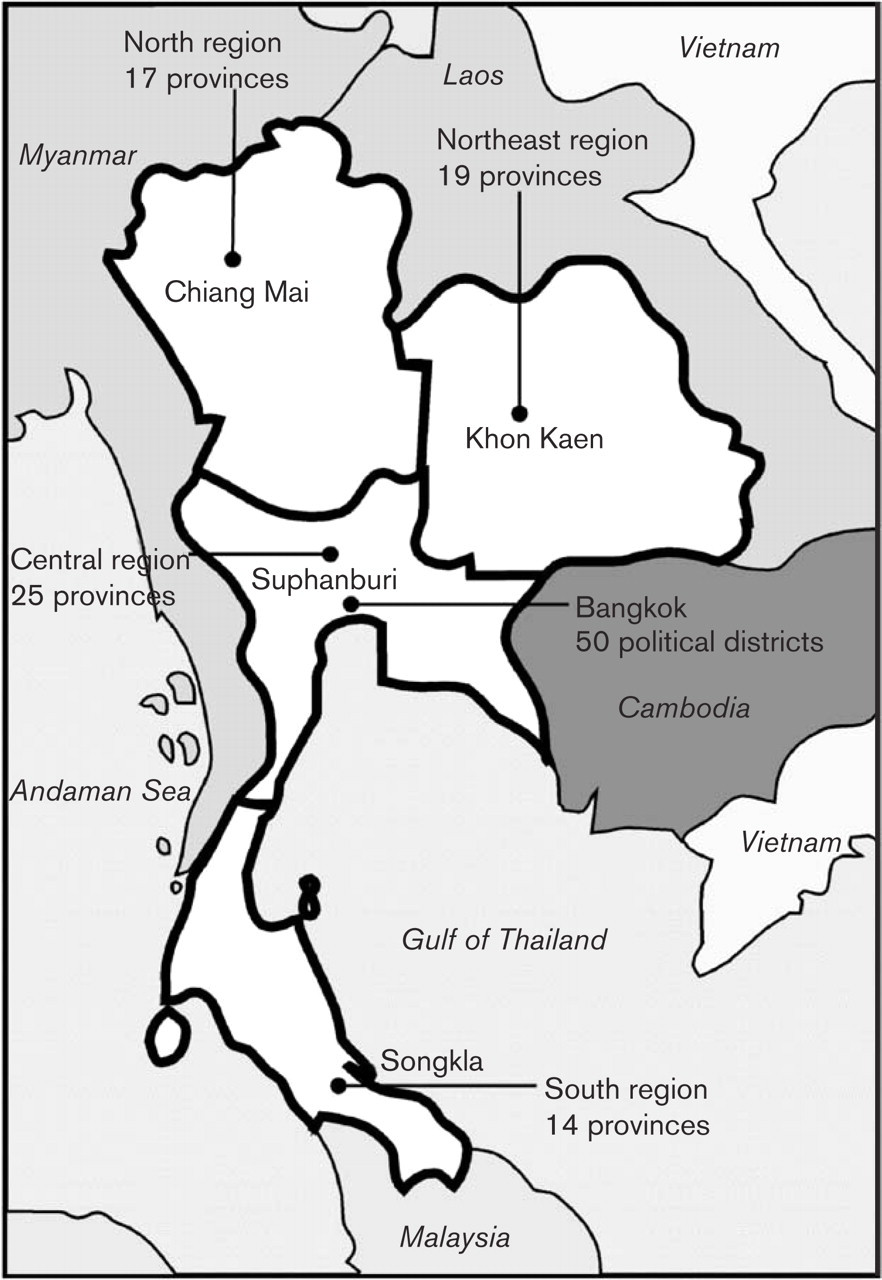
Administrative regions of Thailand showing the location of selected provinces. Lines point to the location of Bangkok and the selected province in each region.
The sample design
One representative province was selected from each of the four regions of Thailand (Fig. 2). From these provinces and Bangkok, a total of five representative urban political districts (one from Bangkok and one from each chosen province) and four representative rural political districts (one from each chosen province) were selected. Finally, up to six representative slum EDs and up to three representative non-slum EDs were selected from each urban political district (except in Central Thailand where there were no slum EDs in the selected urban district) and up to three representative developing and three representative developed EDs were selected from each rural district. Additionally, in North Thailand, the only region in which the selected rural district included undeveloped EDs, two representative undeveloped EDs were selected. At each level, selection of the units for sampling was based on their broad socio-demographic representativeness in the view of the Thai investigators (S.C. and P.S.), with additional consideration given to the potential of the sites for participation in future longitudinal surveillance studies. The number of EDs of each development level selected from each district was dependent upon the population size covered by each ED. Within the selected EDs of a given development level in each district, the population aged 35 years and over was grouped by age (35–44, 45–54, 55–64 and ≥ 65 years) and sex, using lists compiled from local government registers of households. These registers were updated for the census the previous year. Individuals were then sampled at random from each age and sex group with the goal of recruiting a similar number of people from each, under the proviso that only one individual be recruited from a household.
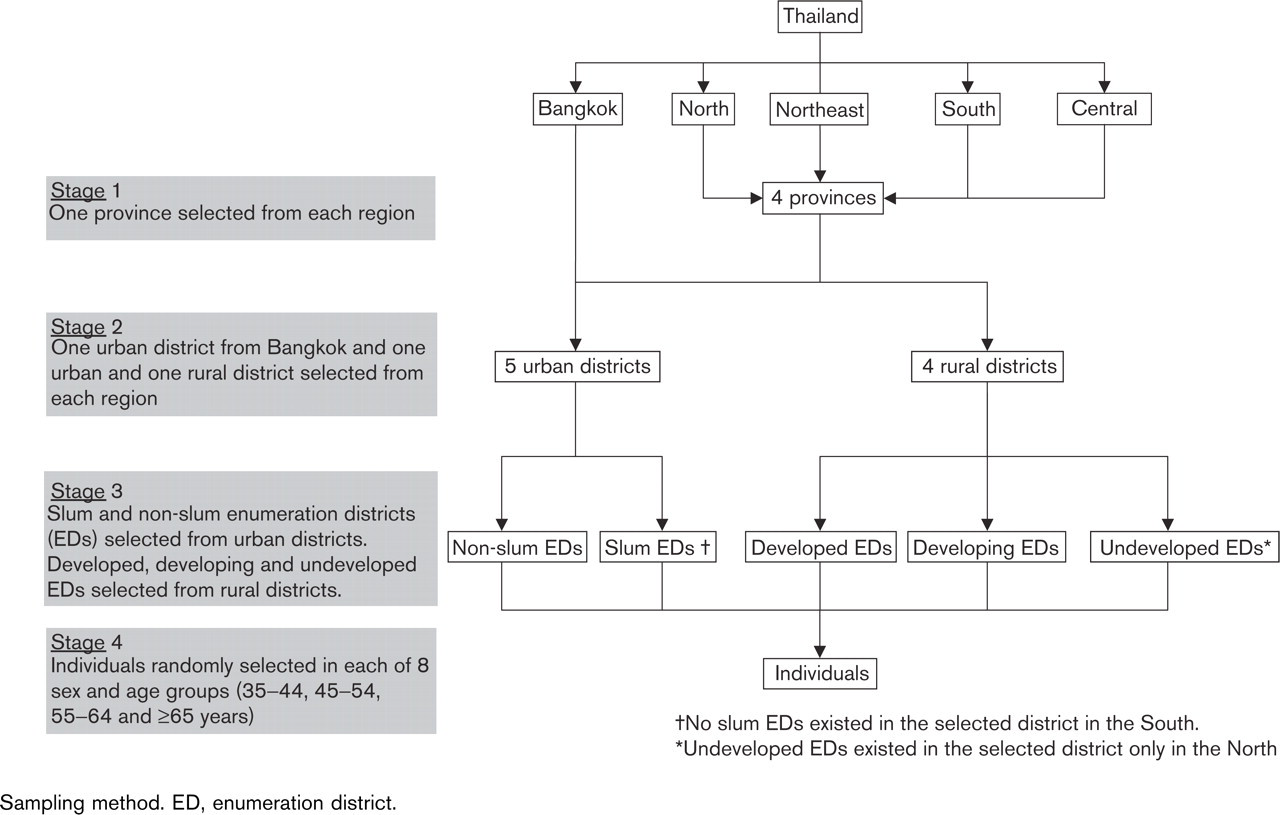
Sampling method. ED, enumeration district.
Data collection and measurements
For each individual who agreed to participate, trained study staff administered a structured questionnaire, performed a brief physical examination and collected a fasting blood sample. The questionnaire sought information about basic socio-demographic variables (including education level, household income and occupation), cardiovascular risk factors, history of cardiovascular diseases, current treatments and behavioural characteristics. The examination included three measurements of blood pressure, made according to American Heart Association recommendations (with systolic and diastolic pressures taken as the first and fifth Korotkoff sounds, respectively) [10], and measurement of body weight and height with participants wearing indoor clothes without shoes.
Venous blood samples for biochemical analysis were obtained after an 8-h overnight fast. Samples were stored immediately in ice, and centrifuged and separated on the day of collection. Sera were subsequently frozen and transferred on dry ice to a central laboratory (Faculty of Medicine, Ramathibodi Hospital, Bangkok) where they were stored at −70°C until analysed. All analyses were performed using a Dimension RxLHM clinical chemistry system (Dade Behring Inc, New York, USA). Serum total cholesterol and high-density lipoprotein (HDL) cholesterol were measured using enzymatic and homogeneous methods, respectively [11, 12]. The laboratory was standardized according to the criteria of the Centers for Disease Control - National Heart, Lung, and Blood Institute Lipid Standardization Program [13]. Plasma glucose levels were measured using the hexokinase-glucose-6-phosphate dehydrogenase method [14].
Definitions
High blood pressure was defined as mean systolic blood pressure ≥ 140 mmHg and/or mean diastolic blood pressure ≥ 90 mmHg [15], and/or treatment with anti-hypertensive medication during the previous 2 weeks. High total cholesterol was defined as fasting serum cholesterol ≥ 6.2 mmol/l (240 mg/dl) [16], and/or treatment with lipid-lowering drugs during the previous 2 weeks. Diabetes was defined as fasting plasma glucose ≥ 7.0mmol/l (126 mg/dl) [17] or a previous diagnosis of diabetes. Overweight was defined as body mass index (BMI) ≥ 25kg/m2 but < 30kg/m2, and obesity as BMI ≥ 30kg/m2 [18].
Statistical methods
Estimates (with standard errors) of mean, or percentage, risk factor levels in the overall population aged 35 years and over, and among age, sex and rural/urban sub-groups of that population, were calculated. Comparisons of risk factor levels between population sub-groups were performed using t-tests for continuous variables and χ2-tests for categorical variables. Age trends were investigated using linear regression models. All analyses allowed for the complex survey design, using STATA 7.0 statistical software (StataCorp, College Station, Texas, USA): enumeration districts were taken as primary sampling units, eight strata were defined by four age groups and sex, and weights were the population [9] to sample size ratios for each combination of age, sex and type of enumeration district.
Results
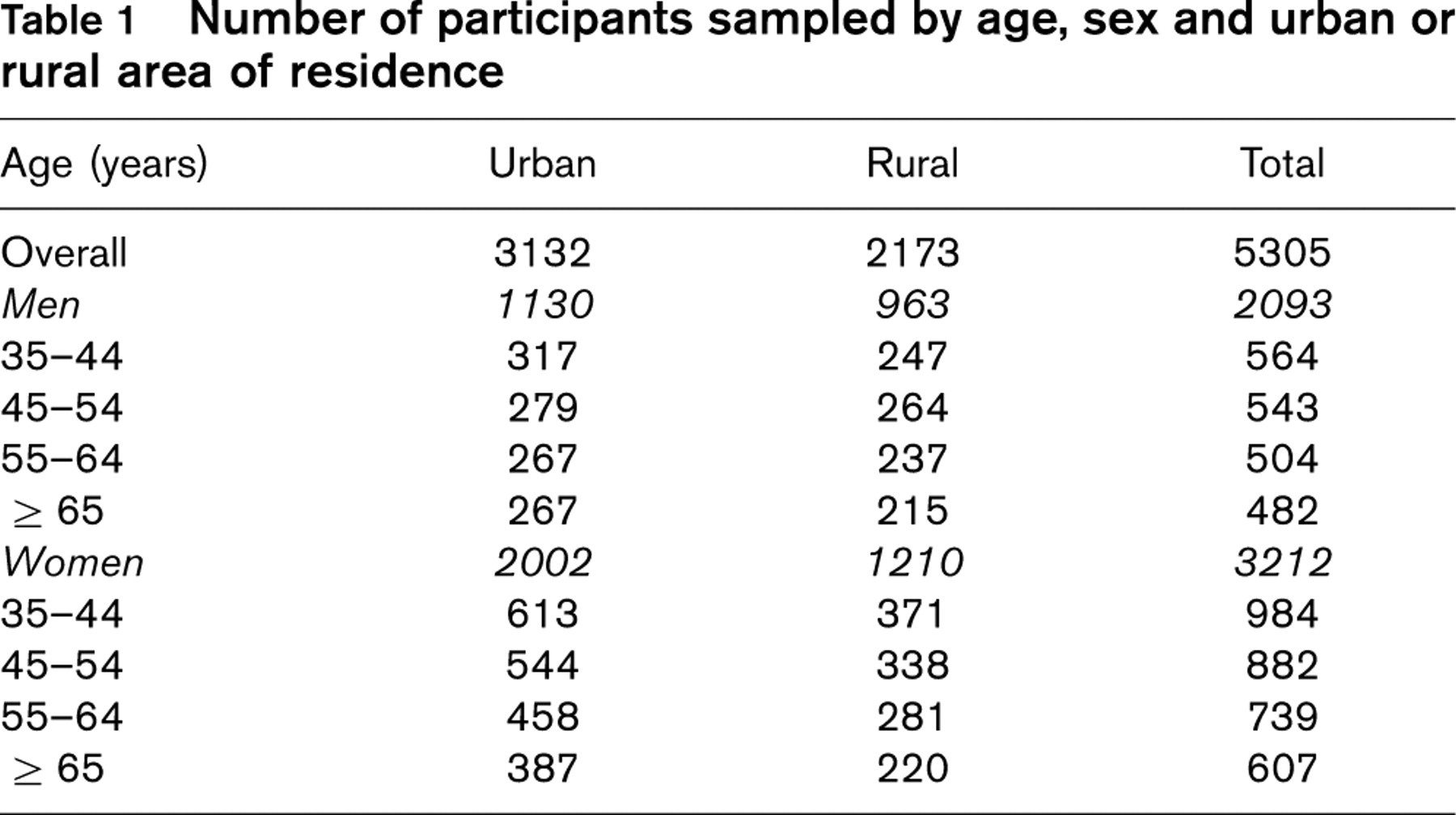
A total of 7909 individuals were invited to participate in the study, of whom 5350 (68%) agreed to participate and provided informed consent. Forty-five were subsequently excluded because their age was found to be less than 35 years on the day of assessment. Among the remaining 5305 participants (Table 1) the data from the questionnaire, anthropomorphic and blood pressure measurements were more than 99% complete, but no usable blood sample was available from 193 (4%) individuals. Between 215 and 613 individuals were sampled in each of the 16 age-, sex- and urban-rural area of residence-specific population groups. The response rate was higher in rural than urban areas (81 versus 61%, P < 0.001) and among females than males (77 versus 57%, P < 0.001), but did not significantly differ by age group (P = 0.6).
Levels of major vascular risk factors in Thai adults aged 35 years or over
Blood pressure
The estimated overall mean blood pressure was 120/76 mmHg (Table 2). Mean systolic blood pressure did not differ between men and women (P =0.4), but mean diastolic blood pressure was higher in men (P = 0.01). Mean levels of systolic and diastolic blood pressure appeared higher among individuals living in urban compared with rural areas (P =0.06 and P < 0.001, respectively) (Table 3 and Fig. 3). Mean systolic blood pressure increased with age group among both men and women and in both urban and rural areas (all P < 0.001). Diastolic blood pressure was, however, highest among those aged 45–54 years in both sexes and in both urban and rural areas. Among individuals aged 35 years or over, the prevalence of high blood pressure was estimated to be 21% (representing 5.1 million people) (Table 4). There was no evidence of a difference in the prevalence of high blood pressure between men and women (21 versus 20%, 0.6). While the proportion of individuals with high blood pressure was greater among urban than rural populations (26 versus 18%, P = 0.02), the estimated absolute number of individuals with high blood pressure was greater in rural than urban populations (Table 4).
Number of participants sampled by age, sex and urban or rural area of residence
Total cholesterol
The estimated mean level of serum total cholesterol was 5.19 mmol/l (Table 2). Mean total cholesterol levels were higher in women than men (P = 0.004) (Table 2) and among individuals living in urban compared with rural areas (both P < 0.001) (Table 3 and Fig. 3). An estimated 18% of the population had high total blood cholesterol levels, with greater proportions of women than men (21 versus 14%, P = 0.01), and urban than rural inhabitants (29 versus 12%, P ≤ 0.001) affected.
Glucose levels and diabetes
The estimated mean level of fasting plasma glucose was 5.55 mmol/l (Table 2). Levels did not differ between men and women (Table 2) (P = 0.3) but were higher among urban than rural inhabitants (P < 0.001) and among older compared with younger individuals (P < 0.001) (Table 3 and Fig. 3). The estimated prevalence of diabetes was 9.6% (Table 1), representing 2.4 million people (Table 4), half of whom were not previously aware of the diagnosis. The prevalence of diabetes was similar for both men and women (9 versus 10%, P = 0.5) but was greater among older individuals of both sexes (both P < 0.001). Diabetes was more common among urban than rural areas (12 versus 9%, P = 0.02) but the absolute number of individuals with diabetes was estimated to be greater in rural than urban populations (Table 4).
Estimated mean levels and prevalence of cardiovascular risk factors in the Thai population, aged 35 years or older, by age and sex group
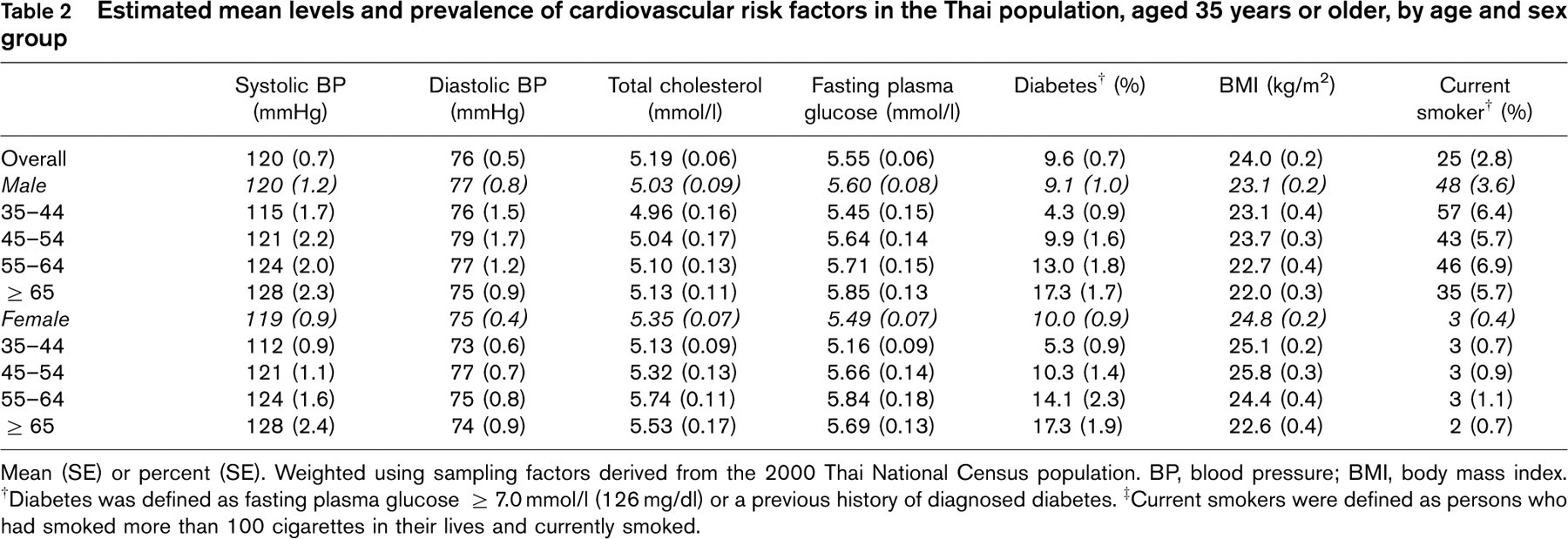
Mean (SE) or percent (SE). Weighted using sampling factors derived from the 2000 Thai National Census population. BP, blood pressure; BMI, body mass index. †Diabetes was defined as fasting plasma glucose ≥ 7.0 mmol/l (126 mg/dl) or a previous history of diagnosed diabetes. ‡Current smokers were defined as persons who had smoked more than 100 cigarettes in their lives and currently smoked.
Estimated mean levels and prevalence of cardiovascular risk factors in the Thai population, aged 35 years or older, by age and sex group in urban and rural areas
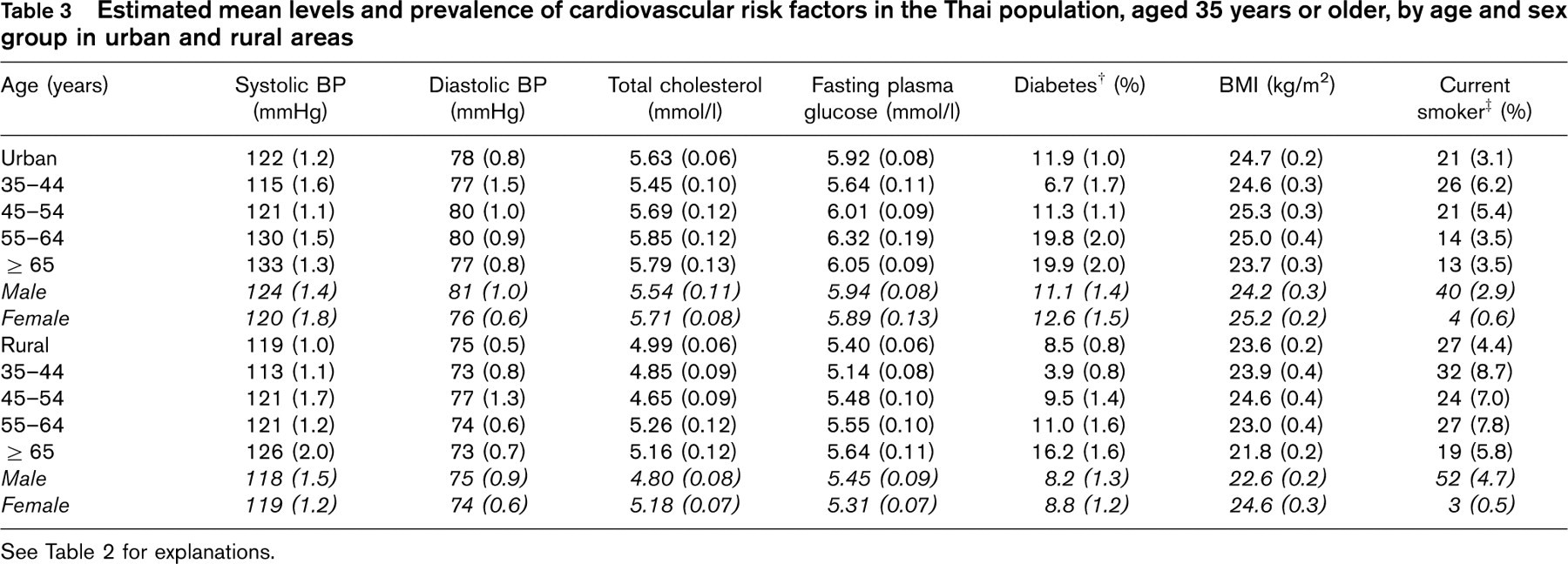
See Table 2 for explanations.
Body mass index and obesity
The estimated mean body mass index (BMI) was 24.0 kg/m2 (Table 2). BMI was higher among women than men (Table 2), and among populations living in urban compared with rural settings (Table 3 and Fig. 3) (both P < 0.001). BMI was greatest in the 45–54 year age groups in both sexes and in both urban and rural populations. The national prevalence of overweight or obesity among those aged 35 or over was estimated to be 36% (representing 8.9 million people) (Table 4). Overweight or obesity was more frequent among women than men (43 versus 28%), and among urban than rural inhabitants (43 versus 33%), (both P < 0.001).
Cigarette smoking
The estimated percentage of current smokers was 25% (Table 2). Smoking prevalence was much higher in men than women (48 versus 3%, P < 0.001) and was higher in rural than urban areas (27 versus 21%, P < 0.001) (Table 3 and Fig. 3). Among men, smoking prevalence was greater at younger ages (P < 0.001) but there was no clear association of age with smoking prevalence among women (P = 0.8). An estimated 6.2 million Thais, aged 35 years or older, currently smoke and 93% of these are male (Table 4). Only 26% of Thai men claimed to have never smoked, compared with 95% of women (P < 0.001).
Discussion
InterASIA is the most comprehensive and detailed survey of the levels of risk factors for cardiovascular disease that has yet been conducted in Thailand. The study clearly identifies major cardiovascular risk factors to be highly prevalent among the adult Thai population, with patterns of risk factor prevalence broadly in line with those anticipated for a country undergoing rapid economic development [5, 6]. While the average levels of most cardiovascular risk factors remain below those typically observed in Western populations [19–21], the likely further deterioration in the risk factor profile of the average Thai adult suggests an urgent need for investment in strategies for risk factor control and disease prevention [5, 6]. In other countries that have experienced an epidemic of cardiovascular diseases, effective strategies for treatment and prevention are believed to have done much to ameliorate the burden of serious fatal and non-fatal vascular events [22, 23].
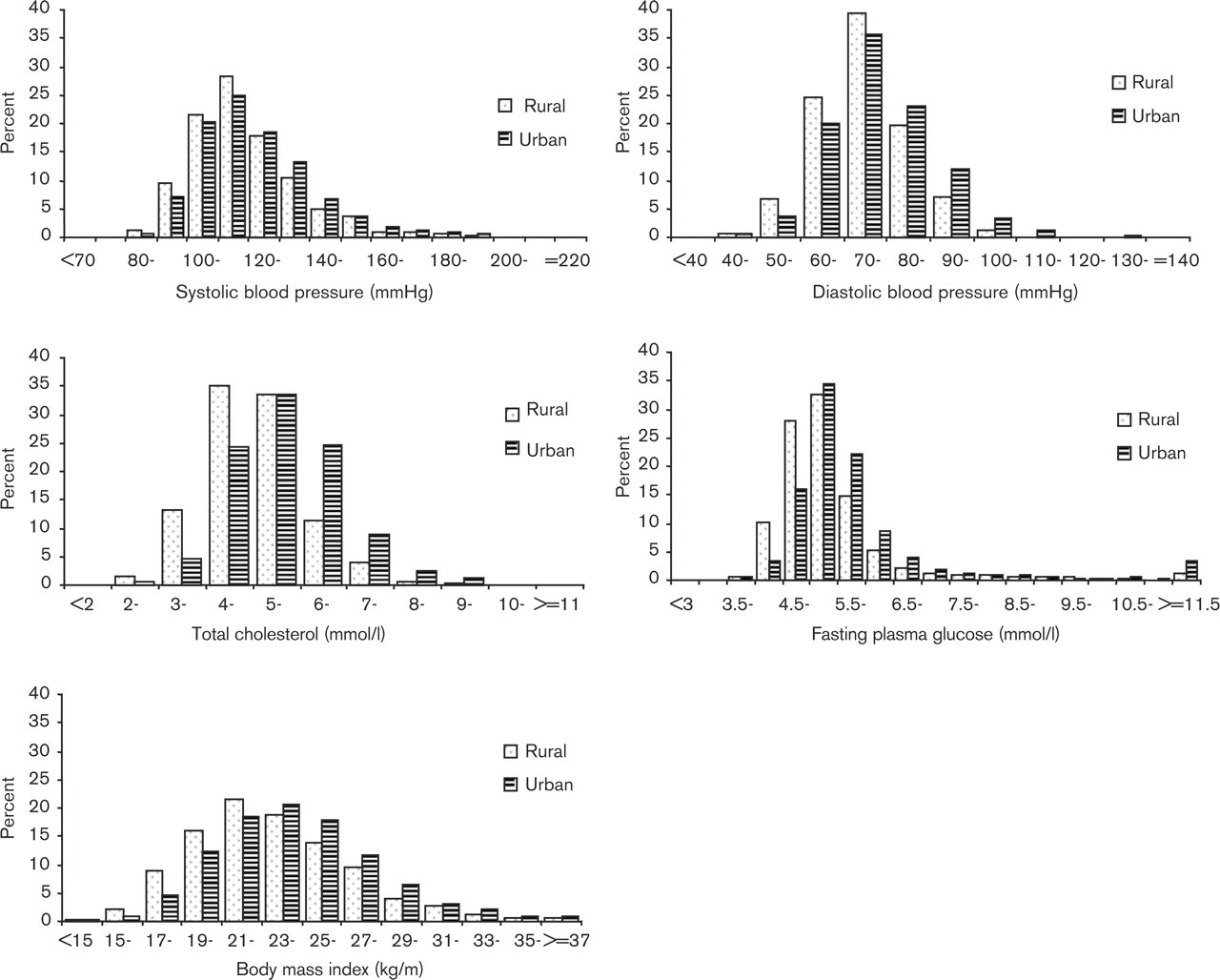
Distributions of estimated population levels of major cardiovascular risk factors by area of residence (urban or rural) in Thai adults, aged 35 years and older.
Estimated numbers (in millions) of individuals with major cardiovascular risk factors in the Thai population, aged 35 years or older
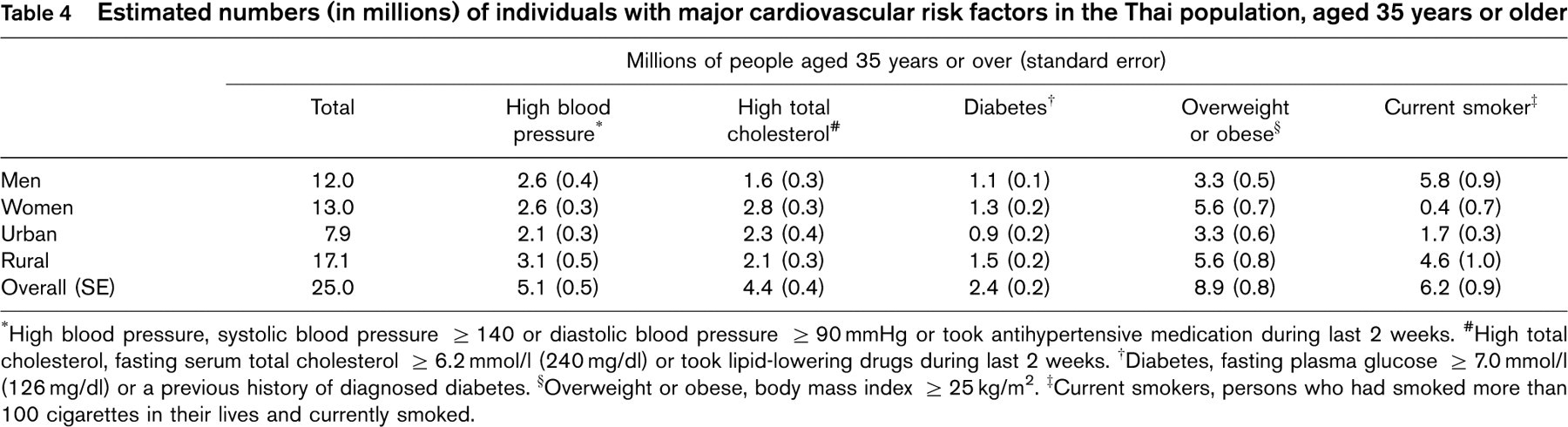
∗High blood pressure, systolic blood pressure ≥ 140 or diastolic blood pressure ≥ 90 mmHg or took antihypertensive medication during last 2 weeks. #High total cholesterol, fasting serum total cholesterol ≥ 6.2 mmol/l (240mg/dl) or took lipid-lowering drugs during last 2 weeks. †Diabetes, fasting plasma glucose ≥ 7.0 mmol/l (126 mg/dl) or a previous history of diagnosed diabetes. §Overweight or obese, body mass index ≥ 25 kg/m2. ‡Current smokers, persons who had smoked more than 100 cigarettes in their lives and currently smoked.
There were clear differences in the patterns of risk factors between Thai populations living in urban compared with rural environments. For blood pressure, total cholesterol, obesity and glucose/diabetes, mean risk factor levels and prevalence rates were worse among the residents of urban areas, whereas smoking rates alone were worse in rural populations. However, while the cardiovascular risk factor levels of rural populations were, on average, rather better than those of urban populations, the absolute numbers of individuals with high blood pressure, overweight, obesity or diabetes were all greater in rural than urban regions, reflecting the large proportion of the Thai population that live in a rural setting. As well as urban/rural variation in risk factor levels, there were also some differences in the risk factor profiles of men compared with women, and older compared with younger individuals. Men had higher mean levels of blood pressure and glucose, and a greater prevalence of both diabetes and smoking, whereas women tended to be more obese and had higher total cholesterol levels. Diabetes, and elevated levels of blood pressure, total cholesterol and glucose were each more frequent among older individuals, whereas obesity and smoking were more frequent among younger people. Differences between the age and sex structure of the urban and rural populations in Thailand are small and do not explain the observed urban-rural differences in risk factor levels. It is likely, therefore, that the variation reflects behavioural differences relating to factors such as nutrition and exercise, as appears to be the case for many other populations [5, 6].
The InterASIA study was designed to ensure that reliable estimates of risk factor levels were obtained for both the Thai population as a whole and for major demographic subgroups. Staff training, monitoring and standardization of all practical procedures, including biochemical analyses, should have resulted in reliable measurements being obtained for the individuals included in the study. In addition, the large size of the study ensured that the overall estimates of risk factor levels were reasonably precise and the good response rates achieved for most sections of the population should have minimized biases both overall and in population subgroups. However, economic and practical constraints on the design of the study have resulted in some drawbacks. Ideally, each stage of sampling should have been completely random, but instead ‘representative’ EDs, suitable for research purposes, were selected by the chief Thai investigators, and this could have led to biases in the point estimates (means and prevalences). Additionally, the complex study design involved non-random, stratified selection of single provinces within regions and single EDs, of particular types, within selected provinces (Fig. 2). This makes calculation of standard errors impossible at the initial levels of sampling and we were, thus, only able to take account of clustering at the ED level of sampling. The reported standard errors will therefore tend to be rather larger than they should. It appears unlikely, however, that the absolute estimates of risk factor levels are seriously biased. Furthermore, while quantitative errors in the magnitude of the differences between population subgroups may be present, it is unlikely that qualitative misrepresentations of risk factor patterns have been made. Comparison of the InterASIA findings with earlier National Health Examination Surveys and other cross-sectional studies in Thailand [24–34] does suggest changes in the absolute levels of risk factors over time. For example, the proportion of the population that smokes tobacco appears to have fallen and the prevalence of high blood pressure, high total cholesterol, diabetes and obesity all appear to have risen. However, the patterns of risk factors in urban compared with rural populations, men compared with women and between people of different ages appear to be broadly comparable across InterASIA and these previous studies. This comparability provides substantial reassurance that biases are unlikely to be a major problem in our study.
In large part, the changes in the absolute levels of cardiovascular risk factors suggested by comparisons to previous studies [24–34] are likely to have been driven by major socio-demographic change over the intervening period, particularly urbanization and ageing of the population. These generally adverse trends seem likely to continue: by 2010 the proportion of the Thai population living in urban environments is projected to rise to 40%, from a 1990 level of 30%, and the proportion of the population aged 60 years or over is expected approximately to double [7, 9]. The previously reported [35], and here confirmed, decline in the prevalence of smoking in Thailand appears to be attributable to the institution of comprehensive legislative measures for tobacco control and a major public education campaign. These measures included a ban on advertising and other promotion of cigarettes, a ban on smoking in public places and a requirement for warning labels on cigarette packets. The participation of the international community in new measures, such as the exclusion of cigarettes from the list of commodities destined for decreased import tax under regional trade agreements, will be key to the continued success of such efforts.
There are many proven means of preventing and treating cardiovascular disease, although most evidence about such strategies derives from studies conducted in high-income industrialized populations from Europe and North America. However, the determinants of cardiovascular disease in Asian populations appear very similar to those in Western populations and, in much of Asia, potentially modifiable risk factors such as blood pressure, blood cholesterol, smoking, obesity and diabetes appear to be leading contributors to both the current and projected cardiovascular disease burden [36–38]. As in the West, effective modification of these risk factors would be anticipated to avert much premature cardiovascular disease, although it is likely that risk factor management strategies developed for high-income countries will require substantial tailoring to the national and regional characteristics of Thailand. Thailand is presently undertaking a major reform of the public health system and the completion of the InterASIA study is, therefore, particularly timely. It is anticipated that the data provided by InterASIA will importantly inform the development of national strategies for the treatment and prevention of cardiovascular disease. In line with the recent recommendations provided in the 2002 World Health Report [39], these strategies could usefully comprise a combination of community based strategies, seeking to achieve population-wide shifts in risk factor levels, as well as approaches targeted specifically at high-risk individuals. Planned future surveys of the communities involved in InterASIA may also serve as a means of measuring the effectiveness of any policy interventions that are implemented, and further directing policy initiatives in the years to come.
Finally, in addition to providing specific data about risk factor levels in Thailand, the InterASIA study has demonstrated that the collection of high quality, nationally representative data about cardiovascular risk factors is possible in low- to middle-income countries with limited research infrastructure. It is likely that the methods used in this study could be applied to many other such countries, and that similarly reliable information could be obtained. Since low- and middle-income countries are anticipated to experience the greatest increases in cardiovascular disease over the next few decades, and information about risk factor levels in these countries is frequently minimal, such data would be of substantial importance. In particular, data of this type could greatly enhance the ability of governments to develop appropriate and effective national cardiovascular disease prevention and treatment strategies.
Footnotes
Acknowledgements
China: Chinese Academy of Medical Sciences, Beijing - Dongfeng Gu, Xiufang Duan, Guangyong Huang, Xigui Wu; Beijing - Yuefeng Ma; FuJian - Ling Yu; Guangxi - Yingnai Chen; Hubei - Ligui Wang; Jiangsu - CaiLiang Yao; Jiling - Lihua Xu; Qinghai - Ping Wang; Shandong - Fuqiang Chen; Shanxi - Jianjing Mo; Sichuan - Xianping Wu. Thailand: Mahidol University, Bangkok - Paibul Suriyawongpaisal, Sayan Cheepudomwit, Porntip Loelekla, Piyamitr Srithara; Bangkok - Poolsook Sariyaporn, Pairao Pongchoke, Somboon Jaiyavat, Charermsri Nantawan, Vachira Kasikoson; North - Somsak Thamthitiwat, Penprapa Siviroj, Jiraporn Suwanteerangkul; Northeast - Pyatat Tasanavivat, Pattapong Kessomboon, Sujinan Horas; South - Virasakdi Chongsuvivatwong, Tada Yipintsoi, Nualta Apakupakul, Walla Jirathamopas, Woravut Jintapakorn; Central - Vongsvat Kosulwat, Atitada Boonpraderm, Amornrat Wongchanapai, Chayanist Wanijjakul. United States: Tulane University, New Orleans, LA - Jiang He, Paul Whelton, Lydia Bazzano, Jing Chen, Paul Muntner, Kristi Reynolds, Xue Xin. Australia: Institute for International Health, University of Sydney - Neil Chapman, Sam Colman, Stephen MacMahon, Bruce Neal, Mark Woodward, Xin-Hua Zhang. Steering Committee: Jiang He (Co-Principal Investigator), Paul Whelton (Co-Principal Investigator), Dale Glasser, Dongfeng Gu, Stephen MacMahon, Bruce Neal, Rajiv Patni, Robert Reynolds, Paibul Suriyawongpaisal, Xigui Wu, Xue Xin, Xin-Hua Zhang. Writing Committee: Sayan Cheepudomwit, Neil Chapman, Jiang He, Bruce Neal, Paibul Suriyawongpaisal, Paul Whelton, Mark Woodward. Financial support: The InterASIA study was funded by a contractual agreement between Tulane University, LA, USA and Pfizer, Inc., NY, USA. Two researchers employed by Pfizer, Inc. were members of the Steering Committee that designed the study. However, the study was conducted, analysed and interpreted by the investigators independently of the sponsor.