
Abstract
Objective
Handbiking and wheelchair racing have gained increased popularity in Germany. This is important because of the inability of wheelchair-dependent people to maintain cardiovascular health and fitness through daily activities. The purpose of this study was to evaluate the energy expenditure (EE; kcal/h) of wheelchair-dependent individuals.
Methods
Ten wheelchair racers (WR) and 17 handbikers (HB) completed a basal metabolism evaluation, an incremental exercise test until exhaustion and an endurance test. Oxygen uptake and carbon dioxide production (
Results
In the endurance test
Conclusion
The results show that EE of HB and WR is high enough to maintain fitness and probably to help to prevent cardiovascular diseases even at a moderate intensity.
Introduction
Preventive medical measures are mainly based on extensive longitudinal investigations focusing on the relation of additional energy expenditure due to physical activity on the one hand and mortality and morbidity rates on the other [1–11]. These findings allow the deduction of corresponding recommendations for sport and physical exercise to minimize the risk of cardiovascular disease. According to the Harvard alumni study, an additional weekly energy expenditure of 2000 to 2500 kcal or an additional daily energy consumption of approximately 300 to 350 kcal minimizes the probability of myocardial infarction [5]. A precondition to putting these recommendations into practice in everyday life, however, is the quantification of the energy expenditure of physical activities as they exist for non-handicapped people for almost any conceivable physical activity [12]. Such recommendations do not exist for people dependent on a wheelchair. Experimental quantifications of the energy expenditure are not available and, consequently, any systematic, prospective longitudinal examination of the relation between energy expenditure and cardiovascular mortality and morbidity cannot yet be performed. Examinations of the energy expenditure in various wheelchair sports are thus the imperative prerequisite for investigating the outlined interactions. In view of the increased life expectancy and the elevated risk of atherogenic diseases due to a forced low-exercise lifestyle in connection with a lower muscle mass as compared with non-handicapped people, and the associated lower energy expenditure, such examinations are of elementary importance [13]. Therefore, the aim of this study was to gain data concerning energy expenditure of wheelchair-dependent individuals in the sports of handbiking and wheelchair racing.
Aim of the study
The aims of the study were to determine the load-induced energy expenditure in two selected, endurance-focused, classical wheelchair sports at different intensities. Furthermore, we wanted to determine the level of training required in the field of wheelchair sport to reach recommended energy expenditure values, and the weekly energy expenditure value of the study group provoked by their physical activity.
Method
Twenty-five athletes with spinal cord injuries (wheelchair racing: seven paraplegically and three quadriplegically, handbiking: 11 paraplegically and four quadriplegically handicapped) and two athletes with amputations of both legs took part in the investigation after having given their written consent to participate in the present study. Anthropometric data are given in Table 1.
Six women and 21 men took part in the investigation. Fifteen of the participants were members of an established national handbike team or the national wheelchair race team, 12 were performance or leisure sport orientated, training for city marathon events. The handbiking athletes were mostly active in endurance-focused competitions whereas most of the athletes in the wheelchair racing group took part in sprint races. In 19 athletes the handicap was due to a traumatic spinal cord injury, two individuals suffered from spina bifida, one from poliomyelitis and two had had both legs amputated. For three participants the spinal cord injury was due to other neurological or vascular causes. On average the athletes had been wheelchair dependent for 14.6 ± 6.1 years and they had been active in wheelchair sports for 10.4 ± 4.5 years. The weekly all-sport activity time was 8.9 ± 3.0 h with a duration of handbike specific training of 5.9 ± 3.3 h and wheelchair racing of 6.7 ± 2.9 h, respectively.
Prior to exercise, medical history was recorded, blood samples were taken and a 12-channel ECG at rest was performed. The resting oxygen uptake and carbon dioxide production was measured using the Deltatrac system (Deltatrac MBM-200, Datex-Engström, Achim, Germany) for not less than 30 min in a supine position after an overnight fasting period. Energy expenditure was measured by indirect calorimetry using the following equation [14]:
Based on the results of the examination, a decision was made with regard to the suitability of the subjects to take part in the study. During the incremental pretest a stress ECG was plotted.
During the incremental pretest all participants were encouraged by the investigator to reach maximum load One criterion of maximum load was a minimum value of 17 on the scale of perceived exertion according to Borg. This value on a scale from 6-20 indicates a subjectively perceived feeling of the effort of ‘very hard’ [15].
The incremental pre-exercise test until exhaustion was carried out to detect the heart rates corresponding to a blood lactate concentration of 2 and 4 mmol/l. These calculated heart rates were used for assessing the intensities of the following endurance tests. Between both tests there was a resting period of 2 h in which the participants were asked to drink carbohydrate loaded fluids in order to avoid glycogen depletion.
Anthropometric data of the test group

M, Male;
F, Female.
Protocol pretest
For the handbikers the tests were performed with the participants sitting in their own handbike which was connected to an ergometer (Cyclus II, Richter, Leipzig, Germany). Due to technical requirements this was necessary although we preferred using the same equipment as during the endurance test. The initial load was 15 watts increasing by 15 watts every 3 min until exhaustion of the participants. The athletes were asked to maintain a crank rate of not less than 60 rpm. Falling short of 50 rpm led to the termination of the test by the investigator. During the tests respiratory gas exchange values were continuously evaluated by an open circuit spirometric system (Oxycon alpha, Jäger, Würzburg, Germany). A capillary blood sample was taken during the last 30 s of each load stage to determine lactate values. Heart rate was also measured at that time, and individual perception of exhaustion was recorded.
For the group of the wheelchair racers the pretests were performed with the racers sitting in their own race wheelchair fixed on a treadmill. The initial speed was 5 km/h, increasing by 1 km/h every 3 min. Respiratory gas exchange values, heart rate and lactate values were measured as described for the group of the handbikers.
Protocol endurance test
The endurance tests were carried out on the treadmill for both types of sport. After a 5-min adaptation time to adjust to the settings, 20 min were at an intensity of a heart rate corresponding to 2 mmol/l lactate in the incremental pretest, being directly followed by a second time unit of 20 min at an intensity of a heart rate corresponding to 4 mmol/l lactate in the incremental pretest (Figure 1 a and b). These intensities represent a moderate aerobic work load (2 mmol/l) and a high load (4 mmol/l) at the lactate threshold defined by Mader et al. [16]. During the endurance test the spirometric data and the heart rates were continuously registered. Blood samples to determine the lactate concentration were taken every 5 min.
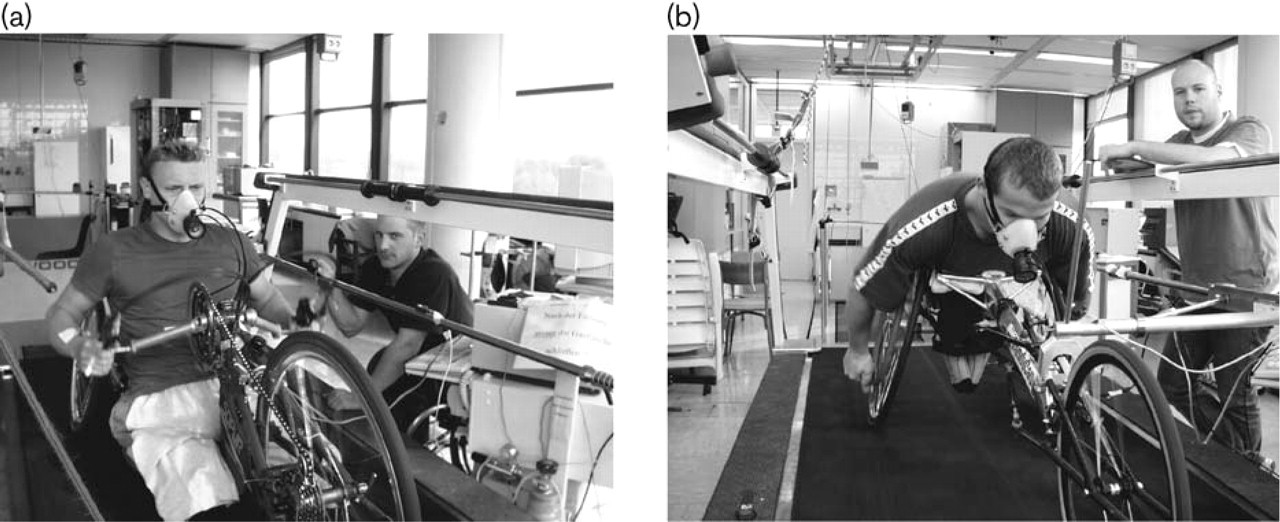
Endurance test in handbiking (a) and wheelchair racing (b) on the treadmill.
Statistical analysis
Analysis was performed using STATISTICA for Windows Version 5.1 F (StatSoft Inc, Tulsa, USA). The effects between both groups were determined by an unpaired t-test. A one-way ANOVA for repeated measurements was performed to test the individual values of each group during the time intervals. Post hoc analysis was performed to test whether the interactions were significant. A P-value less than 0.05 was considered significant.
Results
In the basal metabolism test the energy expenditure in handbikers was 65.4 ± 14.1 kcal/h, and in wheelchair racers 60.3 ± 9.1 kcal/h. For the endurance test the values of
The mean value of the measured energy expenditure at rest was 63.4 ± 12.2 kcal/h and 1521.6 ± 294.0 kcal/day, respectively, for the athletes of both groups. The energy expenditure calculated according to the equation recommended by the WHO, taking the anthropometric data of the athletes such as age, weight and sex into account, however, was 74.2 kcal/h [18]. The mean value of energy expenditure of all wheelchair-dependent athletes was 371.8 ± 97.5 kcal/h for the time interval with moderate intensity, and 498.8 ± 98.88 kcal/h for the high intensity period. There were no significant differences between the two kinds of sport concerning energy consumption during the two time intervals.
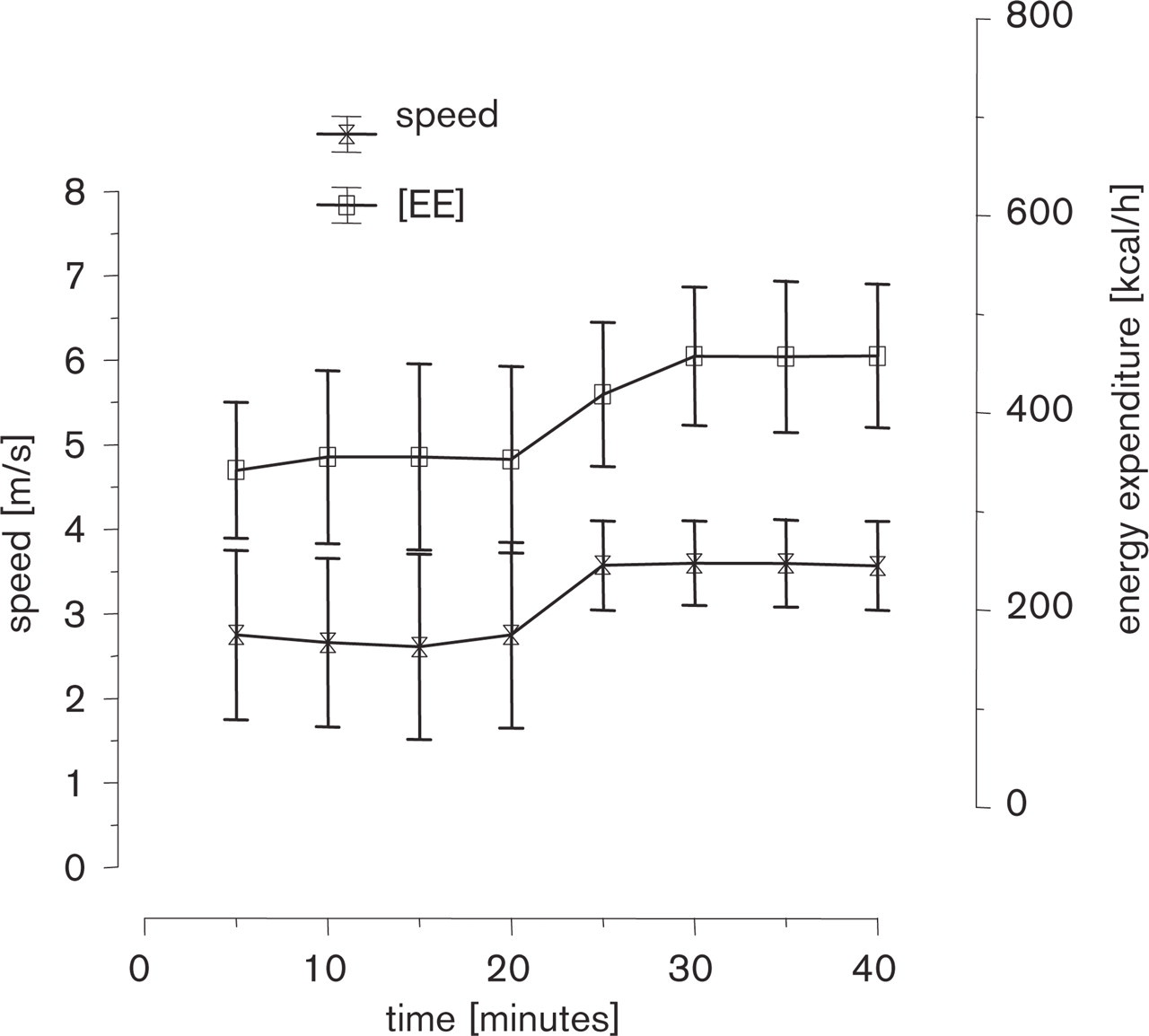
Means and standard deviation of the energy expenditure (EE, kilocalories per hour) and speed (metres per second) during the endurance test with two different intensities for the group of the handbikers.
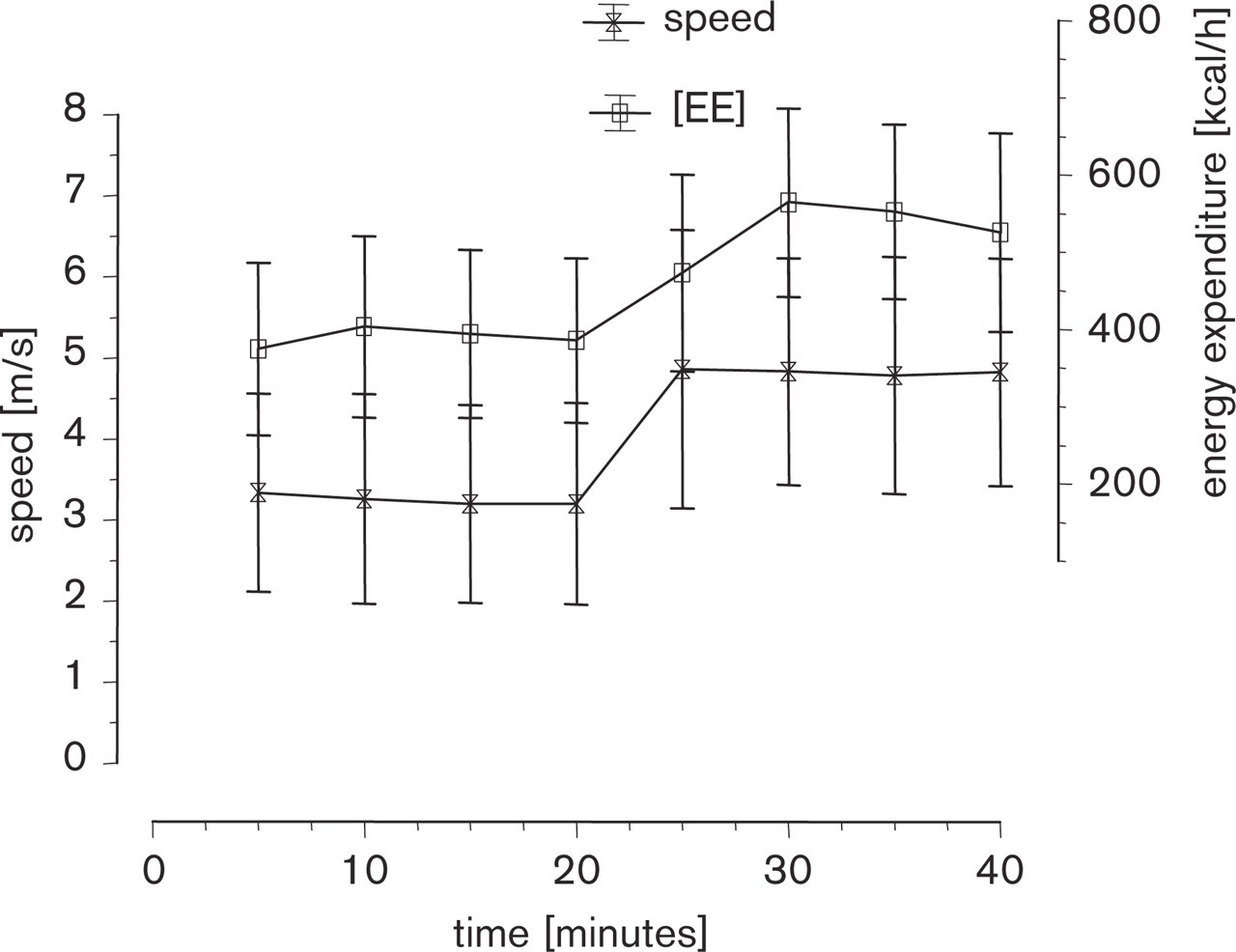
Means and standard deviation of the energy expenditure (EE, kilocalories per hour) and speed (metres per second) during the endurance test with two different intensities for the group of the wheelchair racers.
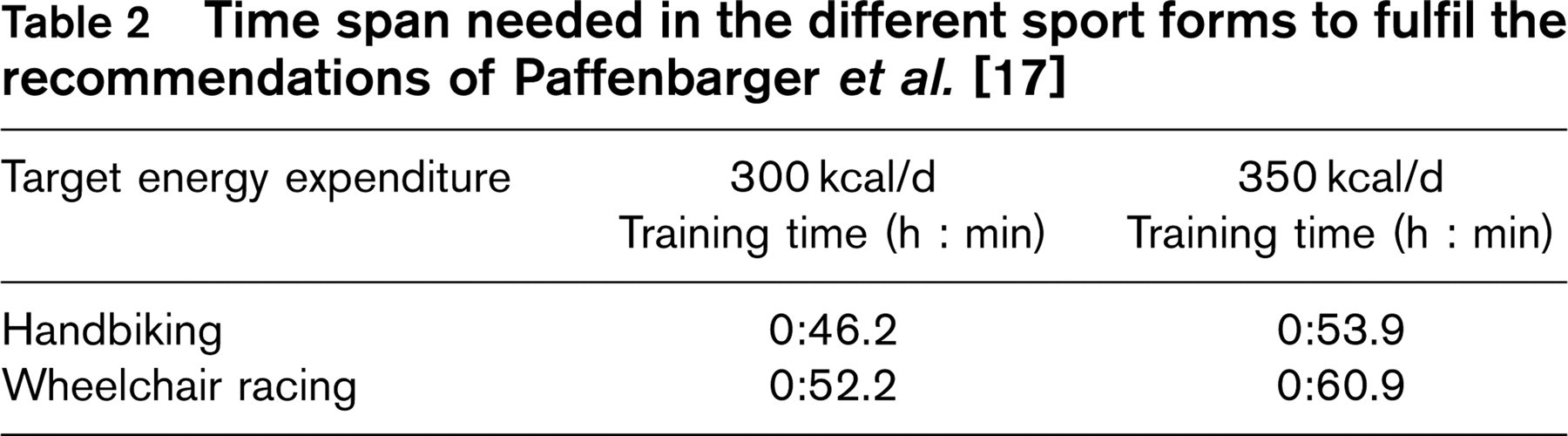
Time span needed in the different sport forms to fulfil the recommendations of Paffenbarger et al. [17]
The lactate values showed no significant differences between the two groups, neither with moderate nor with intensive load. The value of subjective load perception during the lower intensities was 12-13 on the scale according to Borg [15] (very, very easy = 7, very, very hard = 20), which corresponds to an assessment of ‘moderately hard'. For the high intensity, the ‘Borg value’ was 15-16. The mean values of heart rates for both intensities differed significantly between both sports with higher values in the wheelchair racers.
Discussion
Energy expenditure at rest
The discrepancy between measured and calculated energy expenditure during rest can be explained by the lower total muscle mass of the individual athletes and is attributed to the atrophy of the muscles of the paralysed lower extremities. It should be added here that the WHO calculations refer to people without any chronic disease or handicap [18]. Few reference data of energy expenditure of people with spinal cord diseases or injuries are available. Due to methodological differences, only slight comparisons can be made between the examinations by Huang et al. [19] and the results of this study, since the expenditure at rest was elevated by measurements with the subjects sitting as compared with the subjects lying in our study. In 48 paraplegic subjects, Mollinger et al. [20] found expenditure values at rest of 62.6 kcal/h in highly paralysed paraplegics and of 65.4 kcal/h in mildly paralysed paraplegics. In this study, the measured values also ranged clearly below the energy expenditure calculated by standard equations.
Energy expenditure during exercise
Extensive longitudinal studies focusing on the relation of the additional energy consumption due to physical activity on the one hand and the mortality and morbidity rate on the other hand [2, 3], could consistently demonstrate that additional physical activity provides an effect protective mechanism against the occurrence of atherogenic diseases. In recent studies Wei et al. [21] in particular revealed the importance of cardiovascular fitness, which essentially depends on the level of physical activity. According to this study, adiposity is no independent risk factor, if the person affected has an acceptable level of physical fitness. Preconditions for the evaluation of physical activity are systematic quantifications of the energy expenditure during various activities. Such examinations are available in the field of activities of non-handicapped people for almost any physical load and have been listed, for example, by Ainsworth et al. [12], with the values of energy expenditure given in METs
Weekly energy expenditure of the athletes in sport specific activities, further physical activities, and total sports activities. Recommended optimal additional energy expenditure from Paffenbarger et al. [17]

As expected, the values of energy expenditure of moderate and high exercise intensities differed significantly. The low intensity load was subjectively experienced by the participants as moderate (RPE ∼ 12). This was intended, as we wanted to simulate an aerobic training of basic endurance, which is usually recommended from the point of view of preventive medicine [22]. The achievement of this target could be confirmed by the evaluation of lactate concentrations with a mean value of 2.4 mmol/l. The higher heart rate values of the wheelchair racers as compared with the handbikers can basically be attributed to two causes. First, the sitting position of the wheelchair racers — due to a reduced angle in the hip joint — may lead to an increased accumulation of blood in the lower extremity as supposed by Hopman et al. [23]. The reduced venous return leads, in turn, to decreased ventricular diastolic filling and hence to lower preload of the heart. According to Frank and Starling's law, this results in a lower stroke volume being followed by a heart rate increase in order to maintain the required cardiac output. Secondly, the group of wheelchair racers were athletes from sprint disciplines, which may also explain the higher heart rates as compared with the endurance-trained handbikers. Between the mean values of energy expenditure of the two sports, no significant difference could be found. Comparative values of the energy expenditure of wheelchair athletes are only available from basketball. Burke et al. [24] demonstrated an energy expenditure of 6.5 METs, or 516 kcal/h. This value is also quoted by Ainsworth et al. [12]. These authors furthermore gave the energy expenditure of pushing a wheelchair to be 8 METs, without, however, mentioning any respective source. The values of energy expenditure for basketball reported by Burke et al. [24] are 1.1 METs or 126.4 kcal/h higher than the mean values of the handbikers at moderate intensities in our study. In comparison to the group of wheelchair racers the mean values of total energy expenditure in kcal/h for basketball were higher by 170.7 kcal/h. By comparison, the group of wheelchair racers showed higher values in METs by 0.28, mainly reflecting the low body weight of this group (59.2 kg). According to these findings relative values of energy expenditure in METs seem to be more valid. In addition the differing results mainly reflect the differences in intensities of exercise in both studies. Recommendations for maintaining cardiorespiratory and muscular fitness such as those by the American College of Sports Medicine [22] can without doubt be implemented in the examined wheelchair sports. This would require a training frequency of 3-5 units with a duration of 20-60 min each at a moderate intensity. According to the examinations by Paffenbarger et al. [17], a clearly higher additional weekly energy expenditure of 2000 to 2500 kcal or an additional daily energy expenditure of approx. 300 to 350 kcal leads to the greatest possible reduction of the risk of myocardial infarction. Transferred to the wheelchair athletes, they would have to exercise between 46 and 60 min per training session in order to achieve the preset values (Table 2). It needs to be taken into account that the obtained values refer to a moderate training (70%
Thus, the athletes achieved encouragingly high weekly energy expenditures. In this context, however, it should be pointed out that these energy expenditures cannot be considered representative of people dependent on a wheelchair for transportation and sports, since the majority of the examined athletes are highly ambitious competition athletes. Based on the data of energy expenditure gathered in various wheelchair sports it would be possible and desirable to quantify larger subject groups, using questionnaires on physical activity with regard to the energy expenditure, and to examine the relations between physical activity and morbidity as well as mortality for wheelchair-dependent people in prospective studies.
Conclusion
The energy expenditure values of the examined wheelchair athletes in handbiking and wheelchair racing were encouragingly high and did not show any significant difference at comparable intensities. Despite the reduced muscle mass of the examined athletes, the well-known sports medical recommendations concerning energy expenditures can be achieved by individuals through a weekly training of at least three units of less than 1 h at moderate intensity. Moreover, the subjects involved in this examination also reached the energy expenditure values of 2000-2500 kcal/week, defined by Paffenbarger et al. [17], in the sense of the optimal energy expenditure to reduce cardiovascular disease.
Nevertheless, a systematic verification of the transferability of these concepts in the prevention of cardiac diseases for persons with spinal cord injuries are urgently required and of great importance.