
Abstract
Cigarette smoking kills about six million smokers per year worldwide, and the cigarette has become a symbol of threat to mankind, particularly in industrialized countries. Tobacco smoking causes signs of addiction due to nicotine, but it is the inhaled and exhaled smoke that causes damage to health if cigarette smoking is continued for one or more decades. It is very difficult to attain a high efficacy of stopping smoking using methods of primary prevention in children and young adults. Secondary and tertiary prevention methods use medical and psychological support to the smoker (behavioural and aversion therapy) as well as medical advice in combination with drugs such as nicotine replacement or bupropion. Using a combination of these methods can increase effectiveness up to 45%. Use of nicotine replacement therapy (NRT) in combination with medical advice is the method of smoking cessation recommended by the World Health Organization. Bupropion causes several severe side effects which are not observed with NRT. This article reviews various NRT formulations, including chewing gum, patch, nasal spray, tablet and inhaler, and our experience of using NRT in medical practice, such as adverse events, withdrawal symptoms and the efficacy of NRT in patients with coronary heart disease (angina pectoris, cardiac arrhythmias, etc.), are briefly mentioned. Overall, we need greater efforts in practising primary and secondary prevention among current and future physicians to solve the health problems associated with tobacco use in many nations.
Keywords
Introduction
Smoking already kills one in ten adults worldwide. By 2030, perhaps sooner, the proportion will be one in six, or 10 million deaths per year-more than any other single cause. Until recently this epidemic of chronic disease and premature death mainly affected rich countries, but it is now rapidly shifting to developing countries. By 2020, seven of every ten people killed by smoking will live in low- and middle-income nations [1].
Approximately 1.1 billion people smoke worldwide. By 2025, this number is expected to rise to more than 1.6 billion. Most smokers start young; in high-income countries, about eight out of 10 begin smoking in their teens. Although most smokers in low- and middle-income countries start in their early twenties, the peak age of uptake in these countries is falling [1]. In most countries today, the poor are more likely to smoke than the affluent. This is the situation in Germany [2].
Smoking cessation should be the primary objective of medical treatment for people who smoke, particularly since most smokers who require treatment are dependent on tobacco. Statistics on readiness to quit smoking show wide variations: for some 20-30% of smokers an external event marks the starting point for giving up. A further group of undecided smokers-the figures vary between 25% and 40%-may possibly be persuaded to quit by extensive education campaigns directed at the smoking public [3, 4].
Alongside techniques practised worldwide, in which patient education is mainly combined with pharmacological approaches, a wide range of counselling methods is also employed, ranging from physician advice to psychological withdrawal programmes, such as those used to treat other forms of dependence. Scientific assessment of such techniques is only possible if they adhere to defined standards. The technique used must therefore be scientifically justified or justifiable, and the success of treatment must be quantifiable by measuring biochemical markers (e.g. carbon monoxide [CO] in expired air or, preferably, cotinine levels in plasma, urine or saliva). In addition, the consensus definition of cessation is that the smoker remains abstinent for at least 6 (or preferably 12) months after the start of treatment, that is, the ex-smoker should no longer smoke any cigarettes. A reduction in cigarette smoking (e.g. by 20 cigarettes/day) may be termed a partial success but does not qualify as smoking cessation as defined above. Given the millions of smokers who are potentially willing to quit, the techniques employed must be practicable and economically viable, and this explains the dominant position of nicotine replacement therapy (NRT) worldwide [5].
Smokers often set themselves the goal of giving up smoking, and the factors prompting this decision may be a planned pregnancy [6], a sense of responsibility towards their own children or even financial considerations [7]. A prerequisite for any intervention intended to promote smoking cessation is the development of a strong determination to quit smoking. It may take several weeks before these contemplative processes can be transposed into a practicable reality [8]. This is connected with a behavioural change vis-à-vis smoking [9].
Smokers who think about stopping smoking (‘contemplation’; Stage II) have already moved beyond contented unawareness of the problem (‘precontemplation’; Stage I). They then have to consider how they might handle quitting (preparation phase; ‘deciding to try to quit’; Stage III). Once they stop smoking (‘action’; Stage IV), they have taken a decisive step, but initially they are short-term ex-smokers (‘maintenance’; Stage V) and are constantly at risk of recommencing smoking (‘relapse’; Stage VI). Smokers may find themselves repeating the cycle from Stages II or III to Stage VII several times, depending on how they cope with relapses (Fig. 1). In many cases this short-term abstinence may become ‘sustained abstinence’ (Stage VII). It is important for ex-smokers to extend their abstinence over a period of at least months or even one year or longer; they will then realize that cessation is ‘tough to handle’, and something which preferably they would not wish to repeat.
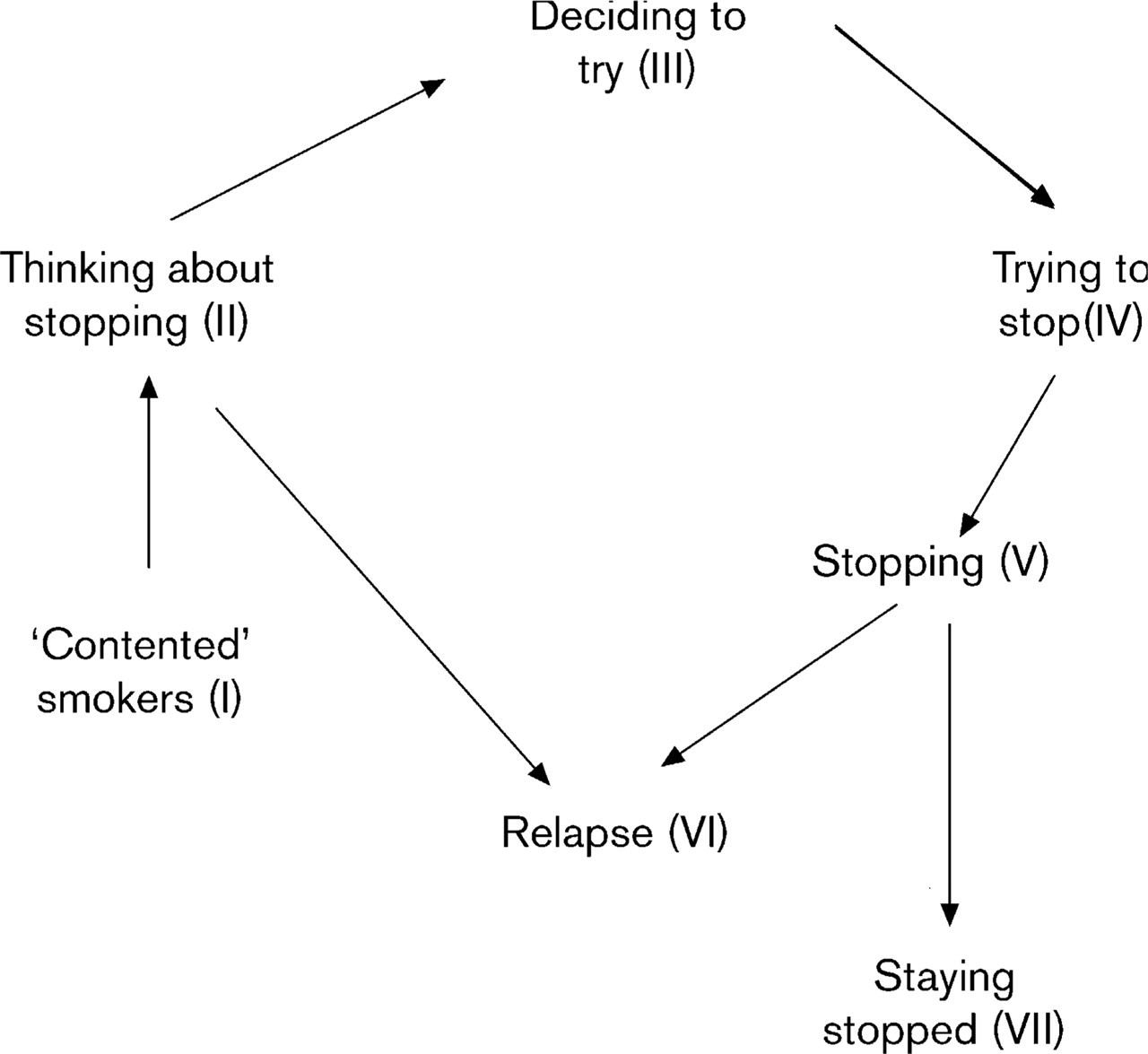
Smoking cessation is a potentially protracted process [9]. The smoker starts in stage I and he can stop smoking (stage V) and staying stopped (stage VII) or relapse (stage VI). He can also decide to try for several times (stage III).
Indications, diagnostic considerations and treatment
In principle, given the numerous, well-known harmful effects of smoking, any intervention to achieve smoking cessation is to be recommended. There are four important indications for smoking cessation:
To prevent a wide range of diseases.
To allow treatment of smoking-related diseases, e.g. chronic obstructive pulmonary disease (COPD), peptic ulcer, hypertension, coronary heart disease, peripheral occlusive arterial disease (POAD), hypercholesterolaemia, diabetes, psychiatric illnesses.
As a component of rehabilitation during recovery from smoking-related diseases (e.g. myocardial infarction, stroke, limb amputation).
To protect non-smokers.
Before treatment starts, smokers should be questioned about the strength of their resolve to quit smoking completely. Their degree of dependence should be assessed [using the Fagerström Test for Nicotine Dependence (FTND)] and, as a minimum requirement, measurements should be taken of CO in expired air (cf. Haustein [10]).
Treatment of the smoker should aim at complete cessation, and stopping smoking abruptly. Fewer than 1-2% of heavily dependent smokers achieve this goal without any medical intervention (i.e. through willpower alone), and the number of cigarettes smoked/day need not be a decisive factor. This method of smoking cessation can be achieved with psychological support, but the outcome is better with pharmacological support.
It is now known that many smokers, because of their heavy dependence and/or considerable habituation, are unable to give up smoking completely, with the result that harm reduction or partial cessation is then a necessary option. The goal here is for smokers (simultaneously patients at risk) to cut their consumption to <10 cigarettes per day with pharmacological support. After a period of reduced cigarette consumption, some smokers may recognize the sense of stopping completely, although this does not automatically imply any change in dependence.
Cigars and pipe smokers comprise only a small portion of smokers and they seldom need help as their dependence is mostly low. The number of dependent smokers of cigarillos is slightly higher, and, if these inhale the tobacco smoke, they can be compared with cigarette smokers and have to be treated like cigarette smokers. All the smokers of cigars, cigarillos and pipes have to be advised like cigarette smokers, and smoking cessation should be achieved by NRT or non-pharmacological methods.
Smoking cessation using non-pharmacological methods
Undoubtedly, the ideal situation is for the smoker one day to decide more or less spontaneously to give up smoking and from that time onwards no longer to smoke cigarettes. This type of decision is commonly taken on special days of the year (e.g. as a New Year's resolution) and, more rarely, is also acted upon. Greater seriousness attaches to decisions that are prompted by personal illness or by the illness or death of a family member or close friend. From our own experience of counselling smokers, we know that even heavy smokers (40 to 60 cigarettes per day) can execute such decisions without major effort. Studies in which self-help interventions led to successful smoking cessation for 6-9 or 12 months are of limited value because biochemical variables were only measured in isolated cases [11]. Smokers whose partners are non-smokers or ex-smokers are more likely to be successful at quitting [12] than those with smoking partners [13]. The support of the spouse may aid success [14, 15], but studies indicating the positive influence of the spouse/partner in this context are countered by others that are critical of their role [16, 17]. Nonetheless, two systematic studies reported the supportive effect of a partner in achieving smoking cessation [18, 19].
Numerous organizations also provide self-help manuals designed to assist smokers who wish to quit [20, 21]. In addition, consulting a therapist may enhance the effectiveness of this method [21]. Standard instructions have been found to be less effective than personalized instructions tailored for a group of smokers [22]. Overall, instructions on smoking cessation are considered useful and more effective than attempting to quit without instructions (Table 1).
Sporting activities are a key aspect of self-help to achieve smoking cessation [23]. Physical exercise has a beneficial effect on cravings [24], depressed mood [25], sleep disturbances [26], feelings of tension [27], stressful situations [28] and on weight gain following smoking cessation, an aspect that is especially important for women [29–31].
The effectiveness of telephone counselling has widely heterogeneous results. In a few studies, telephone counselling was followed by face-to-face counselling. However, telephone counselling can help to prevent further relapses or to stabilize smoking cessation [32].
Assessment of non-drug treatment modalities to promote smoking cessation, compiled from the Cochrane Database [60]
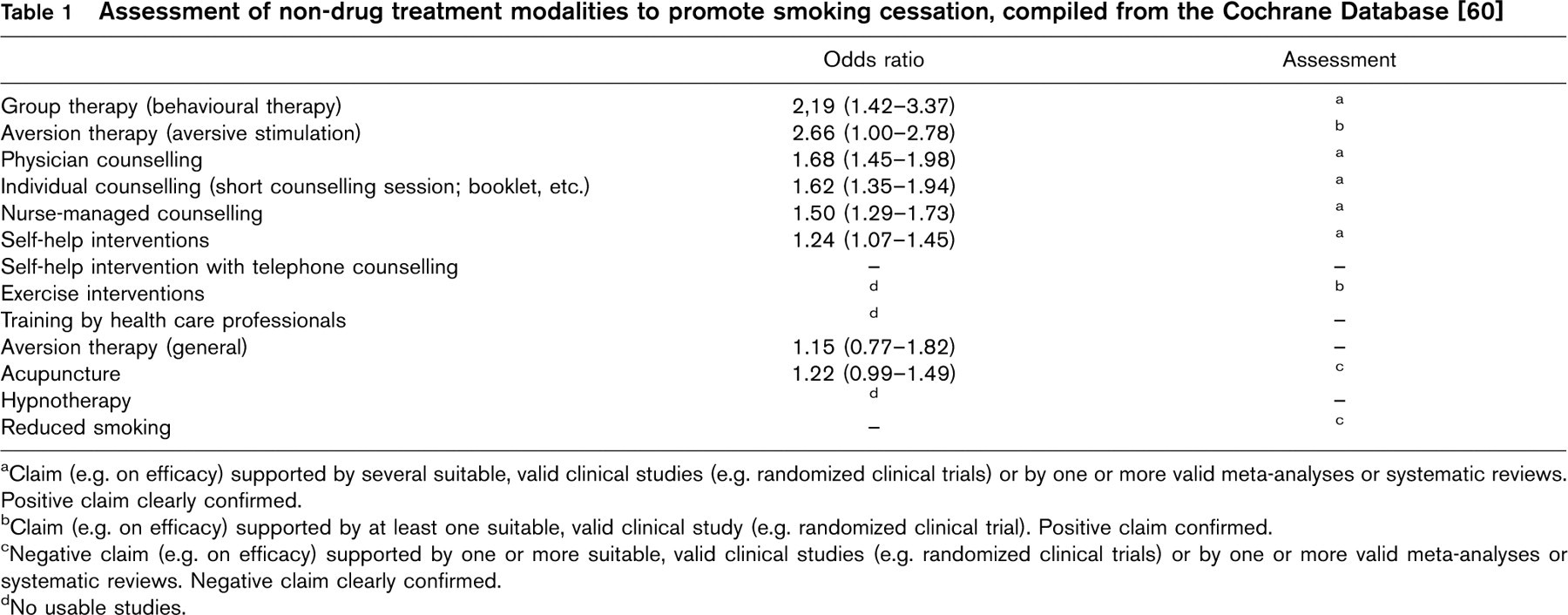
Claim (e.g. on efficacy) supported by several suitable, valid clinical studies (e.g. randomized clinical trials) or by one or more valid meta-analyses or systematic reviews. Positive claim clearly confirmed.
Claim (e.g. on efficacy) supported by at least one suitable, valid clinical study (e.g. randomized clinical trial). Positive claim confirmed.
Negative claim (e.g. on efficacy) supported by one or more suitable, valid clinical studies (e.g. randomized clinical trials) or by one or more valid meta-analyses or systematic reviews. Negative claim clearly confirmed.
No usable studies.
Physicians' advice for smoking cessation
Different studies used 5-min standard interviews to point out the dangers of smoking and issued smokers with an information booklet without offering any further consultation. The studies revealed no clear differences in terms of success, even when biochemical markers were measured (plasma nicotine levels or expired CO). The studies that involved additional physician input (spirometry, CO measurement, oral or written medical counselling, post-cessation support or a combination of interventions), achieved different success outcomes, which were also attributable to-among other things-non-standardized methods and individually tailored physician input in the individual studies.
Clinicians achieved a 35% success rate in group sessions with high-risk patients with coronary heart disease [33] who had survived a myocardial infarction. Even higher success rates were recorded in one uncontrolled study [34]. In further studies, where counselling was made available to high-risk smokers with no history of infarction [35, 36], success rates for smoking cessation ranged from 7 to 31.3%. Where smokers were simply counselled to stop smoking, success was no lower than the other three studies which employed additional interventions such as repeated reminders of the risk of infarction, support for successful smoking cessation, etc. [35, 36] (21% success rate; P < 0.001). A change in smoking habits (from cigarettes to cigars or pipes) was reported in one study [37].
Nursing involvement
As nurses constitute a much larger professional body than physicians worldwide, training efforts are warranted to qualify nursing staff for involvement in smoking cessation programmes, given the enormity of the task. However, counselling by nursing professionals is reported to be less effective than physician counselling [38]. Two different [39, 40] studies of nurse intervention can be considered successful, although some investigators also used NRT to promote smoking cessation. Among post-infarction patients who took part in nurse-managed programmes in a cardiology clinic, effectiveness was much greater [30, 38, 41].
Overall, counselling by trained nursing professionals may be regarded as useful, with statistically significant - although moderate effects - achieved to date [42]. In selected hospitals and outpatient departments, nurses should therefore be involved in patient education to promote smoking cessation [43].
Group behaviour therapy programmes
Dependence experts and psychiatrists in particular consider that behaviour therapy programmes are very effective in promoting smoking cessation [40, 44]. The hypothesis that smoking is a learned and consolidated behaviour based on many years of conditioning has prompted the development of treatment strategies using the same practices to ‘unlearn’ the resultant dependence.
Aversion therapy
Aversion therapy is based on pairing the ‘pleasurable’ event with an unpleasant physical stimulus. It may be regarded as a form of behavioural therapy designed to correct certain behaviours such as dependence (e.g. on cigarettes or excessive eating) [45].
Mass media communication strategies
Over the past 10-15 years several attempts have been made to influence smoking behaviour among the wider population via the mass media. Television, cinema, radio broadcasts, print media of all types, posters, personal discussions, smoker helplines, and even personal direct mailings have been utilized for this purpose. These campaigns either communicated factual information or took the form of appeals; they also employed a counter-advertising strategy, tantamount to a condemnation of the tobacco industry's marketing strategies. When assessing the usefulness of such methods, the decisive factor is the achievement of smoking cessation (or at least a definite reduction in smoking) over a period of several (≥6) months). Experience from Australia and the UK [46, 47] indicates that these campaigns [48] showed initial successes in terms of smoking cessation, with the combination of TV plus radio proving to be beneficial and having a lasting effect [47].
Hypnosis
Hypnosis is a suggestive technique that aims to overcome short-term withdrawal symptoms and to cancel out the cues for smoking. Hypnotherapy lacks any capacity to prevent relapse and does not help smokers to cope with cravings [24, 49].
Acupuncture
A review of 18 studies of the efficacy of acupuncture found that only one showed a significant effect after 12 months [50]. In a comparison of studies using objective criteria, acupuncture was not superior to sham acupuncture in terms of achieving smoking cessation [51–54].
Reduced smoking
Gradual reduction of the nicotine dose administered in cigarettes has been tested as a method of promoting smoking cessation. The statistically non-significant success rate associated with this technique was 5% on average [55–57]. Methods based on smokers' intentions to quit by gradually reducing consumption or other related techniques (e.g. using filter tips of differing lengths) are not workable.
Pharmacotherapy for tobacco dependence
Pharmacotherapy to promote smoking cessation has been investigated in recent decades using a variety of medicinal products: currently, the most commonly employed method, and that recommended by the World Health Organization, involves the use of nicotine replacement medications (for review, see [10]). Although the antidepressant drug bupropion has been approved as an aid to smoking cessation since 2000, little experience of its use has been gained to date in Germany and several other EU countries. All other pharmacological agents have either not fully proved their usefulness or else, like bupropion, whose efficacy has been demonstrated, require further investigation because of a smaller risk-benefit ratio than that with NRT. Consensus papers on the treatment of tobacco use and nicotine dependence have recently appeared in the USA [58, 59] and, along with the review publications of the Cochrane Tobacco Addiction Group [60], these have formed the basis for treatment recommendations in other countries and have provided a major stimulus to the formulation of German recommendations (Table 2).
Nicotine replacement
During the last 20 years, NRT has been used by some 30 million smokers: NRT has been tested in over 34800 smokers in more than 108 studies and these have been reviewed in several meta-analyses [19, 61, 62]. Treatment of the dependent smoker with NRT (in the form of transdermal patches, chewing gum, nasal sprays, sublingual tablets or oral inhalers) can therefore be implemented without any concerns about safety (Table 2).
Smokers with severe ‘physical’ dependence derive the greatest benefit from using NRT. However, a heavy smoker (e.g. 20-30 cigarettes per day) is not automatically a dependent smoker. The following criteria should be applied when initiating treatment with NRT products:
Daily cigarette consumption.
Deep and frequent inhalation on the cigarette.
Increased CO levels measured in expired air.
Difficulty not smoking in response to ‘external compulsions’.
A score of ≥3 points on the FTND [63].
Assessment of treatment methods to achieve smoking cessation (also based on the treatment recommendations on smoking cessation issued by the Pharmaceutical Commission of the German Medical Profession) [10]
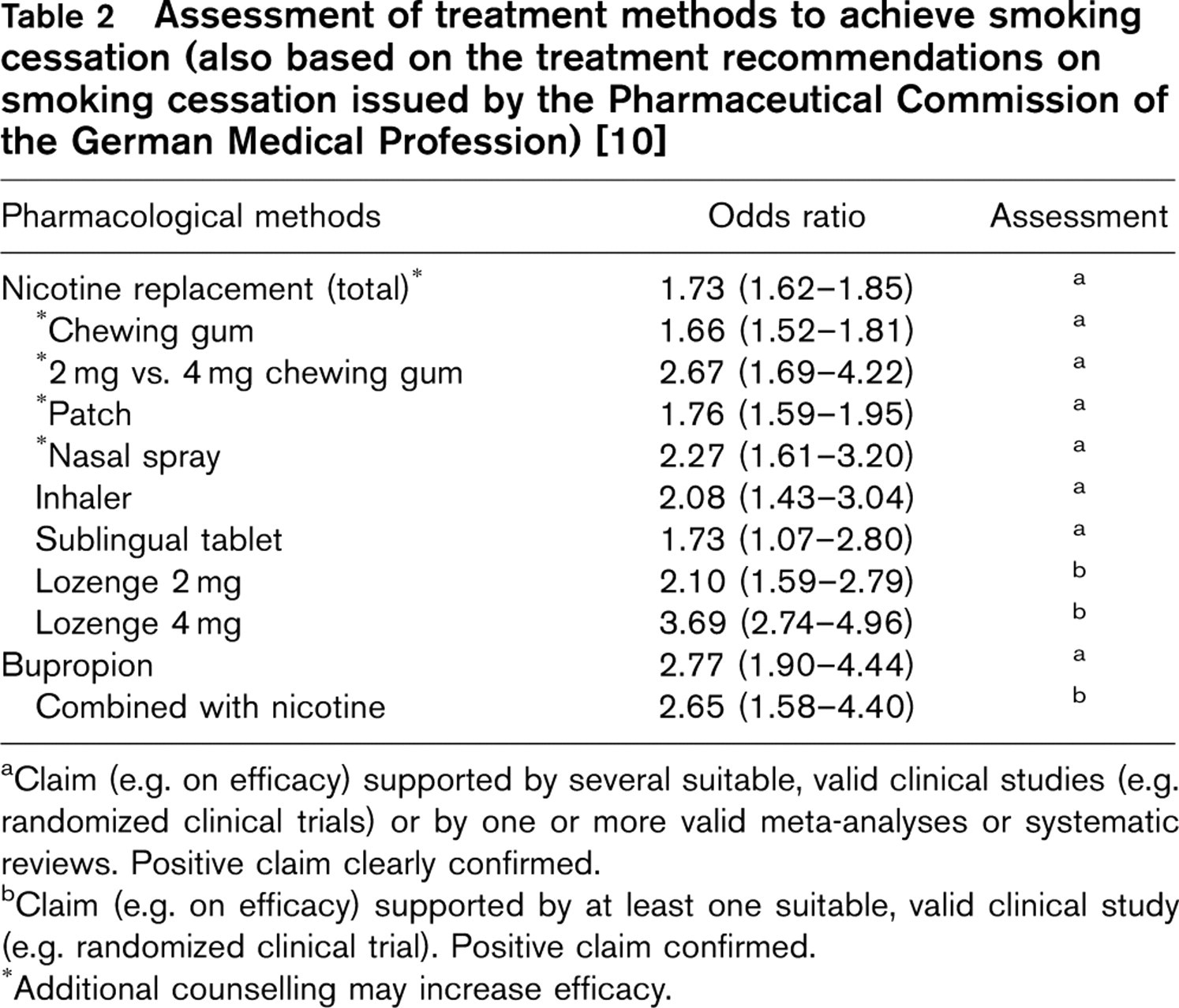
Claim (e.g. on efficacy) supported by several suitable, valid clinical studies (e.g. randomized clinical trials) or by one or more valid meta-analyses or systematic reviews. Positive claim clearly confirmed.
Claim (e.g. on efficacy) supported by at least one suitable, valid clinical study (e.g. randomized clinical trial). Positive claim confirmed.
Additional counselling may increase efficacy.
Evaluation of nicotine products
Nicotine products are licensed as aids to smoking cessation, for the relief of withdrawal from tobacco dependence. Cigarette smoking, with its bolus-like delivery to the brain, is the most reinforcing and dependence-producing form of nicotine administration [64]. The rationale for NRT is that the various formulations alleviate withdrawal symptoms by providing an alternative source of nicotine. Initially, after quitting smokers continue to use nicotine, at a reduced dose and slower speed of nicotine delivery, while coping with the loss of the behavioural side of their dependence. Several weeks later, smokers then break the nicotine dependence by discontinuing their NRT.
In its analysis of the now numerous publications on the efficacy of NRT in smoking cessation, the Cochrane Tobacco Addiction Group includes only trials which are placebo-controlled or comparator-controlled (pharma-cotherapy or non-drug therapy) and which assess smoking cessation by stating the number of ‘failures’ over a follow-up period of 6 months or longer [65]. These studies also employed objective criteria, such as measurements of plasma nicotine concentrations, expired CO levels, etc. (Table 2).
Additional individual counselling of patients helps to increase the success rate. In terms of duration of treatment, one study showed that an 8-week course of treatment with nicotine patches was just as effective as longer treatment periods [66].
Nicotine chewing gum was the first type of NRT to become widely available. Nicotine is absorbed directly through the buccal mucosa, resulting in plasma concentrations which are approximately half those produced by smoking a cigarette [67]. Both 2 and 4 mg preparations are available in many countries, and these are generally available over-the-counter. Several factors, including oral and gastric side effects, and dental prostheses etc., limit the usefulness of nicotine gum in some smokers [68]. The advantage of nicotine chewing gum over the patch is that its dosage can be adjusted individually throughout the day in response to any cravings that may be experienced.
Nicotine patches were developed as transdermal delivery systems to ensure constant release of the active ingredient over a period of 16 or 24 h. The success rates do not differ depending on whether the patch remains on the skin for 16 or 24 h a day [69–71]. The patch should be applied to a dry area of hairless skin, and the application site should be varied daily. A nicotine patch containing 24.9 mg nicotine (Nicorette®) releases 0.9 mg per h during the duration of use. The Nicorette® patch is designed to be worn for 16 h (daytime only) whereas NiQuitin® and Nicotinell® patches administer nicotine over a 24-h period. Due to the pharmaceutical formulation of NiQuitin®, incorporating a membrane type that releases nicotine for transcutaneous delivery, the patches contain 36, 78 and 114 mg nicotine in patch sizes of 7, 15 and 22 cm2, respectively. The Nicotinell® patch contains 52.5 mg nicotine in an area of 30 cm2. During the first 2 h after patch application, differences in plasma nicotine levels have been detected in terms of body area selected (chest > leg > back > gluteal region) but differences observed between application sites are not clinically relevant.
Nicotine attains maximum plasma concentrations between 4 and 10 h following single patch application, and levels then plateau over 16-24 h. With the 24-h patches, significant differences exist between the single-dose and steady-state area under the concentration-time curve (AUC) values and the mean plasma concentration curve. In contrast, the 16-h patch has similar plasma concentrations during steady state and after a single dose, as the plasma level declines during the night. Metabolism of nicotine to cotinine during transdermal passage is estimated to be minimal. Plasma nicotine concentrations rise if cigarettes are smoked while wearing the patch.
Nicotine sublingual tablet is a formulation that is intended particularly for smokers who want to give up smoking but who do not like or cannot use chewing gum [72]. Approximately 50% of absorption from the 2 mg tablet occurs through the buccal mucosa, but the tablet should be placed and held under the tongue.
Nicotine nasal spray is the NRT formulation that allows the most rapid absorption of active ingredient (through the nasal mucosa), thus enabling cravings to be relieved more effectively than with nicotine chewing gum. The nicotine inhaler consists of a plastic housing with a mouthpiece designed to hold a disposable porous cartridge impregnated with 10 mg nicotine. When the user draws air into the mouth through the inhaler, nicotine from the cartridge is vaporized. At room temperature, 13μg nicotine is released by one draw on the 10 mg inhaler [73]. In total, approximately 4mg is absorbed from a 10 mg inhaler during 20 min of intensive use; a maximum of 50% is available to the systemic circulation and the inhalation technique - buccal (shallow puffing) or pulmonary (deep puffing) - is of marginal importance in terms of the dose and steady-state plasma concentrations achieved. A 2 and 4 mg nicotine lozenge have recently been introduced. Compared with the analogous gum formulations, the lozenges deliver 25 to 27% more nicotine than the gums if the AUCs are measured [74]. In one efficacy study, the two lozenge strengths were allocated to smokers depending on their grade of dependency (assessed using the FTND) [74].
Treatment and dosage NRT is the appropriate treatment to help the dependent smoker to achieve smoking cessation. Its effectiveness is increased two- to threefold if the smoker is motivated to stop. Although nicotine patches are more convenient to use than chewing gum or nasal spray, they are less effective for the relief of cravings, particularly when compared with nasal spray. A few studies have been published on the combined use of two different nicotine formulations (patch + chewing gum or nasal spray or inhaler) [65]. Suppression of cravings is the crucial issue with regard to failure in many dissonant ex-smokers once smoking cessation therapy has commenced, and medical management has a pivotal role to play during smoking cessation therapy [65].
Our own experience with NRT, on the basis of treating more than 1200 smokers, is set out schematically in Table 3. The treatment schedule cannot be rigidly defined because, while the level of dependence can be identified, it is shaped by the patient's personality, including his/her own willpower, and the therapist must repeatedly expect the unexpected.
Experiences of using medical support plus NRT In an open, prospective study 217 smokers willing to stop smoking were enrolled over a 15-month period [75]. Complete cessation from smoking was planned with the aid of medical support and nicotine replacement medications (patch, chewing gum, nasal spray) used for 6 months. Smoking behaviour was evaluated using expired CO levels. Treatment was on an individual basis, and most subjects used a combination of two nicotine formulations to suppress craving. During a 3-month period, subjects attended an average of 6.6 consultations, with a follow-up at 6 months. Thirty-nine (17.3%) of the 217 participants attended only one counselling session (‘visitor’). The remaining 178 participants voluntarily followed our treatment plan, but 107 (49.3%, ‘leavers’) stopped attending the consultations before completing treatment; only 73 participants (33.6%, ‘ex-smokers’) were treated for the full 6 months. On an ‘intention-to-treat’ analysis, the success rate was 33.6%. Excluding the ‘visitors’ who absented themselves from the study after one session gives a success rate of 41.0%. Atotal of 155 adverse events were observed during the study but these were mild or moderate, with the exception of one case (nose bleed) that necessitated a switch from nasal spray to chewing gum. The high abstinence rate was achieved by a combination of medical advice plus NRT, suggesting that this method represents the optimal treatment of dependent smokers.
Stepwise schedule for smoking cessation with nicotine products [patch with transdermal release of 0.9 mg nicotine/h, 4 mg chewing gum, nasal spray containing 0.5mg/spray (1 mg/dose) and sublingual tablet containing 2mg] [10]. The level of dependence is classified in four grades
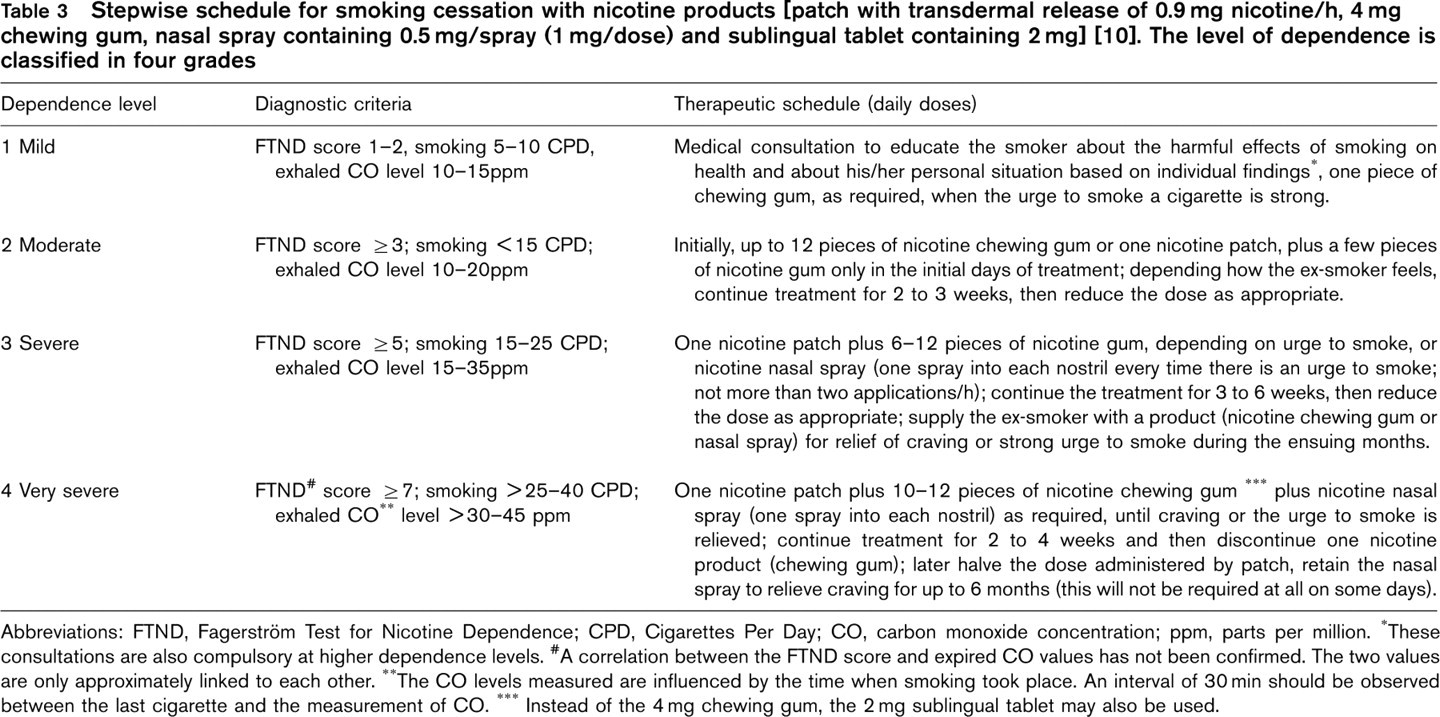
Abbreviations: FTND, Fagerström Test for Nicotine Dependence; CPD, Cigarettes Per Day; CO, carbon monoxide concentration; ppm, parts per million.
These consultations are also compulsory at higher dependence levels.
A correlation between the FTND score and expired CO values has not been confirmed. The two values are only approximately linked to each other.
The CO levels measured are influenced by the time when smoking took place. An interval of 30min should be observed between the last cigarette and the measurement of CO.
Instead of the 4 mg chewing gum, the 2 mg sublingual tablet may also be used.
Adverse events associated with NRT Symptoms of nicotine toxicity range from nausea, abdominal pain and vomiting, dizziness and headache to dyspnoea, convulsions and respiratory failure. Regular cigarette smokers develop tolerance to many of the effects of nicotine, and stopping smoking is associated with various nicotine withdrawal symptoms including dysphoria, irritability, anxiety, difficulty concentrating, restlessness, insomnia, decreased heart rate and increased appetite. Some effects associated with NRT products are withdrawal symptoms, rather than adverse events.
Withdrawal symptoms vary in severity from person to person and may last for several weeks or months. Like alcoholics, many ex-smokers are at high risk because the least cause (going to a restaurant and having an alcoholic drink, meeting up with smokers, stressful situations) may trigger a return to smoking. Many smokers, however, ‘merely’ miss the manual cues associated with the activity of smoking. Withdrawal symptoms are commonly misinterpreted as adverse events of NRT, especially where the symptoms are psychological in nature.
Nicotine formulations as over-the-counter products Various nicotine formulations are sold as over-the-counter (OTC) products in several European countries (e.g. patch and gum in Germany). The rationale for permitting OTC availability is that smokers absorb nicotine from cigarettes in higher doses, and develop higher blood levels than following administration of NRT products. The current regulatory framework restricts access to NRT without adequately considering that the likely consequence will be continued dependent use of nicotine-containing tobacco, which is universally available and extremely harmful. With the aim of reducing harm in adolescents, pregnant women and patients with cardiovascular diseases or diseases of the respiratory tract (e.g. COPD) who smoke, these categories of tobacco users should be permitted to use NRT for smoking cessation, or - if they are unable to quit - to reduce their daily cigarette consumption to less than 10 cigarettes per day. A critique of the current regulatory situation in the UK has recently been published [76].
Worldwide, NRT must become more accessible to smokers by removing regulatory barriers (e.g. France, Australia, Brazil), and early results suggest a favourable public health impact [77].
Bupropion
The effectiveness of bupropion exceeds (non-significantly) that of nicotine products (cf. Table 2) [78]. Placebo-controlled, long-term studies have revealed no convincing differences in efficacy after 1 [79] or 2 years [80]. Relapse to smoking could not be prevented after treatment for 1 year [80], and the mean changes in body weight in the bupropion group differed from the placebo group by 1.3kg after 2 years [80]. In terms of a risk-benefit calculation, people who have smoked for two or three decades may feel ‘healthy’ and have to be convinced to stop smoking, or they may feel ‘ill’ but be unable to stop smoking because they are addicted. Where present, the risk of adverse events and deaths [81] with bupropion is greater and more serious than with NRT [82]. Because of the potentially severe adverse events, bupropion should therefore be considered as second-line rather than first-line medication for aiding smoking cessation [82].
Special therapeutic situations
Ischaemic heart disease
The two controlled studies conducted to date in patients with stable angina point to a favourable influence of benefit on progression or on the course of the disease. In smokers (>20 cigarettes per day) with coronary heart disease, blood flow in various myocardial regions was improved as a sign of ‘smoking reduction’ when cigarette consumption was replaced in part by nicotine patches (14 and 21 mg strengths) [83]. With falling CO content of expired air, the under-perfused myocardial regions were reduced in size, and the patients’ exercise capacity was increased despite higher nicotine levels (compared with controls), because cigarette consumption had decreased. One study indicated that nicotine had a ‘minimally harmful’ effect on the circulation, because even years of smokeless tobacco use did not increase either the risk factors for the development of coronary heart disease or the atherogenic index [84].
When cigarette consumption in patients with stable angina who were using nicotine patches (14 and 21 mg) was gradually reduced from >20 to <7 cigarettes per day, only three out of 77 smokers in the active treatment group compared with eight out of 79 smokers in the placebo group discontinued treatment due to cardiovascular events [85]. Transdermal nicotine administration does not increase either the frequency of angina attacks or the occurrence of nocturnal attacks, arrhythmias or episodes with electrocardiogram evidence of ST-segment depression [85]. In this study, smoking cessation was achieved in 36 and 22% of patients (active treatment versus placebo) [85]. Thus the usefulness of NRT has been confirmed in smokers with stable angina. Recommendations have now also been published concerning the treatment of ischaemic heart disease [86], indicating that nicotine patches clearly reduce the primary endpoints (death, myocardial infarction, cardiac arrest, hospital admission, cardiac arrhythmias or heart failure) within 14 weeks in patients with coronary heart disease (5.4 versus 7.9%, active treatment versus placebo) [86]. Nicotine treatment may thus be initiated as early as 2-3 days after an acute myocardial infarction, and NRT may be used for smoking cessation in all patients with angina pectoris and cardiac arrhythmias.