
Abstract
Background
Measurement of intima-media thickness (IMT) is a well established surrogate marker for cardiovascular endpoints. We studied the long-term effects of statins on femoral IMT and plaque scoring in the Atorvastatin versus Simvastatin on Atherosclerosis Progression (ASAP) study.
Methods and Results
Three hundred and twenty-five patients with familial hypercholesterolaemia were randomized to either atorvastatin 80 mg/day or simvastatin 40 mg/day. IMT was measured at baseline and at 2 years. At baseline, femoral IMT was 1.69 mm in the atorvastatin group and 1.61 mm in the simvastatin group; at 2 years, IMT increased by 0.06 mm (P=0.24) and 0.15 mm (P=0.012), respectively. No significant differences were obvious between these two treatment arms (P=0.26). Femoral plaques were present in 64.7% in the atorvastatin group and 56.1% in the simvastatin group at baseline; after 2 years, these proportions rose to 66.0% (P=0.47) and 67.3% (P=0.02), respectively (P=0.87 between treatment arms). Carotid plaques were present in 6.3% versus 4.9%; after 2 years, these percentages were 5.0% (P=0.48) versus 5.5% (P =0.71), respectively (P=0.90 between treatment arms).
Conclusion
Our study indicates increased efficacy of atorvastatin 80 mg in retarding progression of atherosclerosis in the femoral artery compared with simvastatin 40mg. Interestingly, in the carotid arteries these statins influenced IMT to a greater extent, whereas in the femoral artery the effects were more pronounced on plaque frequency. These findings underscore the generalized effects of lipid lowering on atherosclerosis.
Introduction
The measurement of intima-media thickness (IMT) of superficial arteries has been validated as a surrogate marker for atherosclerotic changes. Prospective studies have shown that increased IMT can predict myocardial infarction (MI) and cerebral vascular events [1–3]. An increase of IMT of 0.03 mm/year is considered clinically significant, since this is associated with a relative risk of 2.2 for nonfatal MI or coronary death [4].
Recently, we have reported on the ASAP (effects of Atorvastatin versus Simvastatin on Atherosclerosis Progression) study cohort [5]. In this trial we studied patients with heterozygous familial hypercholesterolaemia (FH). FH is an autosomal dominant disease characterized by a two- to threefold increase in low density lipoprotein cholesterol (LDL-C) caused by mutations in the LDL-receptor gene. FH patients have a sharply increased risk for early cardiovascular disease (CVD) due to rapidly progressive and extensive atherosclerosis.
The ASAP study was a 2-year, double-blind, randomized clinical trial, where patients were randomized to either atorvastatin 80 mg/day or simvastatin 40 mg/day. Ultrasound scans of carotid and femoral arterial walls were performed. Carotid IMT defined the primary ultrasound endpoint and these data have been previously reported [5]. Subsequently, we reassessed the dataset of the ASAP study to include the femoral artery IMT, a secondary outcome parameter in this trial, as well as the plaque scoring of both carotid and femoral arteries [6]. Our primary objective was to determine whether changes in femoral wall IMT would parallel those in the carotid arteries. Secondly, we wanted to assess whether plaque frequency, as a marker for advanced atherosclerosis, would also respond favourably to intensive or moderate lipid-lowering therapy. In particular, it has been suggested that plaque measurements are better correlated with atherosclerotic events than IMT itself [7]. Here, we present the results of our analyses.
Methods
Protocol
Design and main results of the ASAP study have been reported previously [5]. In summary; ASAP was a 2-year, two centre, randomized, double-blind trial in FH patients to assess whether treatment with atorvastatin 80 mg/day or simvastatin 40 mg/day could retard atherosclerosis progression in FH patients. Men and women aged between 30 and 70 years with FH were screened for eligibility. Patients were either previously untreated or treated, but with LDL-C remaining above 4.5 mmol/l. After an 8-week placebo run in, in which all lipid-lowering medication was discontinued, baseline measurements of lipoprotein parameters and IMT were performed. These measurements were repeated after 2 years. The Institutional Review Boards of both centres approved the protocol and written informed consent of all participants was obtained [6].
Laboratory
Lipoprotein parameters included total cholesterol (TC), (calculated) LDL-C, high density lipoprotein cholesterol (HDL-C) and triglycerides (TG) and were analysed as described previously [6].
Intima media thickness
IMT measurement procedures have been reported before [6]. Ultrasound examinations were performed using a Biosound Phase-2 real time scanner (Biosound Esaote, USA). A high resolution scanner with a 10MHz transducer was used. The mean carotid IMT represents the average of anterior and posterior walls in the common carotid artery (CCA), the carotid bifurcation (BUL) and the posterior wall of the internal carotid artery (ICA), bilaterally. The mean femoral IMT represents the far wall of the common femoral artery (CFA).
In this study a plaque was predefined as an IMT ≥ 1.3 mm and/or wall interface displacement [6].
Images were analysed off-line with semi-automatic edge detection software (Eurequa; TSA company, Meudon, France) [8]. Ultrasound scans were performed by well-trained ultrasonographers in the two centres. The images were stored on disk and analysed by independent readers blinded to treatment information of the patients. During the study reproducibility was checked at regular time points. The intra-observer and inter-observer coefficients of variation were < 5%.
Statistical analysis
The number of participants required to detect a minimal relevant effect over 2 years (change in mean IMT) of 0.05 mm. with a power of 80%, α = 0.05 and a within-subject over time standard deviation estimated as 0.15, equals 141 per treatment group. Allowing for a 10% dropout rate, the total number of patients would amount to 313. In effect a total of 325 patients could be included. The primary efficacy parameter was change in IMT in millimetres after 24 months. Changes from baseline within groups were analysed with a paired t-test or a Wilcoxon test for variables with a skewed distribution. Differences between groups were compared using the independent t-test. McNemar tests were applied for comparing the proportion before and after treatment within groups. Changes of dichotomous data between groups were tested using conditional logistic regression analysis. Statistical analyses were performed using SAS (version 8.02, SAS Institute Inc. Cary, NC, USA).
Results
Lipids
The lipid results have already been published [5]. In short, at baseline there were no significant differences in lipid levels between both treatment groups. LDL-C was reduced by 50.5% in the atorvastatin 80 mg group and 41.2% in the simvastatin 40 mg group. HDL increased by 13% in both treatment groups. Atorvastatin reduced TG levels by 29.2% and simvastatin reduced these levels by 17.7%. Atorvastatin was significantly better in lowering LDL-C and TG levels as compared with simvastatin 40 mg (P = 0.0001 and P = 0.0023, respectively).
Femoral artery IMT
Baseline characteristics of patients in the ASAP study are summarized in Table 1.
The IMT of the common femoral arterial walls could be obtained in 156 (98%) of the 160 patients in the atorvastatin 80 mg treated patients and 158 (96%) of the 165 patients in the simvastatin 40 mg treated patients. Baseline IMT of the CFA was 1.69 mm in the atorvastatin arm versus 1.61 mm in the simvastatin arm. Femoral IMT was significantly correlated with carotid IMT (r = 0.29; P < 0.001). After 2 years of statin treatment these values were 1.74 and 1.75 mm, respectively (Table 2). The IMT increase of 0.05 mm in the atorvastatin group did not reach significance (P = 0.24). In contrast, the 0.14 mm increase of IMT in the simvastatin group was significant (P = 0.012). No significant difference (P = 0.26) was obvious between these two treatment arms.
Carotid artery IMT
The findings with regard to mean carotid IMT have already been published [5]. In short, atorvastatin 80 mg led to a decrease of 0.031mm (P < 0.002), while simvastatin 40 mg was associated with an increase of 0.036 mm (P < 0.005) of mean carotid IMT after 2 years of treatment (difference between treatments P < 0.001).
Baseline characteristics of the patients in the ASAP study
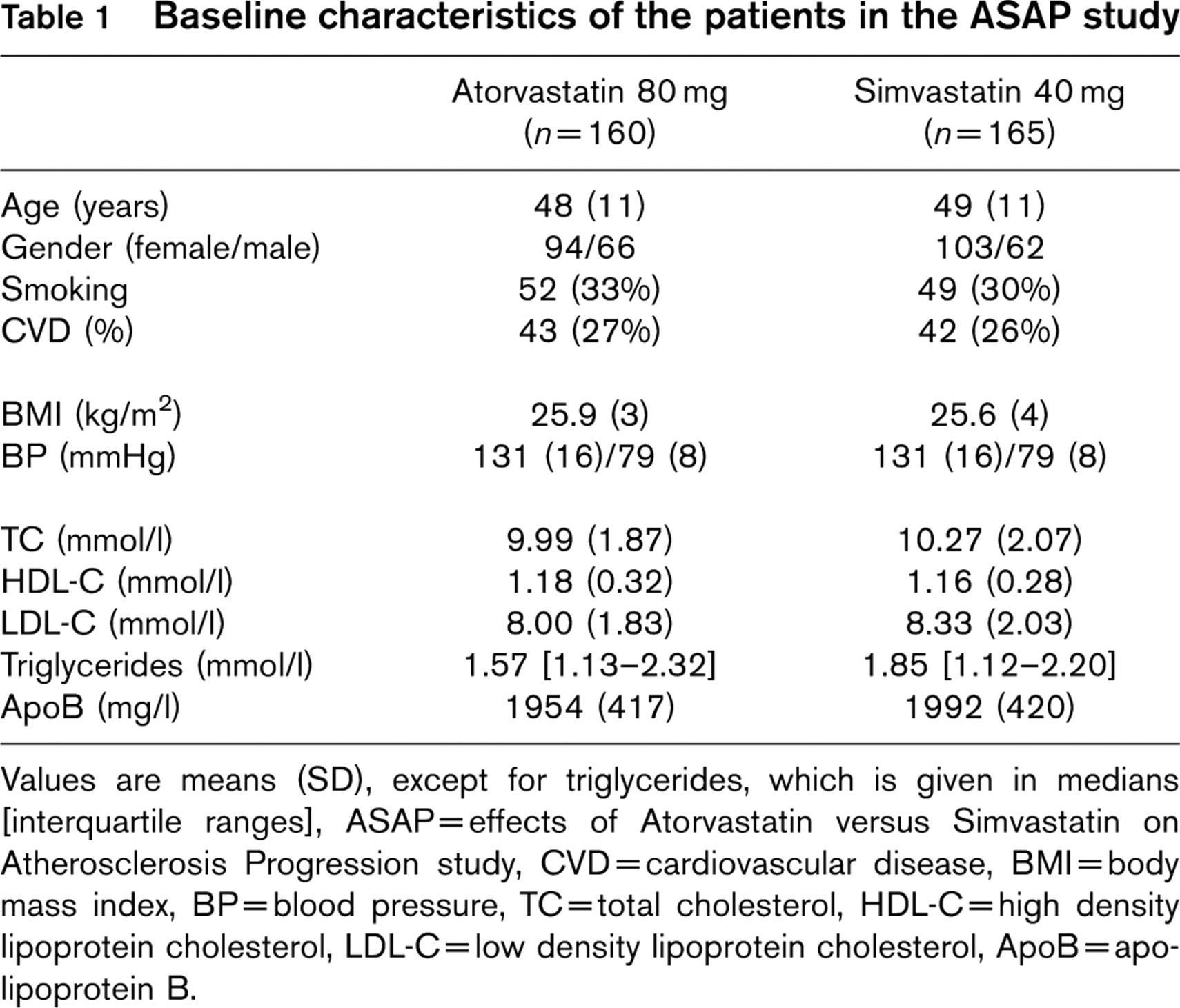
Values are means (SD), except for triglycerides, which is given in medians [interquartile ranges], ASAP = effects of Atorvastatin versus Simvastatin on Atherosclerosis Progression study, CVD = cardiovascular disease, BMI = body mass index, BP = blood pressure, TC = total cholesterol, HDL-C = high density lipoprotein cholesterol, LDL-C = low density lipoprotein cholesterol, ApoB =apolipoprotein B.
Mean IMT at baseline and at 2 years in the simvastatin and atorvastatin treated patients
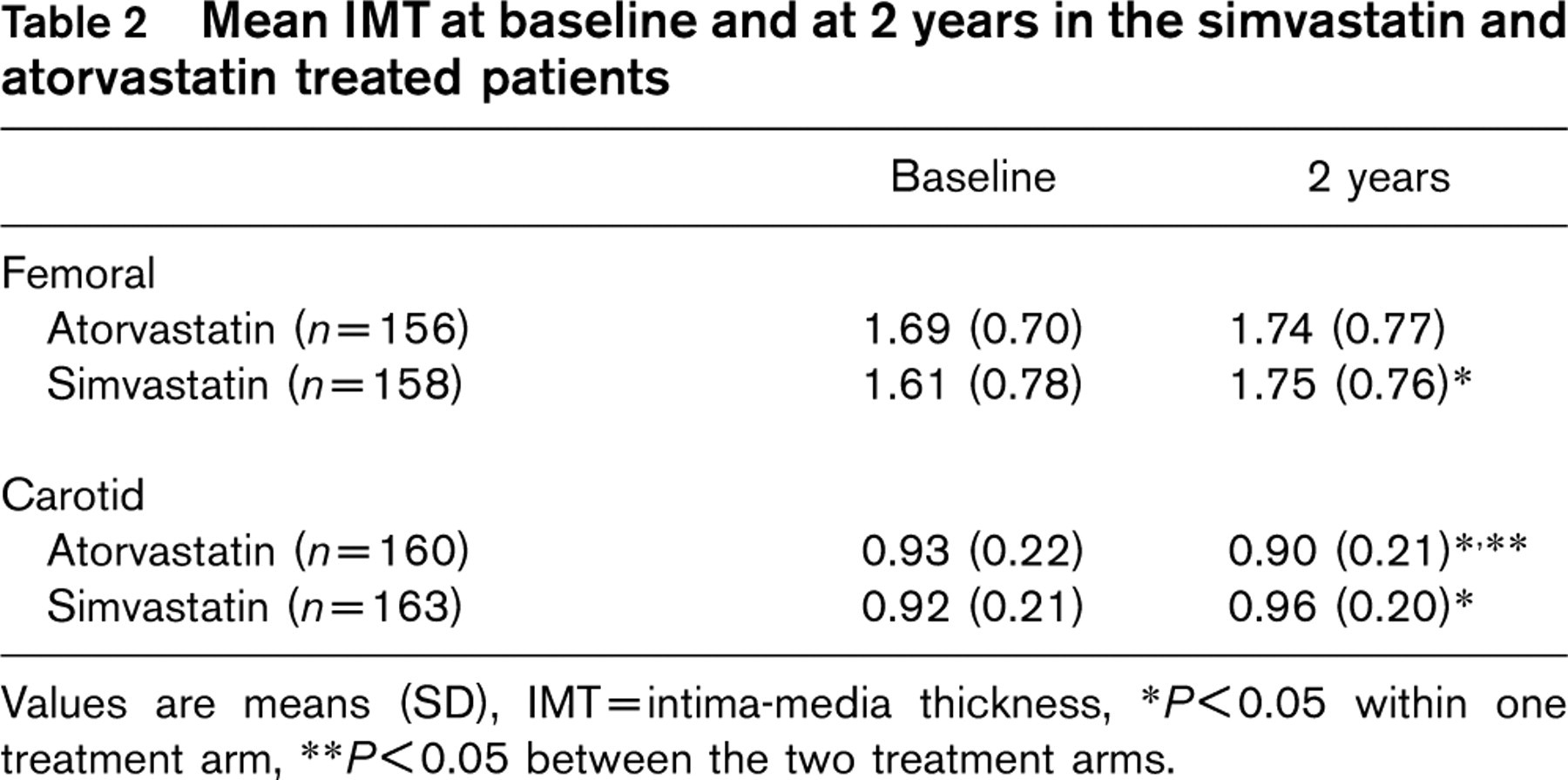
Values are means (SD), IMT = intima-media thickness,
P<0.05 within one treatment arm,
P<0.05 between the two treatment arms.
Plaque scoring
Plaques were present in the femoral arteries in 65.0% of the patients in the atorvastatin 80 mg group and in 57.0% in the simvastatin 40 mg group. The plaque frequency at baseline was not significantly different between the two treatment arms (P= 0.19). After 2 years of statin treatment these percentages increased to 67.5% and 68.5%, respectively (Table 3). The rise in the atorvastatin arm was not significant (P = 0.48), but again in the simvastatin arm the increment did reach statistical significance (P = 0.004). The difference between both treatment arms was not significant (P = 0.87).
In the carotid arteries plaques were present in 6.3% of the patients in the atorvastatin 80 mg group and 4.9% in the simvastatin 40 mg group. After 2 years of treatment these percentages were 5.0% and 5.5%, respectively (Table 3). The change within the treatment groups was neither significant in the atorvastatin arm (P = 0.48), nor in the simvastatin arm (P = 0.71). In addition, the difference between the two treatment arms after 2 years was also not significant (P = 0.90). No significant correlation was observed between plaques present in the femoral artery and the carotid artery, which is most likely due to the small number of plaques present in the carotid arteries.
Discussion
These analyses of the femoral and carotid arteries of FH patients show that the increase of femoral IMT seen over the course of 2 years with simvastatin 40 mg treatment was attenuated in the atorvastatin 80 mg treated patients. In support of these findings, the percentage of plaques in the femoral artery increased significantly in the simvastatin arm, but not in the atorvastatin arm. Lastly, and perhaps most importantly, the percentage of plaques in the carotid artery increased in the simvastatin arm, but decreased in the atorvastatin arm. Although this change did not reach statistical significance the latter results point to a trend comparable with the IMT data. These differences in terms of IMT and plaque development in the two treatment regimens are probably due to the stronger LDL-C and TG reductions in the atorvastatin 80 mg arm [5].
Plaques score (%) at baseline and at 2 years in the atorvastatin and simvastatin treated patients
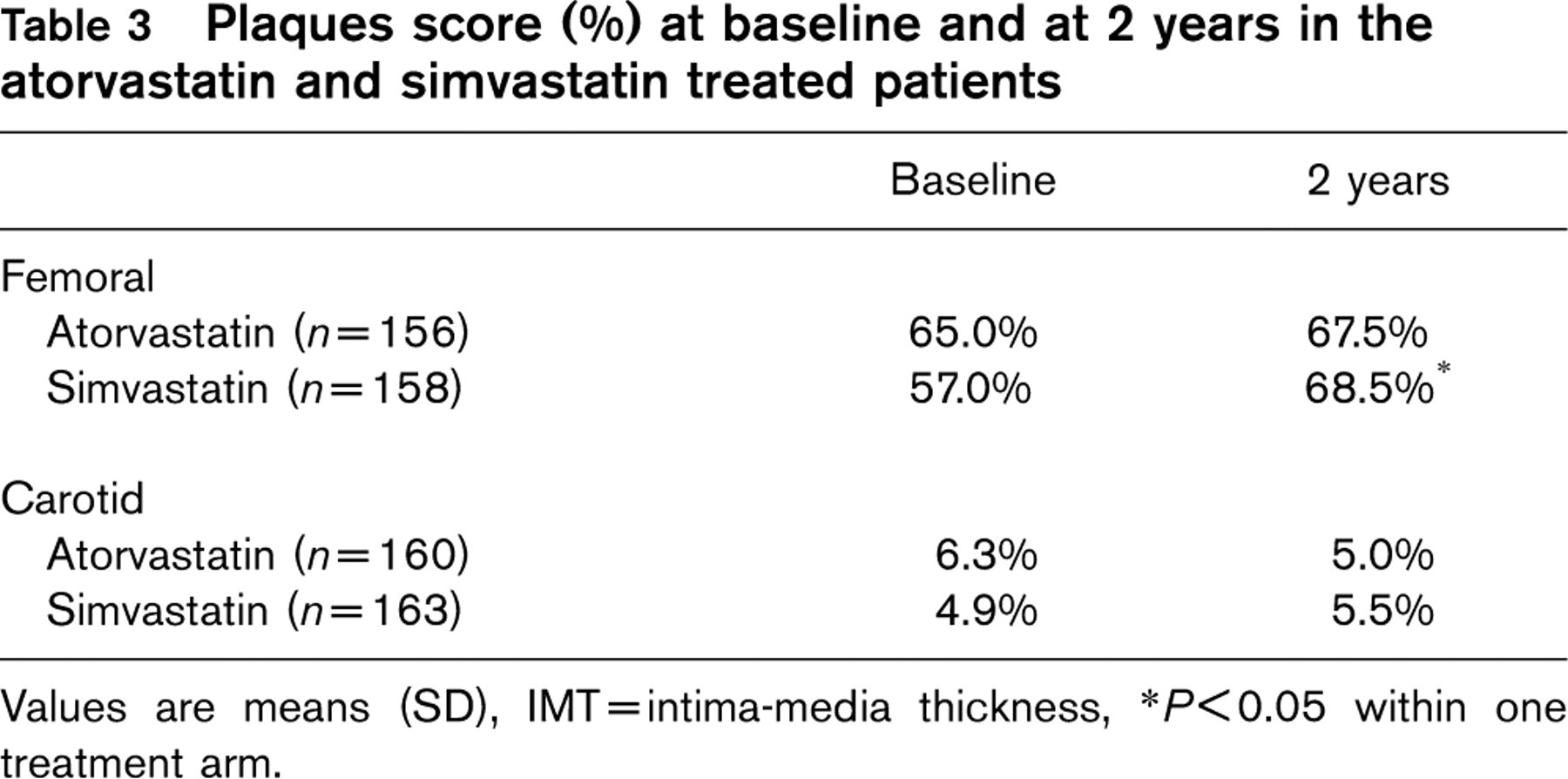
Values are means (SD), IMT = intima-media thickness,
P<0.05 within one treatment arm.
Nevertheless, these results raise several questions. First, is there a fundamental difference between the atherosclerotic process in the carotid compared with the femoral artery? In support of this hypothesis it is apparent that the atorvastatin treated patients did not demonstrate a clear decrease of femoral IMT, such as previously reported for the carotid IMT [5]. The direction of these changes, however, was similar in the femoral and carotid artery for both atorvastatin 80 mg and simvastatin 40 mg treated patients. This may indicate that even stronger reductions of LDL-C levels are necessary to induce regression of the arterial wall thickening in the femoral versus carotid artery, or, conversely, that LDL modification does not have a similar impact on atherosclerotic changes in the vasculature of lower extremities. The latter is highly unlikely, since the Heart Protection Study (HPS) shows similar percentage event reductions in event rates for coronary, cerebrovascular and peripheral arterial disease [9]. Another possible explanation is that organized and fibrotic plaques, which are present at a higher frequency in the femoral artery, show smaller therapeutic response. Furthermore, the size of the effect of statin intervention depends to a significant extent on variability of IMT per se and since variability is greater in the femoral artery, this could mask the effect of statin intervention on change in femoral IMT.
Secondly, are our findings compatible with the results of other lipid-lowering trials using IMT as a surrogate marker? Recently, an expert panel concluded that the far wall of the CCA is the preferred segment to use in lipid-lowering trials [10]. Indeed, the Atherosclerosis Risk in Communities (ARIC) study showed that the CCA correlated well with all major cardiovascular risk factors and supported the results of the Cholesterol Lowering Atherosclerosis Study (CLAS) [2, 4]. Moreover, the Pravastatin, Lipids and Atherosclerosis in the Carotid Arteries (PLAC II) study demonstrated that the far wall of the CCA was significantly correlated with both progression and regression of atherosclerotic disease [11]. Furthermore, in CLAS the therapy effect observed in the femoral arteries was less marked than the strong and consistent benefit reported for both native coronary arteries and aortocoronary bypass grafts [12].
In contrast, in the Regression Growth Evaluation Statin Study (REGRESS) IMT measurements were performed in a subgroup of 255 patients with CVD. In this study pravastatin retarded the increase in IMT compared with placebo, seen over a 2-year period. This effect was predominantly observed in the far wall of the common femoral artery [13]. Recently, a study in which the association between carotid and femoral IMT and coronary artery disease was investigated, indicated that the femoral IMT was also a strong and independent predictor of the extent and severity of coronary atherosclerosis as assessed by coronary angiography [14]. However, another study did not find a significant relationship between femoral artery IMT and coronary atherosclerosis [15].
The question now before us is whether the femoral artery should be used in IMT scanning protocols. Data on femoral IMT alone are scarce and conflicting, in contrast to the reproducible and vast amount of data on carotid IMT. Therefore, we feel that measurement of the carotid IMT provides sufficient information to assess the efficacy of different drug regimens in lipid-lowering intervention trials. Recently, Iglesias del Sol et al. [16] discussed that all the different IMT measurement sites in the carotid artery have the same ability to predict future MI.
In conclusion, our study indicates that atorvastatin 80 mg inhibits atherosclerosis progression to a greater extent than simvastatin 40 mg in both carotid and femoral vascular beds. Specifically, in the carotid arteries statins had greater effects on IMT, whereas in the femoral artery plaque modification by statins was more obvious. These findings in the carotid and femoral arteries illustrate the systemic effects of statins on the arterial wall, irrespective of localization.
Footnotes
Acknowledgements
We thank P. Netten, P. Bouter, P. Lestrade, W. Bogers and B. Imholz for assistance with recruitment, A. Theloose, M. Brok, J. Visser, J. den Arend, G. van der Biezen for the ultrasound investigations and T. Terburg and H. van Langen for technical assistance.
This study was financially supported by Parke-Davis B.V., The Netherlands. J.J.P. Kastelein is an established investigator of the Netherlands Heart Foundation (2000D039).