
Abstract
Background
Many studies have analysed the relation between cardiovascular risk factors and oral contraceptive use in adult women, whereas information on the possible health effects of oral contraceptive use during adolescence is lacking.
Design
The effect of current contraceptive pill use on blood pressure and serum total cholesterol concentration was studied in a cross-sectional sample of 120 adolescent girls with a mean age of 17.4 years.
Methods
After the girls had rested for 5 minutes in the sitting position, trained study nurses measured blood pressure three times consecutively using a mercury sphygmomanometer. The nurses also administered a questionnaire gathering information on the use of oral contraceptives, smoking and parental social class. In the morning blood samples were taken for the measurement of serum total cholesterol.
Results
Mean age (± SD) was 17.4 ± 0.8 years. Blood pressure averaged (± SD) 108.7 ± 9.9 systolic and 68.0 ± 8.2 mmHg diastolic. Serum total cholesterol was 4.5 ± 0.7 mmol/l. Forty-nine girls (41%) were taking the contraceptive pill. Of these, 44 (90%) were on a combination of ethinyloestradiol (20-35 μg) and a progestogen, four (8%) on anti-androgens (35 μg) and one (2%) only on a progestogen. After adjustment for age, body mass index, smoking and alcohol status systolic blood pressure was 4.6 mmHg higher (95% CI 1.2-8.1; P<0.001) in current pill users than in girls not currently on the pill (111.4 versus 106.8 mmHg). Adjusted for the aforementioned covariates, diastolic blood pressure was not related to pill use (68.2 versus 67.8 mmHg; P = 0.7). Serum total cholesterol was 0.43 mmol/l (95% CI 0.18-0.60; P = 0.001) higher among girls using oral contraceptives (4.7 versus 4.3 mmol/l), irrespective of whether or not the model was adjusted for age, body mass index, smoking and alcohol status.
Conclusions
In 17-year-old girls, the use of oral contraceptives was associated with a nearly 5 mmHg higher systolic blood pressure and a 0.4 mmol/l higher level of serum total cholesterol. The long-term prognostic implications of our findings remain to be elucidated.
Introduction
Many studies have analysed the relation between cardiovascular risk factors and oral contraceptive use in adult women [1–4], whereas a few publications have focused on the possible health effects of oral contraceptive use during adolescence [5, 6]. As life expectancy increases, women spend approximately one-third of their life in the reproductive phase and the reported prevalence of oral contraceptive use in 15-to-17-year-olds is 21% [5]. The potential impact of oral contraceptive use on cardiovascular well-being is therefore of increasing importance. We investigated whether the intake of low-dose oral contraceptives affects blood pressure and the serum concentration of total cholesterol levels in 17-year-old girls.
Methods
The study was performed in 1999 and was part of a biomonitoring programme to investigate exposure and early health effects of common environmental pollutants in adolescents [7, 8]. Eligible participants were adolescents in their last year of grammar school (in 1999), and who were life-long residents of the control area or the two suburbs, Peer (control area) and Hoboken (study area). Adolescents were enrolled from a large grammar school and interviews and blood samples were taken in a public health centre. Our fieldwork coincided with the school holidays in Wilrijk (study area); we enrolled adolescents from a local examination centre. Of the 355 invited youngsters, 207 (58.3%) agreed to participate. We excluded seven adolescents from the study because they were not immediately available for interview due to illness or holidays. The sample of the 200 participating adolescents consisted of 120 (60%) girls. Of the 120 girls, 49 (41%) were taking the contraceptive pill.
We adhered to the principles described in the Declaration of Helsinki [9]. The Ethics Committee of the University of Leuven approved the study. We obtained written informed consent from the adolescents and their parents.
Experienced study nurses administered questionnaires to assess lifestyle, intake of medications, dietary and smoking habits, consumption of alcohol and social class of the parents. Drinkers were asked how many glasses of alcohol they drank on weekdays and during the weekend. In an additional question drinkers were asked what type of alcohol they consumed. We expressed the alcohol consumption in grams per day. Smoking habits were assessed by a questionnaire. We used a food frequency questionnaire [7, 8] to record information on the intake of meat, fish, eggs, milk and cheese during the year preceding the present study by asking how many times per day, week or month they consumed the abovementioned food categories. We computed the amount of fat intake per day from the recorded food frequencies using mean consumption portions and the Dutch food composition table [10].
Height was measured to the nearest cm (Soenhle, Bolton, UK) and weight to the nearest 0.1 kg (Seca, North Bend, USA). Body mass index was calculated as weight (kg) divided by height squared (m2). Waist and hip circumferences were measured to the nearest centimetre with a tape measure while the subject was standing. Triceps skinfold of the left arm was measured in triplicate using a Harpender caliper providing a constant pressure of 0.01 kg/mm2 (± 10%) at all openings of the 90 mm2 anvils (Siber Hegner, Zurich, Germany).
After the subjects had rested for 5 min in the sitting position the study nurses measured systolic and phase V diastolic blood pressures three times consecutively using a mercury sphygmomanometer (Riester, Jungingen, Germany). The guidelines of the British Hypertension Society were followed [11]. An appropriately sized cuff was applied. The mean of the three measurements was used to classify participants into one of the JNC VI blood pressure categories: optimum (systolic < 120 mmHg and diastolic < 80 mmHg), normal (systolic 120-129 mmHg or diastolic 80-84 mmHg), high normal blood pressure (systolic 130-139 mmHg or diastolic 85-89 mmHg) or high blood pressure (systolic ≥ 140 mmHg or diastolic ≥ 90 mmHg) [12]. If systolic and diastolic blood pressure readings belonged to different categories, the higher of the two readings was used to determine the blood pressure category.
In the morning non-fasting blood samples were taken. Total serum cholesterol and serum triglycerides were determined in duplicate by an enzymatic method using commercially available enzymatic reagents (Olympus System Reagents, California, USA). Certified reference standards were run along each series of study samples. The laboratory participated in the external quality control programme for medical laboratories in Belgium. Hyperch-olesterolaemia was diagnosed according to the guidelines of the Expert Panel on Blood Cholesterol Levels in Children and Adolescents as a serum concentration of total cholesterol equal to or higher than 5.2 mmol/l (≅ 200 mg/dl) [13].
Database management and statistical analysis were performed with SAS software, version 6.12 (Cary, NC). Student's t-test was used to estimate differences between continuous data and χ2-statistics for categorical data. Allowing for the covariates, we looked for differences between subgroups by using analysis of covariance and logistic regression and adjusted these models for age, BMI and smoking and alcohol status.
Results
Compared with the 120 participating girls, the 96 non-participants had similar mean age (17.3 versus 17.4; P = 0.84, and parental social class distribution (low, medium and high, 33.3, 61.5 and 5.2 versus 28.3, 62.5 and 9.2%; P = 0.46).
Comparison of characteristics between oral contraceptive users and non-users
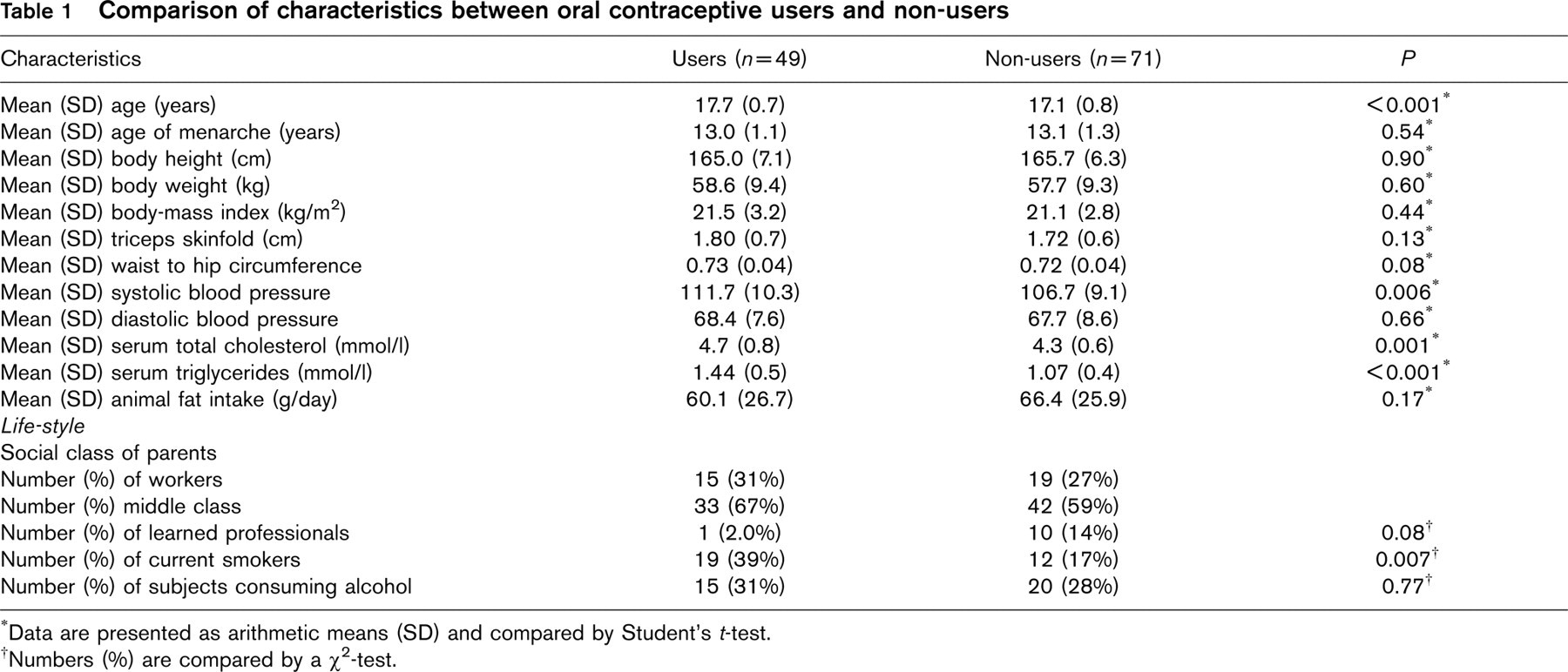
Data are presented as arithmetic means (SD) and compared by Student's t-test.
Numbers (%) are compared by a χ2-test.
The 120 girls were on average (SD) 17.4 (0.8) years old. 49 (41%) were taking the contraceptive pill. Of these, 44 (90%) were on a combination of ethinyloestradiol (20 to 35 μg) and a progestogen, four (8%) on anti-androgens (35 μg) and one (2%) only on a progestogen. The median duration of oral contraceptive pill use was 13.6 months (IQR: 3.8-17.2).
Mean age at menarche, parental social class, the proportion of drinkers, the dietary intake of fat, and all indexes of body fat accumulation were comparable between users and non-users. The age in users was on average 6 months higher than in non-users. Furthermore, in users the proportion of smokers was 58.3% higher (Table 1). In smokers median daily use was 5.5 cigarettes (IQR: 4-12) in 19 users and 6.1 cigarettes (IQR: 4-7) in 12 non-users.
Systolic blood pressure was similar in smokers and non-smokers (109.7 versus 108.4 mmHg; P = 0.52) and drinkers and non-drinkers (109.7 versus 108.4 mmHg; P = 0.50). The corresponding values for diastolic blood pressure were 68.4 versus 66.0 mmHg; P = 0.40 and 69.1 versus 67.5 mmHg; P = 0.35. The single correlation coefficients with systolic blood pressure were positive for body mass index (r = 0.24; P = 0.009) and nonsignificant for age (r = 0.07; P = 0.42), and serum total cholesterol (r = 0.10; P = 0.25). For diastolic blood pressure the correlation coefficients were positive for body mass index (r = 0.21; P = 0.03), and non-significant for age (r = −0.10; P = 0.29) and serum total cholesterol (r= −0.05; P = 0.53).
Mean systolic blood pressure was higher in users compared with non-users (111.7 versus 106.7 mmHg; P = 0.006), while diastolic blood pressure was not related to pill use (68.4 versus 67.7 mmHg; P = 0.7). Sixty two (87%) non-users and 34 (69%) users had optimum blood pressure; six (8%) non-users and 11 (22%) users had normal blood pressure, whereas the remaining 5.8% had high normal blood pressure (three [4%] non-users and four [8%] users) (P = 0.05; Figure 1). None of the participants had a systolic blood pressure higher than 140 mmHg or diastolic pressure higher than 90 mmHg.
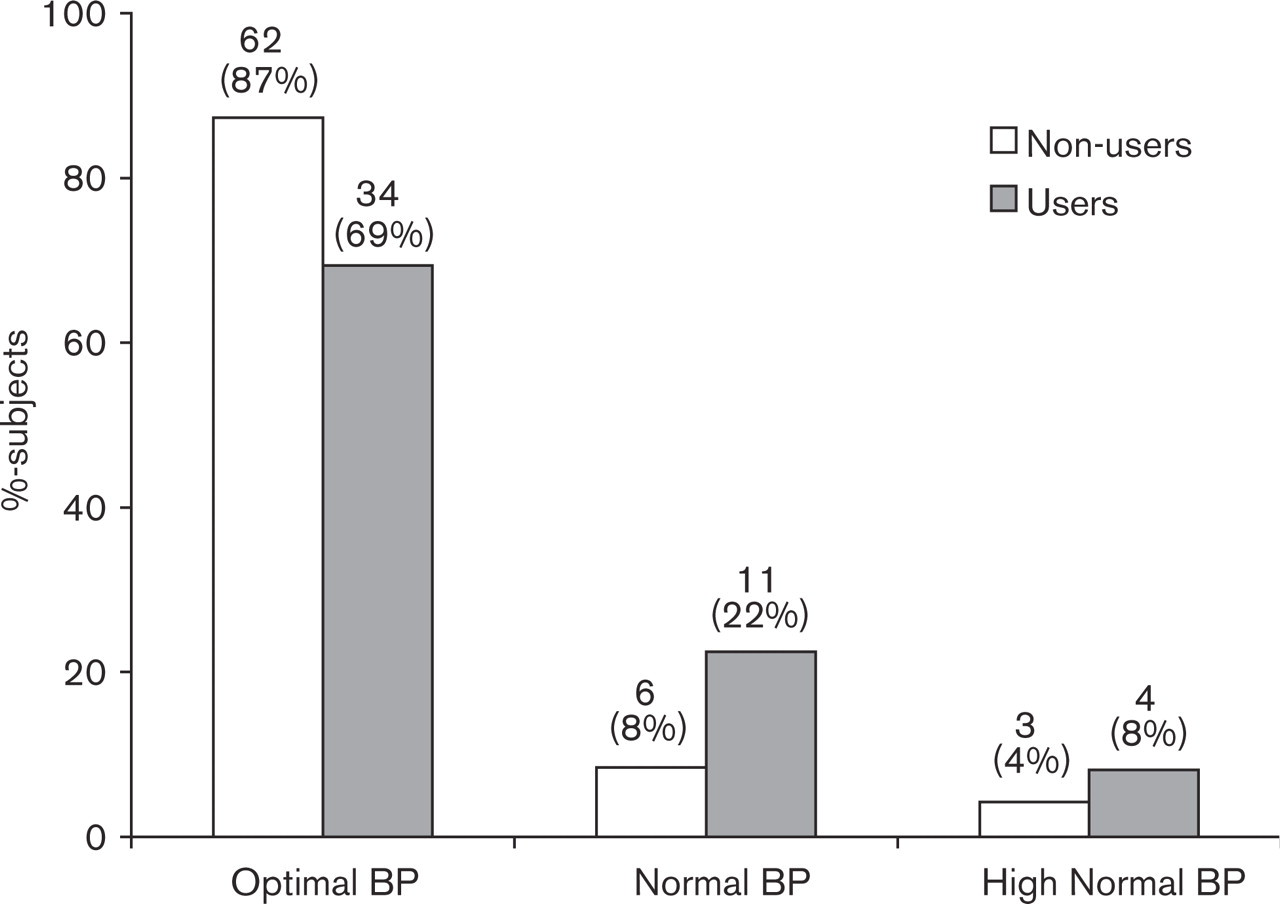
Blood pressure (BP) distribution among oral contraceptive users (n = 49) and non-users (n = 71). Optimum BP (systolic < 120 mmHg and diastolic < 80 mmHg), Normal BP (systolic 120-129 mmHg or diastolic 80-84 mmHg), and High normal BP (systolic 130-139 mmHg or diastolic 85-89 mmHg).
Systolic blood pressure unadjusted and adjusted for age, body mass index, smoking and alcohol status respectively, was 5.0 (Table 1) and 4.6 mmHg (111.4 versus 106.8 mmHg, P < 0.001) higher in girls taking oral contraceptive pills (n = 49) than in 71 not using these pills. However, before (Table 1) and after the aforementioned covariables (68.2 versus 67.8 mmHg; P = 0.77), diastolic blood pressure was not related to pill use. In multiple logistic regression analysis, the odds of not having an optimal blood pressure was 4.27 times higher (95% CI: 1.46-2.5; P = 0.008) in girls currently taking the contraceptive pill, irrespective of whether or not the model was adjusted for age, body mass index, smoking and alcohol status.
Serum total cholesterol was similar in smokers and non-smokers (4.67 versus 4.44 mmol; P = 0.13) and drinkers and non-drinkers (4.43 versus 4.67mmol; P = 0.13). While serum triglycerides were higher in smokers (1.26 versus 1.06 mmol; P = 0.04) but similar in drinkers and non-drinkers (1.17 versus 1.08 mmol; P = 0.37).
Serum total cholesterol and serum triglycerides were higher among girls using oral contraceptives: 4.7 versus 4.3 mmol; P = 0.001 and 1.44 versus 1.07 mmol; P < 0.001, respectively, and irrespective of whether or not these models were adjusted for age, body mass index, smoking and alcohol status. Total cholesterol was above or equal to 5.2 mmol/l in 14 (29%) users and in five (7%) non-users (P = 0.002). The use of oral contraception was associated with a 4.19 (95% CIs: 1.30-3.51; P = 0.017) times higher risk of hypercholesterolaemia, independent of age, body mass index, smoking and alcohol status.
Discussion
Forty-one percent of 17-year-old girls in the current study are on oral contraceptives. Current use of oral contraceptives is associated with an increase in systolic blood pressure by 4-5 mmHg and the total concentration of cholesterol in serum by 0.40 mmol/l.
The increase of nearly 5 mmHg in systolic blood pressure is in agreement with earlier findings in women on contraceptive pills containing higher levels of oestrogens (ethinyloestradiol 50 μg) [14]. This might suggest that adolescent girls are more vulnerable to the pressor effect of oral contraceptives than pre-menopausal women or that the blood pressure increase is independent of the dose of oestradiol. Several mechanisms underlying the pressor action of contraceptives have been proposed which include increases in the plasma levels of angiotensinogen, angiotensin II, aldosterone [15] which in turn may lead to chronic salt retention and expansion of circulating volume leading to higher systolic blood pressure [14–16].
The Royal College of General Practitioners study reported that the incidence of hypertension was 2.6 times higher in oral contraceptive users than in non-users [17]. In our adolescents systolic blood pressure was below 140 mmHg, but the odds of having an optimal blood pressure (systolic < 120 and diastolic < 80 mmHg) was 4.3 times higher in non-users. At the population level, high normal blood pressure (systolic 130-139 or diastolic 85-89 mmHg) is associated with an increased risk of cardiovascular complications [18] and higher incidence of hypertension [19] compared with optimal blood pressure (systolic < 120 and diastolic < 80 mmHg). However, given the low risk of cardiovascular disease in young women, small elevations in blood pressure will have little impact on this short-term cardiovascular prognoses unless other risk factors are present such as familial hypercholesterolaemia [20], smoking [17, 21] or the presence factor V Leiden [22]. Early identification of children at risk for hypertension, proper evaluation, and appropriate management is important to prevent the long-term complications associated with high blood pressure [23]. The long-term use of oral contraceptives throughout the reproductive part of a women's life may in the long term predispose to cardiovascular disease [1, 2, 4, 17, 21]. Most published cohort studies included only middle-aged women and little is known about the risk associated with contraceptive use starting shortly after menarche and sustained until menopause.
The WHO collaborative Study and Royal College of General Practitioners report an increased risk of acute myocardial infarction and stroke in oral contraceptive users and these data suggest that smoking is a major associate of increased cardiovascular risk in oral contraceptive users [17, 21]. In connection to our study approximately 40% of the oral contraceptive users were current smokers compared with 17% of the non-users. This observation was also noted in adult populations as well as in other adolescent populations [5, 6, 24].
Elevated blood levels of lipids are probably the most important biochemical risk factors for atherosclerosis. In the liver triglyceride synthesis is enhanced by oestrogen and inhibited by androgen and these triglycerides are partly brought into the circulation as low-density lipoproteins. Progestogens may have androgen side effects. When a contraceptive pill containing an oestrogen and a progestogen is introduced, the resultant effect is not predictable. Total cholesterol was above or equal to 5.2 mmol/l in 29% of the users and in 7% of the non-users. This cut-off point corresponds to the upper 95th percentile in the American young adult population determined by the pediatric panel of the US National Cholesterol Education Program [25]. The mean difference in serum total cholesterol and serum triglycerides between users and non-users was 0.44 mmol/l and 0.37 mmol/l, respectively. The clinical significance of this observation is supported by the fact that atherosclerosis begins early in life and is accelerated in the presence of high cholesterol and serum triglycerides [26]. In our study only total serum cholesterol and serum triglycerides were measured. Information on other lipid risk factors, such as low-density lipoprotein cholesterol concentration, was not available [27–29].
In conclusion, our study shows that in adolescent girls blood pressure and serum total cholesterol are significantly higher among oral contraceptive users compared with non-users and that oral contraceptive use clusters with smoking. Further studies, especially in larger cohorts, are warranted.