
Abstract
Background
Exercise training (ET) has been shown to improve functional work capacity in patients with stable chronic heart failure (CHF) having moderate symptoms (NYHA class II). This analysis was conducted, to evaluate the effects of ET on left ventricular function and haemodynamics in patients with advanced CHF (NYHA class III) fulfilling the inclusion criteria of the COPERNICUS trial.
Methods
Seventy-three patients with moderate and advanced CHF were prospectively randomised to a training (n = 36), or to a control group (n = 37). At baseline and after six months, patients underwent echocardiography and symptom-limited ergospirometry with measurement of central haemodynamics by thermodilution.
Results
Nine out of 37 patients in the control group (C) and 10 out of 36 patients in the training group (T) had symptoms of advanced CHF. Exercise training over a period of six months resulted in an improvement of functional status on average by one NYHA class in patients with advanced CHF. Moreover, oxygen uptake at the ventilatory threshold increased by 49% (from 7.7 ± 1.0 to 11.4 ± 0.4 mL/min/kg, P<0.01 versus baseline) and at peak exercise by 32% (from 16.3 ± 1.6 to 21.5 ± 1.2 mL/min/kg, P<0.01 versus baseline) in training patients. The small, but significant reduction in left ventricular end-diastolic diameter by 7% (from 70 ± 2 to 66 ± 2 mm; P<0.05 versus baseline) was accompanied by an augmentation in stroke volume at rest by 32% (from 45 ± 3 to 60 ± 6 mL, P<0.05 versus baseline) and at peak exercise by 27% (63 ± 9 to 81 ±9 mL, P<0.05 versus baseline) as a result of ET in patients with advanced CHF.
Conclusion
In patients with advanced CHF (NYHA class III), long-term exercise training is associated with an enhanced physical work capacity, an improvement in stroke volume and a reduction in cardiomegaly.
Keywords
Introduction
Exercise intolerance as a hallmark of patients with chronic heart failure (CHF) was regarded as a warning symptom precluding any strenuous physical activity. However, growing evidence suggests that this approach does not protect patients from cardiac decompensation—it rather accelerates physical deconditioning and may worsen symptoms of heart failure. Randomised clinical studies clearly reveal that carefully designed exercise training programs improve symptoms of breathlessness, fatigue and functional work capacity in patients with CHF [1–9]. These beneficial training effects have been primarily attributed to a reversal of skeletal muscle abnormalities involving an enhanced oxidative capacity of the working skeletal muscle [3, 4, 10–12] and a partial correction of endothelium-dependent vasodilatation of resistance as well as conduit vessels [13–15]. Moreover, exercise training was shown to improve the neurohormonal balance thereby restoring heart rate variability. Besides the improvement in functional work capacity, one single, recent report suggests, that exercise training may reduce morbidity and mortality in patients with CHF [16]. Physicians have been concerned whether to prescribe regular physical exercise in patients with CHF since the additional load placed on the left ventricle might further deteriorate left ventricular function. However, this doesn't seem to be the case. In a prospective randomised training study—the Leipzig Heart Failure Training Trial (LHFTT)—we were able to demonstrate that long-term exercise training in patients with CHF is associated with a small but significant improvement in stroke volume and reduction in cardiomegaly [17]. Despite the improvements seen with regular physical exercise in patients with CHF, clear guidelines with respect to the kind and duration of training that should be described are still missing. Moreover, it is not understood yet whether patients with advanced chronic heart failure also benefit from a training intervention since previous trials have (due to safety concerns) mainly focused on patients with mild-to-moderate symptoms.
Therefore, using data from our previously published, prospective randomised trial, we analysed whether patients with advanced heart failure (NYHA class III) may benefit from a long-term, ambulatory exercise training program with respect to: (1) maximal exercise capacity and oxygen uptake, (2) left ventricular diameter, and (3) cardiac performance as compared to an inactive control group with the same severity of heart failure. Furthermore, we were interested whether patients with advanced heart failure (NYHA class III) benefit from the training intervention as much as patients with mild-to-moderate symptoms (NYHA class II) regarding the above mentioned parameters.
Methods
Patient selection
The inclusion and exclusion criteria have been published previously [17]. Briefly, 73 patients aged ≤ 70 years or younger with chronic heart failure as a result of a dilative cardiomyopathy or ischaemic heart disease were studied. The presence of heart failure was documented by signs, symptoms and angiographic evidence of reduced left ventricular function (ejection fraction <40%). Patients had to be clinically stable for at least three months and were required to have a physical work capacity at baseline greater than 25 watts prior to enrolment into the study. Exclusion criteria were: significant valvular heart disease, uncontrolled hypertension, diabetes mellitus, hypercholesterolaemia (≥ 6mmol/L), peripheral vascular disease, pulmonary disease or musculoskeletal abnormalities precluding exercise training. The Ethics Committee at the University of Leipzig approved the study protocol and all patients provided written informed consent before entry into the study.
Study design
Patients were prospectively randomised to either a training group or an inactive control group. All patients underwent invasive cardiopulmonary exercise testing and echocardiography at baseline and after six months.
In order to ensure close supervision, all patients assigned to the training group remained in hospital for the initial three weeks of the training program. They were asked to exercise four to six times daily for 10 minutes on a bicycle ergometer at a workload adjusted to 70% of the symptom-limited maximal oxygen uptake. Before discharge from the hospital, maximal symptom-limited ergospirometry was performed to calculate a training target heart rate for home training, which was defined as the heart rate reached at 70% of the maximal oxygen uptake during symptom-limited exercise. Patients were provided with bicycle ergometers for daily home exercise training and were asked to exercise close to their target heart rate daily for 20 minutes for a period of six months. Moreover, they were expected to participate in at least one group training session of 60 minutes each week consisting of walking, callisthenics, and ball games.
Patients assigned to the control group received their individually tailored cardiac medication and were supervised by their private physicians.
Cardiopulmonary exercise testing
Exercise testing was performed on a calibrated, electronically braked bicycle in an upright position. Workload was increased every three minutes in steps of 25 W beginning at 25 W. Exercise was discontinued when patients were physically exhausted, developed severe dyspnea or dizziness. Haemodynamics were measured using a 7 Fr Swan-Ganz catheter (Swan-Ganz 93A-131-7F Edwards Laboratories, Santa Ana, California) connected to a cardiac output computer; (COM-2, Edwards Laboratories) that was introduced into the right pulmonary artery through the right antecubital vein. Gas exchange measurements were simultaneously obtained at rest and at the end of each workload during bicycle exercise with a commercially available system (Jaeger EOS-Sprint). The ventilatory threshold (VT) was defined as the oxygen uptake prior to the systematic increase in the ventilatory equivalent for oxygen (VE/VO2) without a concomitant increase in the ventilatory equivalent for carbon dioxide (VE/VCO2) [18]. Heart rate was continuously monitored using an ECG and blood pressure was measured using an automatic cuff.
Echocardiography
All patients underwent a complete resting echocardiographic study in multiple views at both the initial and the final evaluations. End-systolic (ESD; [mm]) and enddiastolic dimension (EDD; [mm]) of the left ventricle were determined in the parasternal long-axis. Left ventricular ejection fraction was obtained in the apical long-axis using the disk method. At least three consecutive cardiac cycles were analysed and averaged in each patient by an experienced blinded observer.
Statistical analysis
Mean value ± standard error of mean (SEM) was calculated for all variables.
Stroke volume was calculated by dividing cardiac output by heart rate. Systemic vascular resistance was calculated as mean arterial pressure divided by cardiac output and was expressed as dynes per second per centimetre−5.
For statistical evaluation non-parametric tests (Mann-Whitney U-test for inter-group comparison, Wilcoxon signed-rank test for intra-group comparison) were used to avoid potential errors from non-normal distribution of data and due to the small sample size. To determine whether patients with severe chronic heart failure (NYHA class III) also benefit from the training intervention this group was analysed separately. To assess whether patients with severe (NYHA class III) and moderate symptoms (NYHA class II) of chronic heart failure respond to exercise training in a different way, those groups were also compared. The New York Heart Association functional class distribution was compared by the chi-square test. A two-sided P value of less than 0.05 was considered statistically significant.
Results
Patient selection
A total number of 73 patients were enrolled into the Leipzig Heart Failure Training Trial. The baseline characteristics of those patients have been reported previously [17]. Ten out of 36 patients in the training group and nine out of 37 patients in the control group showed signs of severe advanced heart failure consistent with NYHA class III. Additionally, all of these patients had a reduced peak oxygen uptake (≤ 18mL/min/kg). The remaining patients in both groups showed moderate symptoms of CHF (NYHA class II, Figure 1).
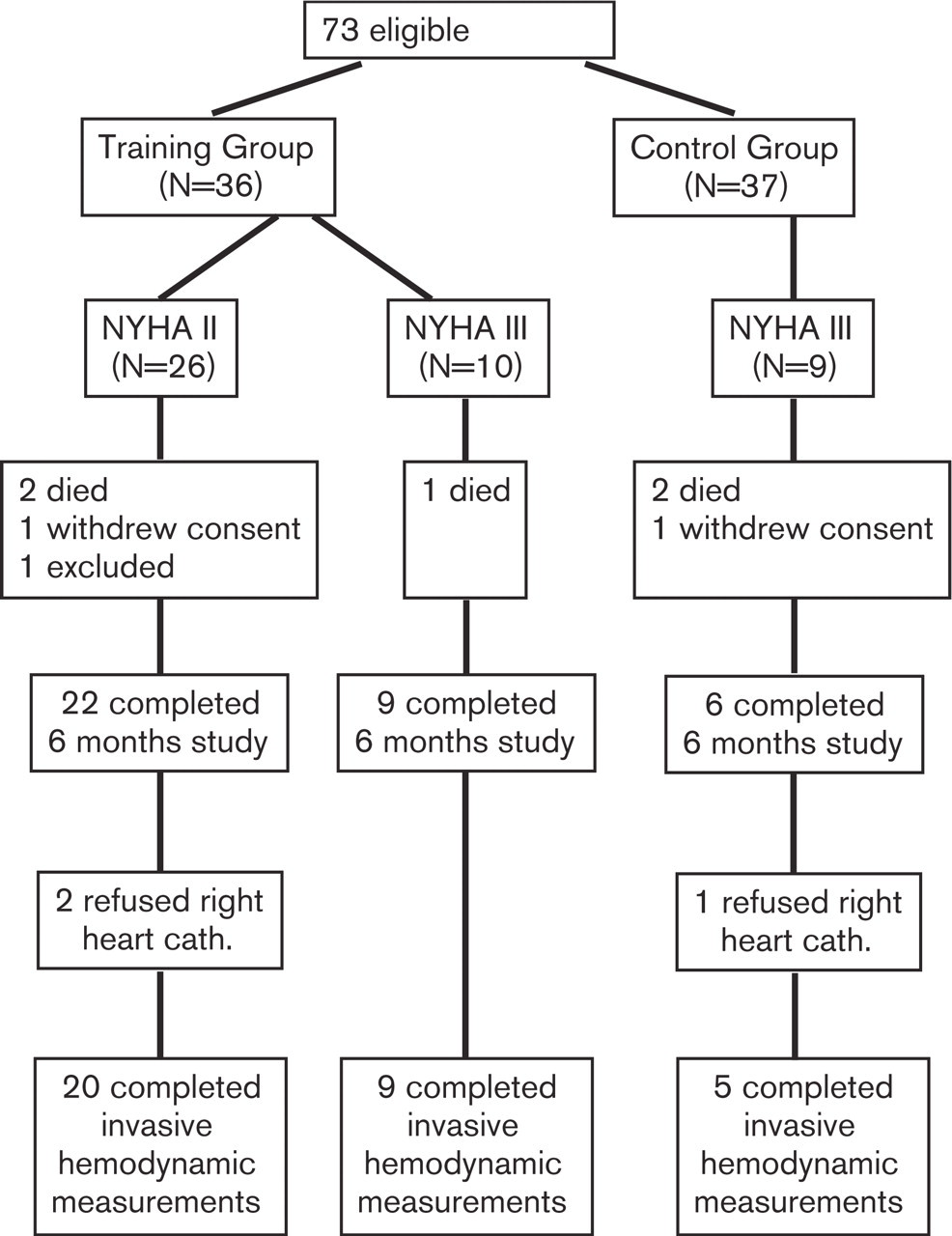
Patient randomization and follow-up. cath. indicates catheterization.
Baseline characteristics
Patients in the control and the training group with advanced CHF (NYHA class III) did not differ with respect to age, weight, LVEF, maximal oxygen uptake or medication (Table 1). However, patients with advanced CHF in the training group had a larger left ventricular end-diastolic diameter than those in the control group. Moreover, patients in the training group with moderate heart failure (NYHA class II) were characterized by a lower left ventricular end-diastolic diameter and a higher oxygen uptake at peak exercise (P = 0.03) compared to those with advanced CHF (NYHA class III, Table 1).
Dropouts and clinical events
In the exercise training group, three patients (NYHA class II: n = 2, NYHA class III: n = 1) died of sudden cardiac death unrelated to exercise during the study period of six months (Figure 1). These patients were comparable to those who successfully completed the exercise-training program with respect to age, LVEDD and VO2max. One patient was excluded from further analysis because of an atrioventricular node re-entrant tachycardia and one patient withdrew consent (NYHA class II). Data from 31 patients (NYHA class II: n = 22, NYHA class III: n = 9) were used for subsequent analysis.
Patient clinical characteristics
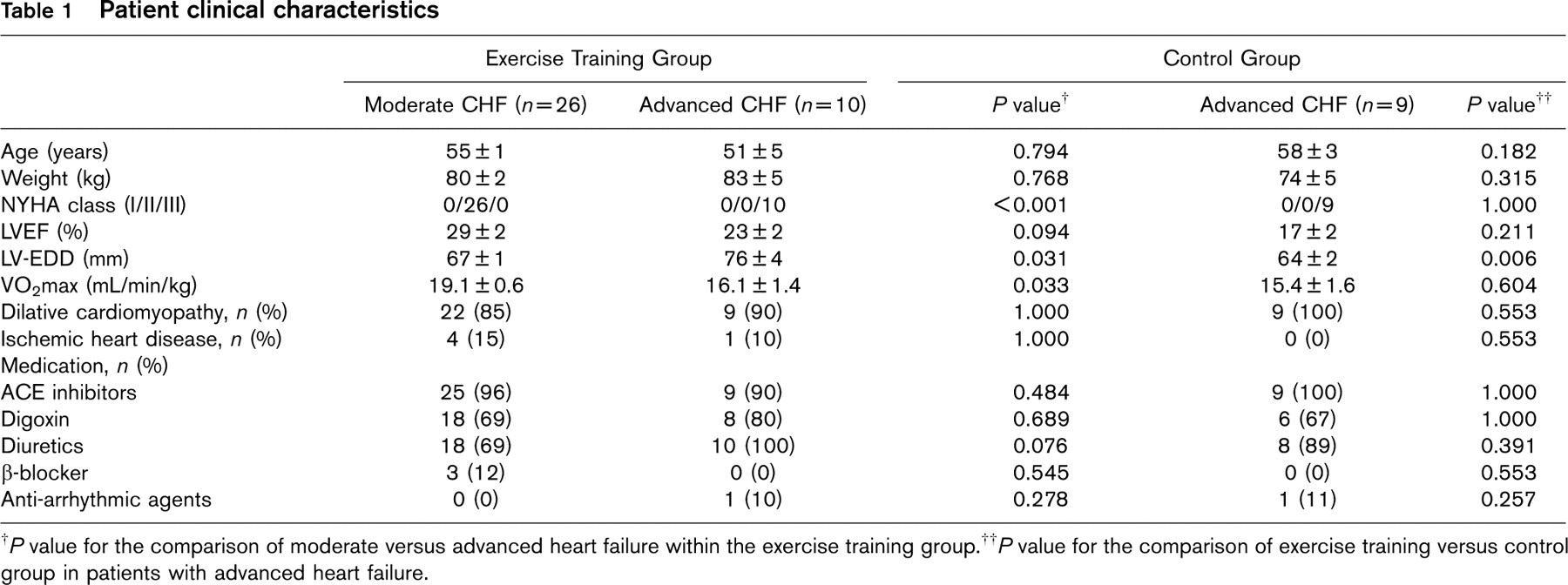
† P value for the comparison of moderate versus advanced heart failure within the exercise training group.
† P value for the comparison of exercise training versus control group in patients with advanced heart failure.
Exercise and gas exchange data
† P value for the comparison of moderate versus advanced heart failure within the exercise training group.
†† P value for the comparison of exercise training versus control group in patients with advanced heart failure.
∗∗ P<0.01 versus the beginning.
∗∗∗P<0.001 versus the beginning within the same group.
Two patients refused right heart catheterisation at the six months follow-up examination (NYHA class II), and therefore data from invasive measurements were completed for a total of 29 patients (NYHA class II: n = 20, NYHA class III: n = 9).
In the control group, two patients with advanced heart failure (NYHA class III) died of sudden cardiac death during the study (Figure 1). Another patient with NYHA class III withdrew consent for study participation after baseline measurements and one patient (NYHA class III) refused the right heart catheterisation during follow-up. These patients did not differ significantly with respect to the baseline parameters from patients in the control group that underwent the six-month follow-up evaluation.
Effects of exercise training on exercise capacity and maximal oxygen uptake
As a result of the exercise training, clinical symptoms of patients with moderate heart failure (NYHA class II) improved on average by half of one NYHA class (0.4 ± 0.1) and in patients with advanced heart failure (NYHA class III) by one NYHA class (1.0 ± 0.2), whereas the NYHA class in patients from the control group remained unchanged during the study period (Table 2).
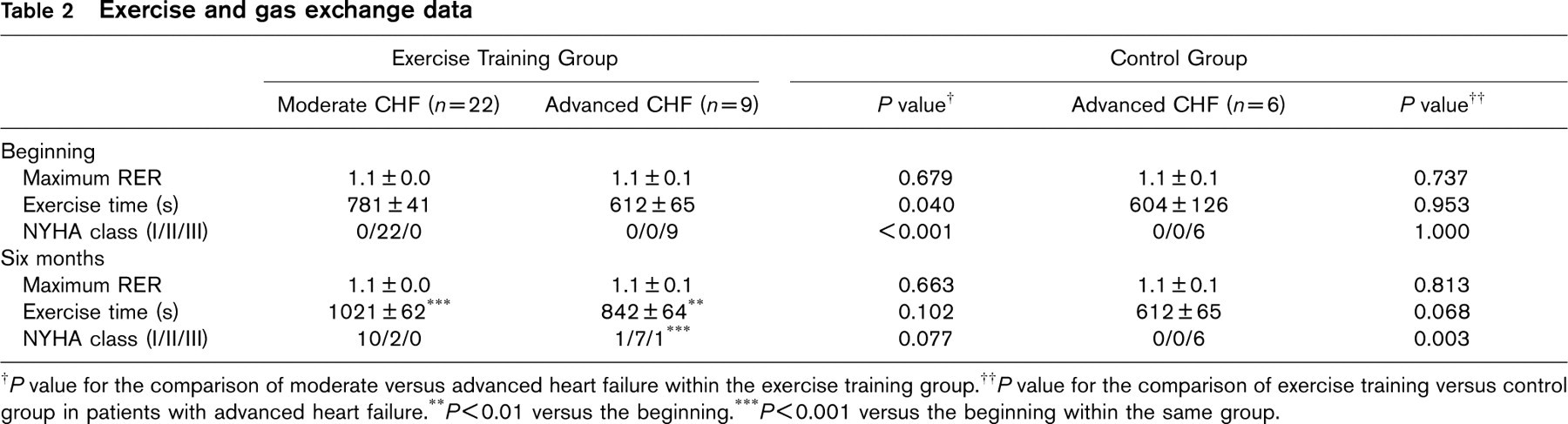
In patients with advanced CHF (NYHA class III) who underwent training, oxygen uptake at the ventilatory threshold increased by 3.7 ± 1.0 ml/kg/min and at peak exercise by 5.2 ± 1.6 mL/min/kg (Figure 2, Table 2) as a result of regular physical exercise. The augmentation in exercise capacity was accompanied by an increase in exercise time by 230 ± 71 s. Oxygen uptake at the ventilatory threshold and at peak exercise, as well as exercise time and exercise capacity, did not change in the control patients with advanced heart failure. However, despite that, patients with moderate symptoms of heart failure (NYHA class II) tended to have higher values regarding the above-mentioned parameters, the absolute improvement in oxygen uptake at the ventilatory threshold at peak exercise, and the increase in exercise time was comparable to those with NYHA class III (Figure 2, Table 2).
Effects of exercise training on central haemodynamics
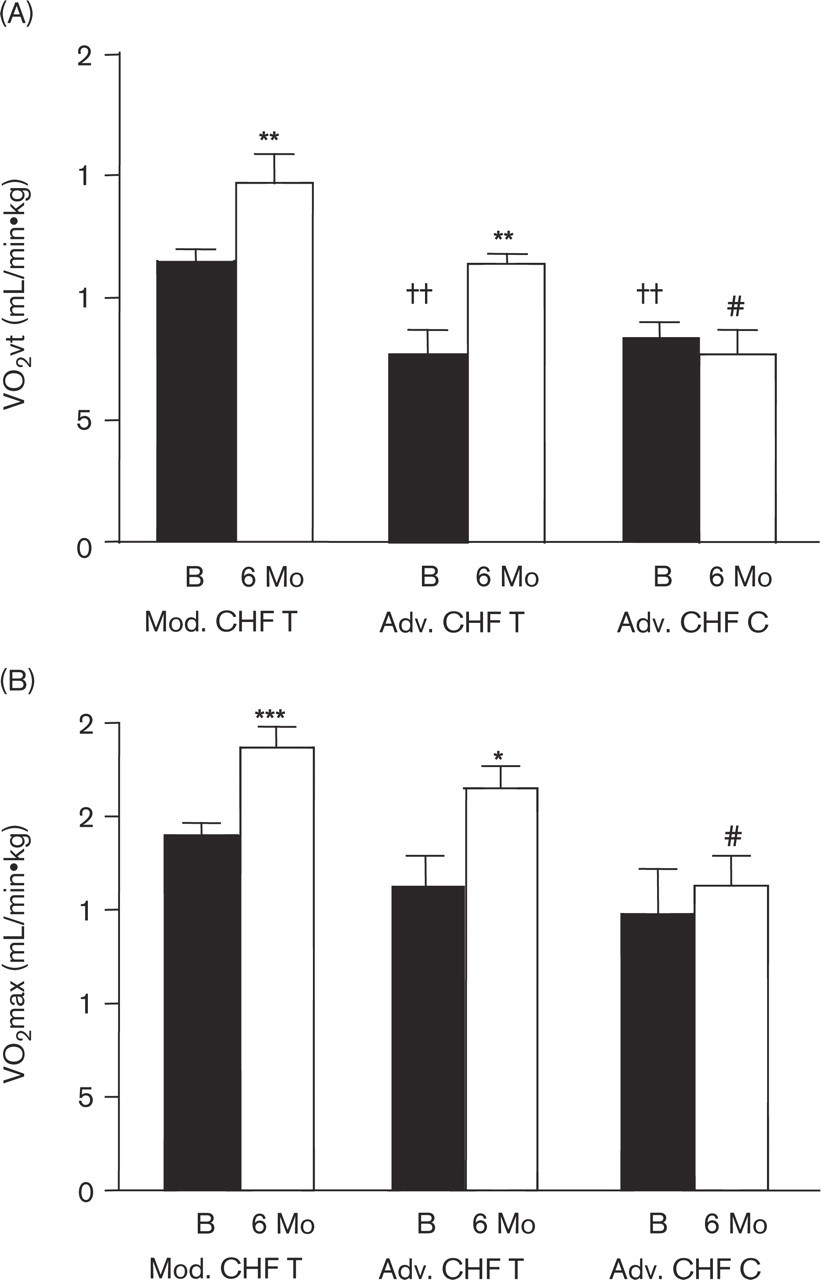
In patients with advanced CHF (NYHA class III) after six months of training, resting heart rate decreased by 6 ± 5beats/min and heart rate a peak exercise increased by 6 ± 5beats/min, but these changes were not statistically significant. In contrast, exercise training led to a significant increase in stroke volume at rest by 15 ± 6mL and at peak exercise by 17 ± 6mL in these patients (Figure 3). There was a trend toward an increase in cardiac output at rest from 4.3 ± 0.3 to 5.0 ± 0.4 L/min (P = 0.06) but the augmentation in stroke volume was offset by the decrease in resting heart rate (Table 3). As a result of improved stroke volume and increased heart rate, cardiac output at peak exercise was significantly enhanced by 3.1 ± 1.1 L/min (Figure 4A). In control patients with advanced heart failure, heart rate, stroke volume, and cardiac output at rest and during peak exercise did not change during the six months of the study period.
(A) Changes in oxygen uptake at the ventilatory threshold (VO2vt) in the training groups (T, advanced and moderate CHF) and the control group (C, advanced CHF). (B) Changes in oxygen uptake at the peak exercise (VO2max) in the training groups (T, advanced and moderate CHF) and the control group (C, advanced CHF). Mod CHF, moderate chronic heart failure; Adv CHF, advanced chronic heart failure; B, beginning; 6 Mo, 6 months. ∗ P<0.05 versus the beginning; ∗∗ P<0.01 versus the beginning; ∗∗∗ P<0.001 versus the beginning within the same group; †† P<0.01 versus Mod CHF at the beginning; # P<0.05 versus Mod CHF at 6 Mo.
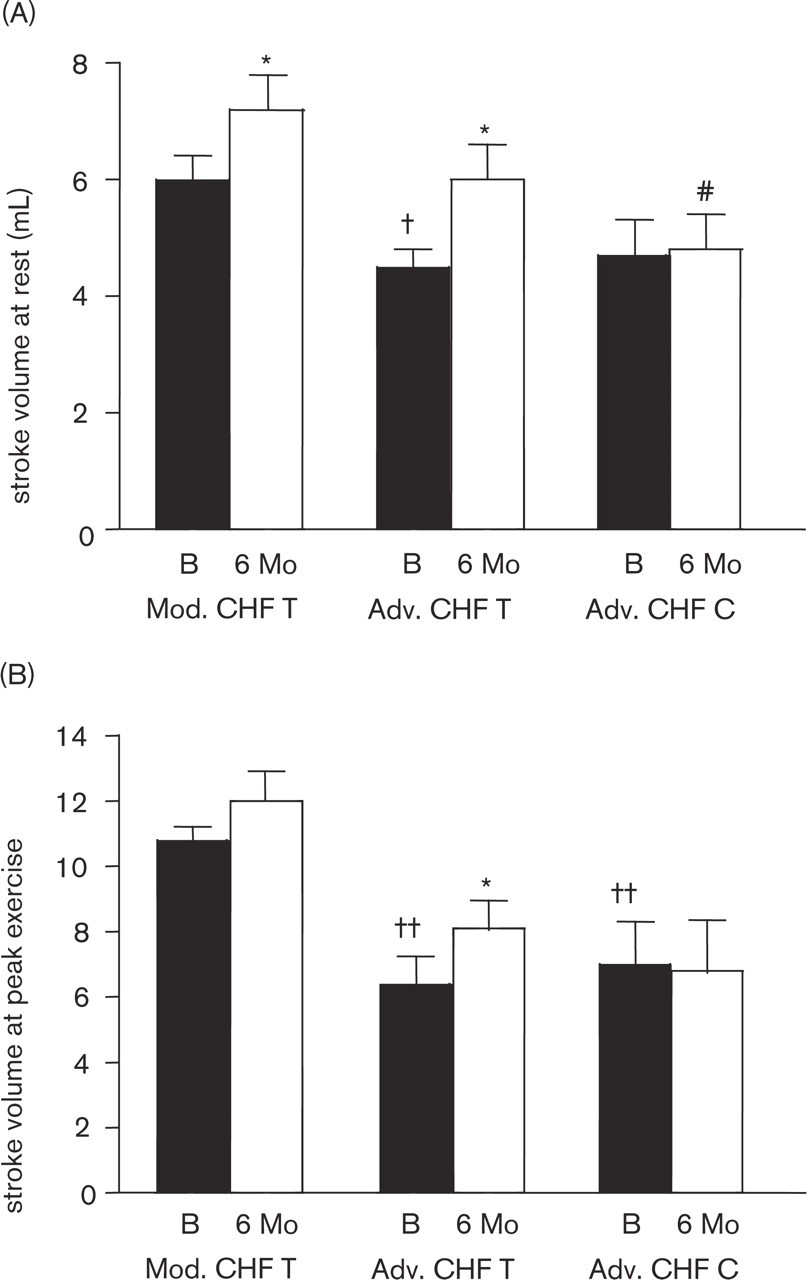
(A) Changes in stroke volume at rest in the training groups (T, advanced and moderate CHF) and the control group (C, advanced CHF). (B) Changes in stroke volume at peak exercise in the training groups (T, advanced and moderate CHF) and the control group (C, advanced CHF). Mod CHF, moderate chronic heart failure; Adv CHF, advanced chronic heart failure; B: beginning, 6 Mo: 6 months. ∗P<0.05 versus the beginning within the same group; † P<0.05 versus Mod CHF at the beginning; †† P<0.01 versus Mod CHF at the beginning; # P<0.05 versus Mod CHF at 6 Mo.
In patients with moderate symptoms (NYHA class II), resting heart rate declined non-significantly by – 11 ± 3 beats/min as a result of exercise training. There was only a significant improvement in stroke volume at rest by 12 ± 5 mL (Figure 3A), but not at peak exercise (Figure 3B). Despite the fact that increases in stroke volume and heart rate at peak exercise did not reach levels of statistical significance, cardiac output at peak exercise was significantly enhanced by 2.5 ± 0.8 L/min in these patients after six months of exercise training (Figure 4A). However, the beneficial trend towards an increase in cardiac output at rest after regular physical exercise was only visible in patients with more severe symptoms (NYHA III) at baseline. Mean pulmonary artery pressure at rest and in response to exercise remained unchanged at the end of the study compared to baseline in all of the groups (data not shown).
Heart rate, total peripheral resistance and pulmonary vascular resistance
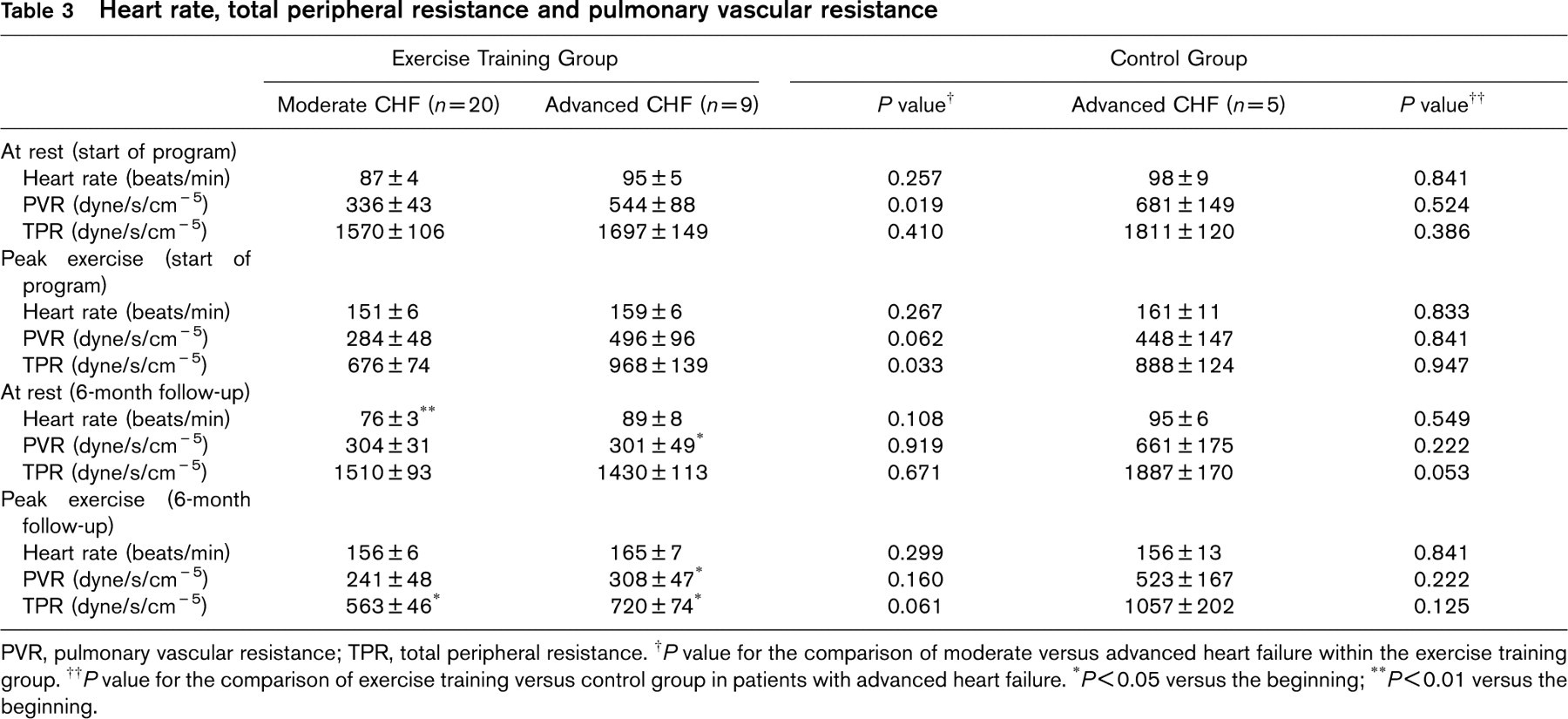
PVR, pulmonary vascular resistance; TPR, total peripheral resistance.
† P value for the comparison of moderate versus advanced heart failure within the exercise training group.
†† P value for the comparison of exercise training versus control group in patients with advanced heart failure.
∗P<0.05 versus the beginning;
∗∗P<0.01 versus the beginning.
Effects of exercise training on systemic and pulmonary vascular resistance
In patients with severe CHF (NYHA class III), long-term exercise training led to a non-significant decrease in systemic vascular resistance at rest by −266 ± 185 dynes·s·cm−5 and at peak exercise by −248 ±138 dynes·s·cm−5 (P = 0.053. for change versus control, Table 3). The exercise-training program also resulted in a decline in pulmonary vascular resistance at rest by −242 ± 98 dynes·s·cm−5 (P< 0.05 versus the beginning) and at peak exercise by −187 ± 104 dynes·s·cm−5 (P < 0.05 versus the beginning). However, neither systemic vascular resistance at rest and during peak exercise nor pulmonary vascular resistance at rest or during peak exercise changed significantly in patients in either the control group or in the training group with initially moderate symptoms (NYHA class II) during the six-month study period.
Effects of exercise training on echocardiographic LV-dimensions and ejection fraction
In patients with advanced heart failure (NYHA class III), left ventricular end-diastolic and end-systolic diameters decreased significantly from 70 ± 2 to 66 ± 2 mm and from 61 ± 2 to 54 ± 3 mm after six month of exercise training, respectively (P< 0.05. versus the beginning). Moreover, resting left ventricular ejection fraction improved in the training group in patients with advanced CHF from 27% to 33% at the six-month stage, (P = 0.075 versus the beginning). In contrast, left ventricular end-diastolic (66 ± 2 mm at the start, and 69 ± 3 mm after six months) and end-systolic diameter (59 ± 3 mm at the start and 62 ± 3 mm after six months) as well as ejection fraction remained essentially unchanged in the control group (Figure 4B).
However, patients with moderate symptoms of CHF (NYHA II) were characterized by a significant reduction in end-diastolic diameter from 68 ± 1 to 65 ± 2 mm and end-systolic diameter from 59 ± 2 to 54 ± 2 mm after six months of exercise training. This reduction in cardiac size was accompanied by a significant increase in left ventricular ejection fraction from 31 ± 2% at baseline to 36 ± 2% after six months of exercise training (Figure 4B).
Discussion
Three key messages emerge from this analysis evaluating the effects of a long-term exercise training program on exercise capacity, cardiac size and left ventricular function in patients with advanced heart failure (NYHA class III) in comparison with an inactive control group (NYHA class III) and an exercise-trained group of patients with moderate symptoms of chronic heart failure (NYHA class II):
Aerobic endurance training over a period of six months leads to an increase in exercise time, oxygen uptake at the ventilatory threshold and at peak exercise in patients with advanced chronic heart failure (NYHA class III) who fulfilled the inclusion criteria of the COPERNICUS trial. The improvement in exercise capacity was accompanied by an augmentation in left ventricular stroke volume at rest and during exercise and by a small but significant decrease in left ventricular end-diastolic diameter.
Long-term exercise training in patients with advanced chronic heart failure is associated with a considerable reduction of pulmonary vascular resistance at rest.
Patients with moderate (NYHA class II) and advanced (NYHA class III) heart failure showed a comparable increase in exercise time, oxygen uptake at peak exercise, augmentation in stroke volume at rest and peak exercise, and a comparable reduction in cardiac size as a result of the exercise training program. However, the trend towards an increase in cardiac output at rest and the decrease in pulmonary vascular resistance was only obvious in patients with advanced heart failure (NYHA class III). Both patients with moderate (NYHA class II) and advanced symptoms (NYHA class III) tended to have a lower peripheral resistance at rest and at peak exercise after the endurance-training program, but statistical significance was not achieved in either of the subgroups.
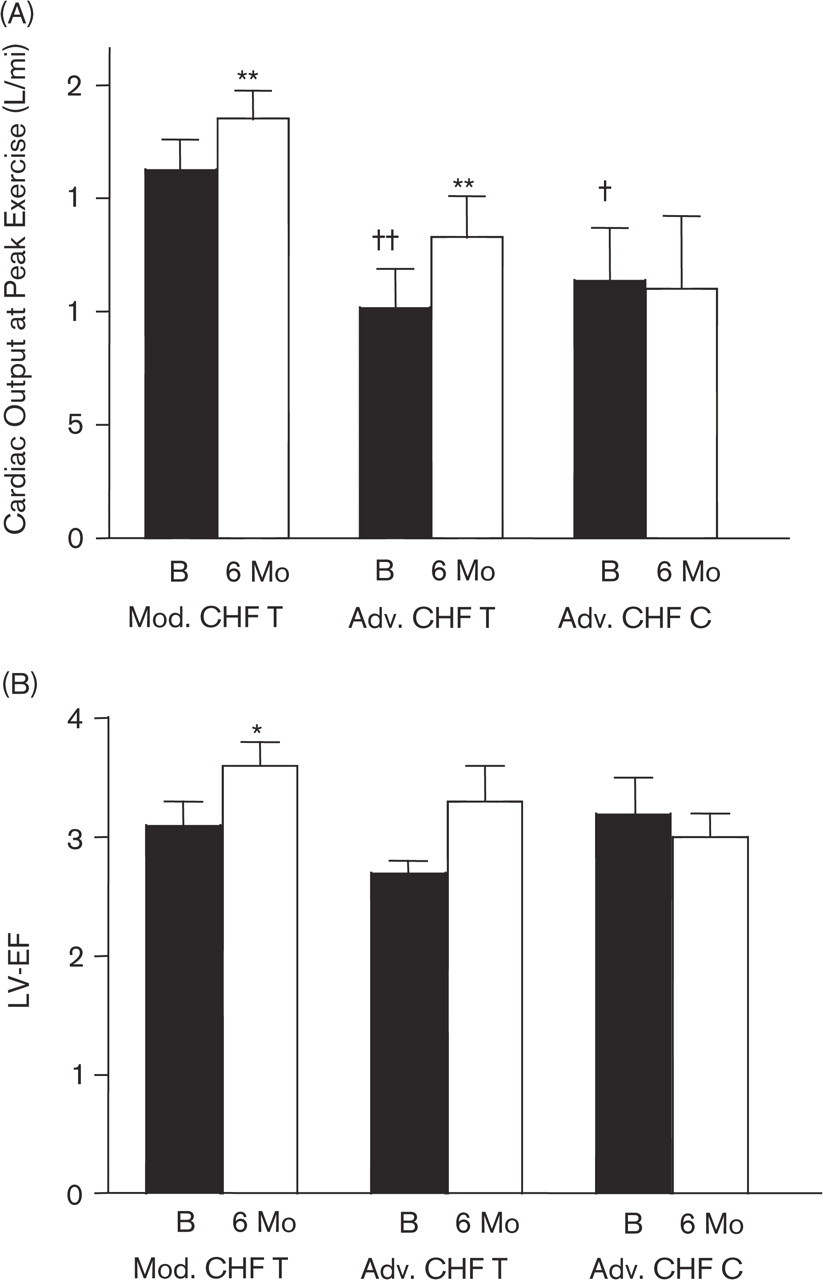
(A) Changes in cardiac output at peak exercise in the training groups (T, advanced and moderate CHF) and the control group (C, advanced CHF). (B) Changes in left ventricular ejection fraction (LV-EF) in the training groups (T, advanced and moderate CHF) and the control group (C, advanced CHF). Mod CHF: moderate chronic heart failure; Adv. CHF: advanced chronic heart failure; B, beginning; 6 Mo, 6 months. ∗ P <0.05 versus the beginning; ∗∗ P<0.01 versus the beginning within the same group; † P<0.05 versus Mod CHF at begin; †† P<0.01 versus Mod CHF at the beginning.
Exercise training is effective in patients with stable CHF
Previously, it has been shown that exercise training represents an effective, adjuvant therapy improving symptoms and clinical status in patients with CHF. The enhanced exercise capacity reflected by an increase in oxygen uptake at the ventilatory threshold and at peak exercise has been primarily attributed to adaptations in the peripheral circulation and the skeletal muscle [1, 19, 20]. Moreover, we have recently demonstrated that regular physical exercise in patients with chronic heart failure and mild-to-moderate symptoms positively effects central haemodynamics, resulting in a decrease in resting heart rate, an increase in stroke volume and a partial restoration of a normal left ventricular size [16]. Despite of the improvements seen with regular physical exercise, a considerable degree of uncertainty remains as to whether all patients, especially those in the advanced stages of heart failure (NYHA class III), benefit from the training intervention. In the present analysis we were able to show that the exercise-induced improvement in clinical symptoms is not limited to patients with moderate heart failure. Also patients in NYHA class III responded to the training intervention with an increase in oxygen uptake at the ventilatory threshold as well as at peak exercise and an augmentation in exercise time despite their lower baseline values (which reflected their more advanced stage of the disease).
Effects of exercise training on cardiac function
One of the major goals of any therapy in CHF is a reduction in left ventricular wall stress to prevent or decelerate a further cardiac dilatation. In the LHFTT [17], we unexpectedly found that six months of aerobic exercise training increased stroke volume at rest and at peak exercise in patients with mild-to-moderate symptoms of CHF. Further analysis of this data revealed that patients in the more advanced stages of heart failure (NYHA class III) especially benefited from the training intervention as reflected by a remarkable increase in stroke volume at rest. This resulted, despite the reduction in resting heart rate, in an augmentation in cardiac output at rest by approximately 20%. Moreover, stroke volume at peak exercise increased significantly in those patients indicating an enhanced cardiac performance.
Besides the improvement in stroke volume, the hearts of patients with severe heart failure (III) were characterized by a significant reduction in end-diastolic as well as end-systolic diameter following the six-months exercise training. A comparable restoration in cardiac shape with a decrease in the above-mentioned parameters in response to regular physical exercise was also seen in patients with milder symptoms (NYHA class II). One possible explanation for the enhanced cardiac performance maybe the decrease in resting heart rate with a lengthened diastolic filling period accompanied by an augmentation of stroke volume. However, the increase in stroke volume in patients with advanced heart failure was even seen with a non-significant reduction in heart rate. Therefore, additional mechanisms seemed to be involved in the augmentation in stroke volume.
Possible mechanisms explaining the improvement of cardiac performance
We have previously attributed the reduction in cardiac size and the increase in stroke volume at rest and during peak exercise to an after-load reduction as a sign of a decrease in systemic vascular resistance. In the present analysis we also observed a reduction in systemic vascular resistance at rest and during peak exercise in patients with advanced CHF (NYHA class III) as a result of the training intervention. Due to the small sample size and the inter-individual variations, the trend—which is also seen in patients with milder symptoms (NYHA class II)—did not reach statistical significance. The reduction in after-load may be attributed to several mechanisms—it has been shown previously that patients with CHF are characterized by an impaired endothelium-dependent vasodilation in response to stimulation with agonists or flow [23, 24]. The blunted vasodilatory capacity of small resistance vessels at rest and especially during exercise might contribute to higher systemic vascular resistance in both circumstances. Recently, we were able to demonstrate that systemic physical exercise not only corrects endothelium-dependent vasodilation of the trained lower limb (most likely by an enhanced endothelial nitric oxide formation), but also improves endothelial function of the untrained upper limb [15, 25]. However, in the present analysis complete data with respect to peripheral endothelial function were only available in a minority of the patients precluding further statistical analysis.
Furthermore, peripheral vascular resistance may also be lowered by an attenuation of sympathetic activity and an increased vagal tone seen in patients with heart failure after regular physical exercise [21]. Previously we have shown that exercise training in patients with CHF significantly decreases plasma epinephrine concentrations. However, the changes in plasma catecholamines were not related to changes in systemic vascular resistance [17].
One surprising result of this subgroup analysis is that patients with severe symptoms especially benefited from the training intervention with a remarkable decrease in pulmonary vascular resistance at rest. It is tempting to speculate that the improvement in LV systolic function may lead to a decrease in preload thereby reducing pulmonary artery pressure and pulmonary vascular resistance. Alternatively, it is conceivable that the improvement of endothelial function may affect pulmonary resistance vessels or that both mechanisms contribute to the decrease in pulmonary vascular resistance.
Clinical implications
This analysis suggests that exercise training in patients with advanced heart failure (NYHA class III) improves clinical symptoms, exercise time, oxygen uptake at the ventilatory threshold and at peak exercise to a similar extent when compared with patients with only moderate CHF. Moreover, the six months of exercise training were associated with an increase in stroke volume at rest and at peak exercise and by a small but significant reduction in cardiac size.
However, every subgroup analysis should be interpreted in light of several limitations. The study was conducted in one centre, was limited to men with chronic heart failure and only 19 patients with advanced CHF were randomised to both groups. However, despite these limitations the data revealed that exercise training seems to be safe and efficient in patients with advanced chronic heart failure (NYHA class III) and prompted us to conduct a randomised, prospective trial assessing not only the effects but also different training protocols in patients with severe CHF (NYHA class III to IIIb).
Footnotes
Acknowledgements
This study was supported by a grant from the Deutsche Herzstiftung, Germany (F/21/02).