
Abstract
Background
The prognostic significance of left ventricular hypertrophy (LVH) identified by simple electrocardiographic (ECG) criteria in high-risk patients with established cardiovascular (CV) diseases is not clearly understood.
Design and methods
The Heart Outcomes Prevention Evaluation (HOPE) trial was a randomized trial, which evaluated the effects of ramipril and of vitamin E on major CV outcomes in 9541 men and women aged 55 years or older with a history of coronary artery disease, stroke, peripheral vascular disease or diabetes mellitus with at least one additional CV risk factor. Patients were followed for an average of 4.5 years. We evaluated the association between simple ECG criteria for LVH and the risk for major vascular events, for CV and all-cause mortality and for heart failure.
Results
Electrocardiographic LVH was present in 793 (8.3%) HOPE study participants. Of these, 19.0% sustained a major CV event (MI, stroke or CV death), 15.6% died and 6.1% developed heart failure compared with 15.6%, 10.8% and 2.9% respectively of those without ECG-LVH (P = 0.0023; P < 0.0001 and P < 0.0001). In multivariate analysis ECG-LVH was an independent predictor of CV and all-cause death and of heart failure.
Conclusions
In patients with CV disease simple, easily applicable ECG criteria for LVH identify a subset of individuals at particularly high risk for death and for heart failure.
Keywords
Introduction
The electrocardiographic (ECG) pattern of left ventricular hypertrophy (LVH) is a common response to hypertension, coronary artery disease (CAD), valvular disease and cardiomyopathies [1]. In hypertension, LVH develops in response to sustained pressure overload [2], while after myocardial infarction (MI) the left ventricle (LV) compensates for the function of the lost myocardium, by chamber dilation and hypertrophy of non-infarcted segments [3]. In addition to being a common adaptive mechanism to increased haemodynamic loading conditions, LVH can develop also as a consequence of sustained activation of neurohormonal systems, such as the renin-angiotensin-aldosterone and the adrenergic systems, increased levels of insulin, growth hormone, thyroxine and glucagon [1–4]. Some of these neurohormonal systems are often activated in atherosclerosis, even in the absence of hypertension or prior MI. Thus, LVH can develop in a variety of patients with atherosclerotic vascular disease and, while traditionally considered a direct marker of sustained haemodynamic and neurohormonal stresses on the myocardium, its presence implies that such stimuli are indeed present and may exert adverse effects on the entire vascular system. Therefore, LVH may identify a wide range of individuals at increased risk for various adverse cardiovascular (CV) outcomes.
Population-based studies and studies in hypertensive cohorts have shown that ECG-LVH is independently associated with increased incidence of CAD and with CV and all-cause mortality [5–25]. There are insufficient data, however, regarding the prognostic significance of ECG-LVH in high-risk individuals with existent CV disease or those with other markers of high risk. The few available studies suggest increased mortality rates in CAD patients with ECG-LVH [10, 26, 27]. These studies have been generally too small to provide reliable estimates of risk associated with ECG-LVH, are relatively old and often do not incorporate therapies commonly used at present in the management of such patients. Moreover, the prognostic relevance of LVH in other subsets of patients with CV disease remains unknown.
Similarly, while ECG-LVH was shown to be a marker of increased risk of heart failure and of stroke in the general population [6, 9, 13, 28], there are no reports evaluating whether this applies also to a high-risk population with existent vascular disease. Furthermore, previous studies have often used complex criteria for the ECG diagnosis of LVH, limiting their clinical applicability.
We therefore evaluated the prognostic significance of simple ECG criteria for LVH in the Heart Outcome Prevention Evaluation (HOPE) study in 9541 high-risk patients on a range of CV outcomes. Because of the large number of outcome events (> 1500 major CV events) and the diversity of the population studied, precise estimates of risk for specific outcomes were obtained overall and in key patient subgroups.
Methods
Study Population
HOPE was a multicentre, randomized double-blind placebo-controlled trial, which evaluated the effects of long-term therapy with the angiotensin-converting enzyme (ACE) inhibitor ramipril and with vitamin E in patients at high risk for adverse CV outcomes. The study design, patients' baseline characteristics and the main study results have been reported [29–31]. Briefly, the HOPE trial included women and men aged 55 years and older with a history of high-risk CAD, stroke, peripheral arterial disease (PAD) or diabetes mellitus with at least one additional CV risk factor (hypertension, elevated total cholesterol and/or low high-density lipoprotein cholesterol concentration, cigarette smoking, or microalbuminuria). Patients were excluded from the trial if they had heart failure or known impaired LV systolic function (ejection fraction <40%), uncontrolled hypertension, significant valvular disease, renal disease or major non-cardiac illness.
Definition of electrocardiographic left ventricular hypertrophy
All patients had a 12-lead ECG at randomization. Criteria for ECG-LVH were specified in the study protocol and all ECG tracings were interpreted at each HOPE study centre by the site principal investigator using these criteria. LVH was considered to be present, if the sum of the S wave in lead V1 and the R wave in lead V5/V6 exceeded 35mm (the Sokolow-Lyon voltage criteria) [32]. LVH with LV strain and LVH with left axis deviation were defined as present, if in addition to the above voltage criteria there was ST segment depression and T wave inversion in the anterolateral precordial leads V5 and V6, or the QRS axis was between −30° and −120°, respectively. To keep the definition simple and the results easily applicable, only the voltage criterion, regardless of the presence or absence of LV strain and/or left axis deviation (i.e. any LVH), was used for the main analyses (Tables 1–3 and Figure 1). LVH with strain and LVH with strain and with left axis deviation were evaluated in subgroup analyses.
Follow-up and outcomes
Follow-up information was gathered as previously detailed [29–31]. Following randomization patients were seen after 1 month and thereafter at 6-month intervals. The primary HOPE study outcome was defined as the composite of MI, stroke and death from CV causes. Among the predefined secondary HOPE study outcomes were all-cause death and hospitalizations for heart failure. An Events Adjudication Committee blinded to treatment assignment adjudicated all primary and secondary study outcomes. The committee reviewed source documents and used pre-defined criteria for the ascertainment of the study outcomes. These have been previously described [29–31].
Baseline characteristics of patients with and without LVH on baseline ECG
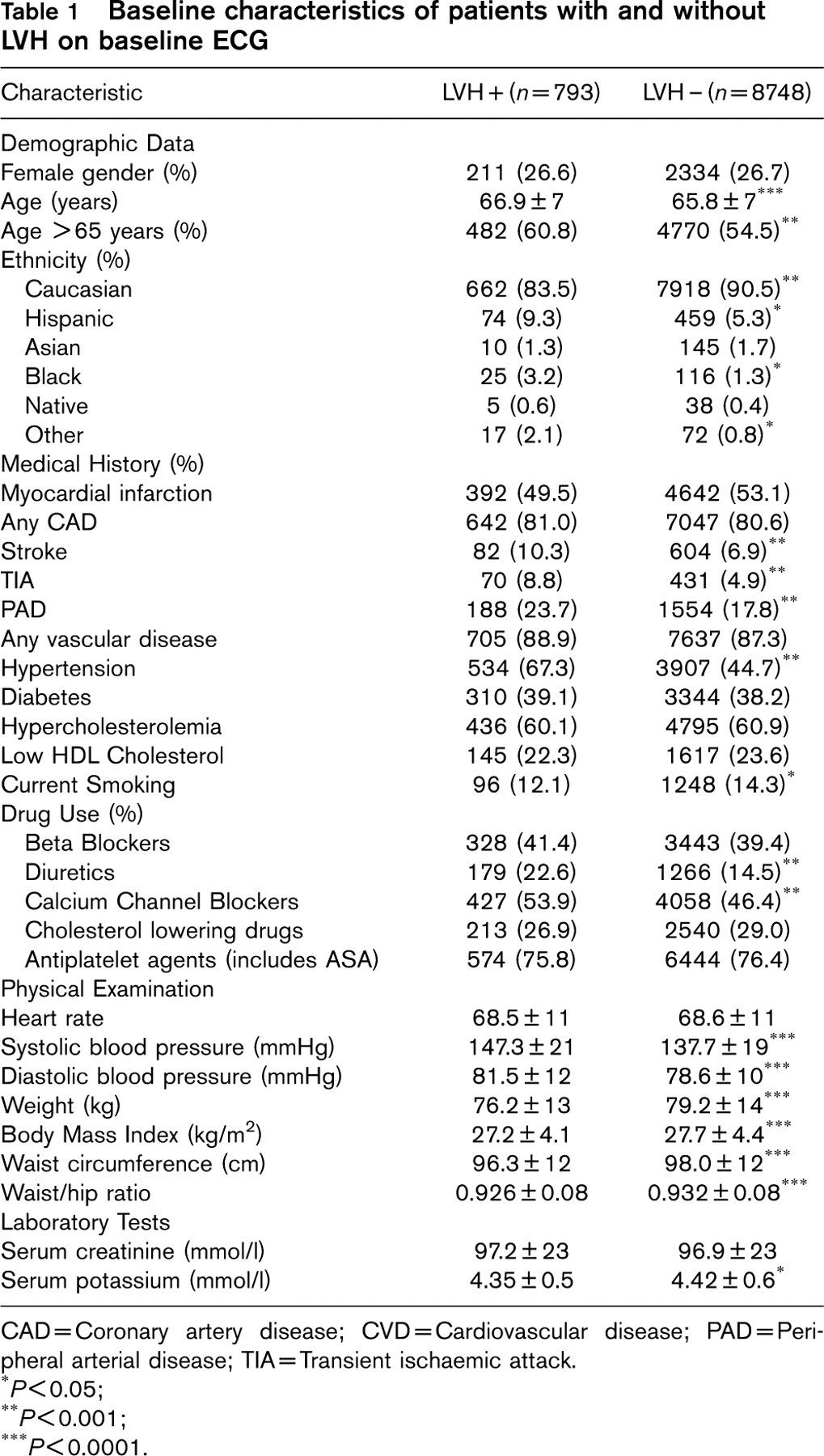
CAD=Coronary artery disease; CVD=Cardiovascular disease; PAD=Peripheral arterial disease; TIA=Transient ischaemic attack.
∗P<0.05;
∗∗P<0.001;
∗∗∗P<0.0001.
Statistical analysis
Baseline characteristics of patients with and without ECG-LVH were compared using the chi-square test for proportions and the Student t-test for continuous variables. For the purposes of this study, that is, the evaluation of the prognostic significance of ECG-LVH, we defined a priori as outcomes of interest the primary HOPE study outcome, that is, the composite of MI, stroke and death from CV causes, each of its components, all-cause death, and hospitalizations for heart failure. Survival curves for the outcomes of interest were estimated according to the Kaplan-Meier procedure for patients with and without ECG-LVH and compared using the log rank test. Cox regression analyses were used to calculate the relative risks (RR) and 95% confidence intervals (CI) associated with ECG-LVH. These risk estimates were also computed in analyses adjusted for age and gender and in multivariate models, in order to evaluate the independent contribution of ECG-LVH to CV risk. We used two multivariate models, one model controlling for age, gender, history of hypertension and baseline systolic blood pressure and a second model controlling for age, gender, history of CAD, MI, diabetes mellitus, hypertension, current smoking, dyslipidaemia, baseline systolic and diastolic blood pressure, body mass index, use of antiplatelet agents, beta-blockers and calcium channel blockers, diuretics and treatment assignment to active ramipril. Cox regression analyses were also used to estimate the RR and 95% CI associated with ECG-LVH in predefined, clinically relevant subgroups. All analyses were performed using the SAS software, version 8.0.
Results
A total of 9541 individuals, 2545 (26.7%) women and 6996 (73.3%) men were enrolled into the HOPE study between December 1993 and June 1995. Their mean age was 65.9 ± 7 years and most study patients were Caucasian, 8580 (89.9%). At study entry there were 8342 (87.4%) patients with documented CV disease (including CAD, cerebrovascular and/or PAD), 7689 (80.6%) with CAD, 5035 (52.8%) with prior MI, 1187 (12.4%) with prior stroke or TIA, 1742 (18.3%) with PAD, 4441 (46.5%) with a history of hypertension and 3654 (38.3%) with a history of diabetes. A detailed review of patients' baseline characteristics has been previously published [30]. Mean follow-up was 4.5 years. Vital status was ascertained at the end of the study for 99.9% of study participants.
Electrocardiographic diagnosis of LVH
Left ventricular hypertrophy as defined in this study was present on the baseline ECG in 793 (8.3%) study participants. Of these, voltage criteria alone were present in 441 (55.6%) patients, voltage criteria and LV strain in 189 (23.8%) and voltage criteria with LV strain and left axis deviation in 75 (9.5%). The remaining 88 patients had voltage criteria for LVH and left axis deviation without a LV strain pattern.
Baseline characteristics of HOPE study patients with electrocardiographic LVH
Key baseline characteristics of patients with and without ECG-LVH at baseline are shown in Table 1. Patients with LVH were older and more likely to be Hispanic or black, although overall the prevalence of non-Caucasian study participants was low in both groups. A history of prior stroke, TIA, PAD and hypertension was more common in patients with ECG-LVH, while current smoking was more common in those without. The prevalence of CAD, prior MI, diabetes and hypercholesterolaemia was similar in patients with and without ECG-LVH. Patients with ECG-LVH were more likely to be treated with diuretics and calcium channel blockers. There were no significant differences in the use of beta-blockers, nitrates, cholesterol-lowering agents, insulin, oral hypoglycaemic agents, oral anticoagulants, post-menopausal hormone replacement or antiplatelet agents. Baseline physical examination revealed higher systolic and diastolic blood pressure in the patients with ECG-LVH. Patients without ECG-LVH had higher body mass index and higher waist and hip circumference. Patients with ECG-LVH had lower serum potassium levels at baseline, while serum creatinine was similar in those with and without ECG-LVH.
Major cardiovascular events and total mortality of HOPE study participants with and without ECG-LVH
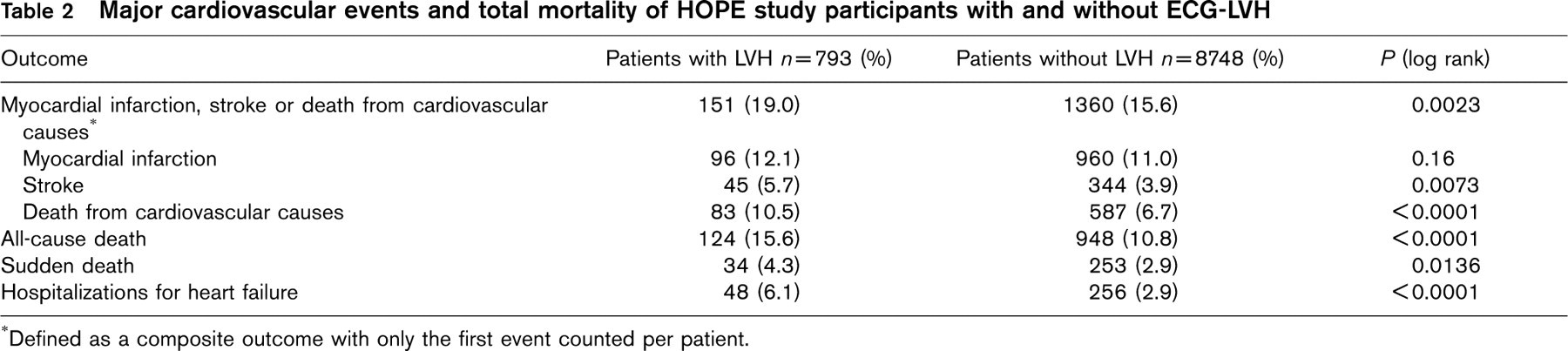
Defined as a composite outcome with only the first event counted per patient.
The effect of electrocardiographic LVH on the risk for major cardiovascular events and death
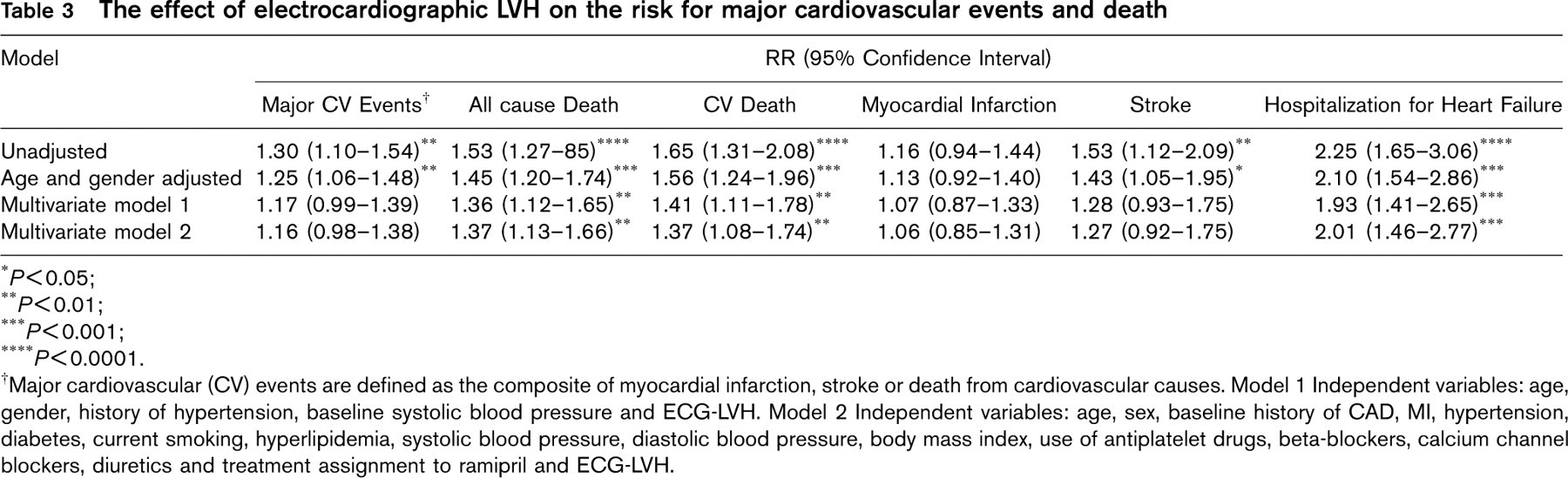
P<0.05;
P<0.01;
P<0.001.
P<0.0001.
Major cardiovascular (CV) events are defined as the composite of myocardial infarction, stroke or death from cardiovascular causes. Model 1 Independent variables: age, gender, history of hypertension, baseline systolic blood pressure and ECG-LVH. Model 2 Independent variables: age, sex, baseline history of CAD, MI, hypertension, diabetes, current smoking, hyperlipidemia, systolic blood pressure, diastolic blood pressure, body mass index, use of antiplatelet drugs, beta-blockers, calcium channel blockers, diuretics and treatment assignment to ramipril and ECG-LVH.
Electrocardiographic LVH and the risk of major cardiovascular events
Patients with ECG-LVH had higher cumulative rates of primary HOPE outcome events, of all-cause death and of hospitalizations for heart failure (Figure 1A, B and C).
Among the 793 patients with baseline ECG-LVH, 151 (19.0%) sustained a major CV event - MI, stroke or death from CV causes - compared with 1360 patients among the 8748 (15.6%) without ECG-LVH (P = 0.0023) (Table 2). The RR of sustaining a major CV event was 1.30 (95% CI, 1.10-1.54; P < 0.01) for patients with baseline ECG-LVH vs. those without. This association remained statistically significant after adjustment for age and gender. In multivariate analyses, after correcting for baseline imbalances and other predictors of CV risk, a similar trend was noted, although this did not reach conventional levels of statistical significance in multivariate models. Similarly, the risk of stroke was increased in the presence of ECG-LVH in unadjusted analysis and in analysis adjusted for age and gender with non-significant trends in multivariate analyses. The association with risk of MI was not statistically significant (Table 3).
Electrocardiographic LVH and the risk of death
Among 793 patients with ECG-LVH, 124 (15.6%) died compared with 948 (10.8%) of those without ECG-LVH (P < 0.0001) (Table 2). The RR of all-cause death for patients with ECG-LVH was 1.53 (95% CI, 1.27-1.85; P<0.0001) and this association remained statistically significant in multivariate models controlling for age and gender and for other predictors of risk (Table 3). Independent predictors of all-cause death in multivariate analysis (model 2) were current smoking (RR, 2.06; 95% CI, 1.77-2.41), history of MI (RR, 1.63; 95% CI, 1.40-1.89), diabetes (RR, 1.42; 95% CI, 1.24-1.62), ECG-LVH (RR, 1.37, 95% CI, 1.13-1.66), history of hypertension (RR, 1.20; 95% CI, 1.05-1.38), treatment assignment to ramipril (RR, 0.84; 95% CI, 0.74-0.95), male sex (RR, 1.21; 95% CI, 1.04-1.40) age (RR, 1.07; 95% CI, 1.06-1.08) and systolic blood pressure (RR, 1.00; 95% CI, 1.00-1.01). Similarly, the risk of death from CV causes was also significantly higher in patients with baseline ECG-LVH (Table 3). Independent predictors of CV death in the multivariate model 2 were current smoking (RR, 1.91, 95% CI, 1.56-2.34), history of MI (RR, 1.68, 95% CI, 1.39-2.02), history of CAD (RR 1.61, 95% CI, 1.18-2.18), diabetes (RR, 1.67, 95% CI, 1.36-1.90), male sex (RR, 1.47; 95% CI, 1.08-1.74), ECG-LVH (RR, 1.37; 95% CI, 1.08-1.74), treatment assignment to ramipril (RR, 0.75; 95% CI, 0.64-0.87), history of hypertension (RR, 1.26; 95% CI, 1.06-1.49) and age (RR, 1.07; 95% CI, 1.05-1.08). There were overall few reports of sudden death, but these were more frequent in individuals with ECG-LVH (Table 2).
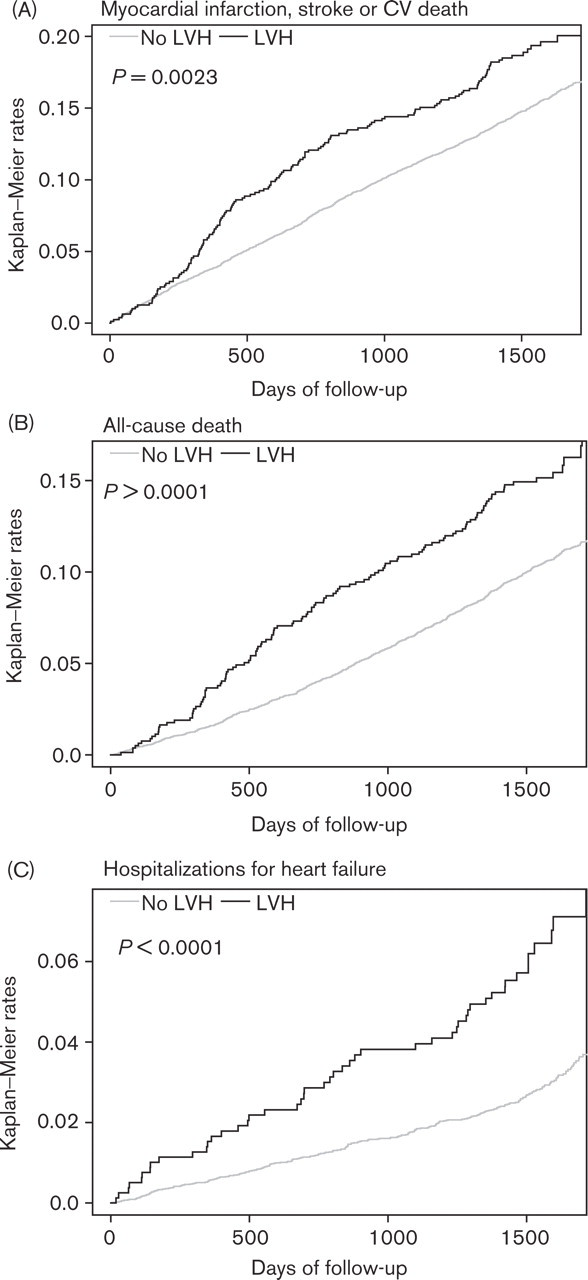
Kaplan-Meier estimates of the composite of myocardial infarction, stroke or death from cardiovascular causes (A), of all-cause death (B) and of hospitalizations for heart failure (C) in patients with and without ECG-LVH.
Electrocardiographic LVH and the risk of heart failure
Among the 793 patients with ECG-LVH, 48 (6.1%) required hospital admission for heart failure vs. 256 (2.9%) of the 8748 patients without ECG-LVH (P < 0.0001) (Table 2). The RR for heart failure requiring hospital admission for patients with ECG-LVH vs. those without was 2.25 (95% CI, 1.65-3.06; P < 0.0001) and this association remained highly statistically significant after adjusting for age and gender and in multivariate models (Table 3). Independent predictors of heart failure risk in the multivariate model 2 were diabetes (RR, 2.29; 95% CI, 1.79-2.92), history of MI (RR, 2.07; 95% CI, 1.54-2.78), ECG-LVH (RR, 2.01; 95% CI, 1.46-2.77), current smoking (RR, 1.9; 95% CI, 1.39-2.59), age (RR, 1.08; 95% CI, 1.07-1.10) and body mass index (RR, 1.04; 95% CI, 1.01-1.07).
Subgroup analyses
In subgroup analyses the adjusted risk for all-cause death, CVdeath and heart failure associated with ECG-LVH was significant and not significantly different in clinically relevant subsets of patients including women, men, patients younger and older than 65 years and in those with and without a history of CVD, CAD, hypertension and diabetes.
The presence of ECG-LVH with LV strain and of ECG-LVH with LV strain and with left axis deviation identified subsets of patients at particularly high risk for adverse outcomes. Patients with voltage criteria for LVH and LV strain had a multivariate (model 2) adjusted RR for the composite outcome of MI, stroke or death from CV causes of 1.65 (95% CI, 1.25-2.17; P = 0.0004), for all-cause death of 1.55 (95% CI, 1.12-2.16; P = 0.008), for CV death of 1.68 (95% CI, 1.51-2.45; P = 0.007), for stroke of 1.74 (95% CI, 1.05-2.89; P=0.032) and for hospitalizations for heart failure of 3.43 (95% CI, 2.20-5.37; P<0.0001). Patients with voltage criteria for LVH, LV strain and left axis deviation had a multivariate RR for the composite outcome of MI, stroke or death from CV causes of 1.72 (95% CI, 1.10-2.68; P=0.016), for all-cause death of 2.96 (95% CI, 1.95-4.48; P<0.0001), for CV death of 2.69 (95% CI, 1.60-4.51; P=0.0002), for stroke of 2.21 (95% CI, 1.04-4.70; P=0.039) and for hospitalizations for heart failure of 2.75 (95% CI, 1.22-6.20; P=0.014). In the multivariate analysis ECG-LVH with LV strain, with or without left axis deviation, was by far the most potent clinical predictor of risk for heart failure.
Discussion
The main finding of our study is that LVH defined by very simple ECG criteria is an independent predictor of increased risk of all-cause death, CV death and heart failure in a wide range of patients with vascular disease. Using this very simple definition of LVH the risk of major vascular events and of stroke was also increased and the association remained significant after controlling for age and gender, but not after further adjusting for other predictors of risk. The patients enrolled in the study had generally well controlled blood pressure and a significant proportion were taking anti-ischaemic, blood pressure lowering and other cardiac protective drugs. In the presence of ECG-LVH the increased incidence of adverse outcomes was noted after a short duration of observation (Figure 1). The effect of ECG-LVH was similar (no statistically significant differences) in patients with a history of CAD and in those without and in other clinically relevant subsets of patients, including men, women, those with a history of hypertension and those without, those with diabetes and those without. LVH with repolarization abnormalities consistent with LV strain and LVH with LV strain and with left axis deviation were associated with higher risk than LVH by voltage criteria alone.
The association with risk of heart failure is particularly noteworthy, with a multivariate two-fold increase in the risk of developing heart failure in this population with well preserved LV ejection fraction at study entry and with a very rapid effect of LVH on heart failure risk. We believe that the ascertainment of heart failure events was precise. Only heart failure events considered to be the direct cause for hospital admission are included in this report. These events were all predefined secondary outcomes of the HOPE trial and were adjudicated based on review of hospital charts in the presence of documented clinical and radiological signs of congestion. We did not perform serial measurements of LV ejection fraction in all study patients and diastolic function was not measured, so that we cannot reliably differentiate between heart failure due to systolic versus diastolic dysfunction. However, patients with previous episodes of heart failure and those with known low LV ejection fraction were excluded from study participation and in an echocardiographic study conducted in 506 study participants baseline LV ejection fraction was 58% and study end ejection fraction remained on average well preserved, 57% (diastolic function was not measured in the echocardiographic substudy) [33]. Furthermore, the adverse effect of ECG-LVH on heart failure became apparent after a short period of observation and was observed in patients who did, as well as those who did not sustain an MI during the study. Therefore, diastolic dysfunction was likely a major mechanism of heart failure in this middle-aged population with vascular disease and multiple CV risk factors.
Various mechanisms may explain the association between LVH and increased CV risk. Thus, LVH may be a more sensitive marker of exposure to hypertension than casual blood pressure measurements. Other factors leading to LVH, including age, presence and extent of CAD, increase in cardiac collagen content, obesity, salt intake, neurohormonal factors and genetically determined influences are also strongly associated with increased CV risk. LVH itself can cause increased oxygen demand and reduced coronary vasodilator reserve, subendocardial ischaemia, lethal arrhythmias, diminished ventricular performance and increased stiffness of the myocardium leading to diastolic heart failure [2].
Relevance of the study in the context of previous investigations evaluating the prognostic relevance of left ventricular hypertrophy
Several previous studies have evaluated the prognostic relevance of ECG-LVH. Seminal data are provided by the Framingham Heart study, which enrolled in its original cohort 2336 men and 2873 women between the ages of 30 and 62 and conducted biennial follow-up evaluations. After 14 years of follow-up study participants with ECG-LVH had a 3.3-fold age-adjusted increased risk of death and a 2.7-fold increase in the risk of myocardial infarction [6]. After 20 years of follow-up the age-adjusted risk of death, stroke, MI and cardiac failure was increased in men and in women with ECG-LVH, 5 and 4.7 times, 4.1 and 7.6 times, 2 and 3 times and 7.5 and 8.6 times, respectively [9]. The excess risk for all these outcomes persisted in multivariate analysis taking other risk factors, including hypertension into account. These findings relate to LVH with ST-T abnormalities (LV strain) in addition to high R wave amplitude (voltage criteria), defined by the Framingham investigators as ‘definite LVH’. By comparison, when adjusted for hypertension, the risk associated with isolated high R wave-LVH (defined as ‘possible LVH’) was virtually nil [9]. Compared with the Framingham study, ECG-LVH was a less powerful predictor of death and CV morbidity in our study, although the populations studied differ greatly. A number of other large population-based epidemiological studies and studies in hypertensive cohorts have assessed the risk associated with ECG-LVH and reinforce in general the findings of the Framingham Heart study [13–25]. The prevalence of ECG-LVH and the estimates of risk associated with ECG-LVH vary however, quite considerably in these studies and the variability of these estimates is related to the different populations studied and the differences in the diagnostic criteria used to define ECG-LVH and to define the clinical endpoints of interest, as recently reviewed in a comprehensive overview by Ashley et al. [34]. Furthermore, in most of these studies the number of individuals with ECG-LVH and the number of outcome events were relatively small, accounting for difficulties in obtaining precise estimates of risk, in spite of the large number of subjects studied and the prolonged periods of follow-up of many such studies, some of which extended over decades. For example, in the Framingham Heart study at the time of initial evaluation only 76 individuals were found to have ‘definite’ ECG-LVH and another 57 had ‘possible LVH’ and after 14 years of follow-up ‘definite LVH’ was present in 233 subjects [6]. After 14 years of follow-up there were 531 deaths, the total number of persons with pre-existent or newly manifested CAD was 574 and there were 123 cases of congestive heart failure [6]. In our study both the number of individuals with ECG-LVH and the number of outcome events are significantly higher.
Very few studies to date have explored the prognostic significance of ECG-LVH in individuals with clinically overt CAD or other manifestations of CVD. In the Framingham Heart study the appearance of ECG-LVH increased the risk of death three-fold for those with antecedent angina pectoris, and four-fold for those with previous MI [10]. These data are derived however, from a small number of subjects with established CAD [6]. Furthermore, the use of effective preventive therapies such as aspirin, lipid-lowering agents, beta-blockers and ACE inhibitors in patients with CAD was much lower in the Framingham cohort than it is at present, so that the relevance of the reported risk estimates for ECG-LVH to current clinical practice is limited. The Coronary Drug Project, a randomized trial of lipid lowering drugs, reported the outcome of 2760 men in the placebo arm of the study, followed from 1969-1972. Three-year mortality of the 186 (6.7%) men with prior MI who had ECG-LVH was almost twice that in men without ECG-LVH (22.6% vs. 12.1%; P=0.0002) [26]. After controlling for other variables, ECG-LVH by voltage criteria alone was not an independent predictor of mortality, while the presence of ECG-LVH with ST depression and T wave inversion (LV strain) predicted increased mortality even when other risk predictors were considered. The number of subjects with ECG-LVH and the number of all-cause deaths for the entire study population, 354, are much smaller than in our study. Furthermore, the study may be of limited applicability at present, as patients' management differed greatly from current clinical practice standards. Sullivan et al. evaluated 4824 patients referred for coronary angiography [27]. Angiographically significant CAD was found in 3063 patients, of whom 182 met ECG criteria for LVH. Five-year survival was significantly lower in patients with ECG-LVH as compared with those without, regardless of whether CAD was present: 84.4% vs. 94.5% (P=0.016) in the absence of CAD and 81.0% vs. 87.7% in the presence of CAD (P<0.001).
A few previous studies have evaluated the risk associated with echocardiographic LVH in CAD patients. Ghali et al. evaluated a cohort of 785 patients, mostly black hypertensives, referred for coronary angiography [35]. Left ventricular hypertrophy was identified by echocardiography in 194 of 381 patients with angiographically proven CAD. After 4 years of follow-up the RR of death adjusted for age, gender and hypertension was 2.14 (95% CI, 1.24-3.68) in patients with LVH compared with those without. In a subsequent report the same group of investigators reported data on 1089 black patients who underwent coronary angiography and were followed for 5 years [36]. Eighty percent of patients had a history of hypertension. Left ventricular hypertrophy was identified by M-mode echocardiography in 50% of the study participants and was a significant independent predictor of all-cause death and cardiac death both in patients with and in those without coronary artery disease. The risk of death was increased about two-fold in CAD patients with echocardiographic LVH. These studies clearly identify LVH as a significant predictor of risk in CAD patients. The results, however, apply primarily to hypertensive black CAD patients. Furthermore, these studies did not evaluate the risk of developing heart failure or other adverse CVoutcomes. The method used to identify LVH, M-mode echocardiography, while more sensitive than electrocardiography, is more costly and not used routinely in risk stratification, especially in patients with CAD without prior MI or heart failure.
Study limitations
A possible limitation of our study relates to the absence of central ECG readings. However, the ECG tracings were evaluated by site investigators following predefined criteria for the diagnosis of LVH. The criteria used for defining ECG-LVH are very simple and more complex criteria have been shown to have better correlations with echocardiographic LVH [34]. However, such complex criteria and scoring systems are not frequently used in clinical practice and would be also difficult to apply in large multicentre studies. The simplicity of the diagnostic criteria for LVH and the fact that ECGs were interpreted by individual investigators may increase the clinical applicability of our study. A high proportion of patients (52.8%) had prior MI, which may impact on the detection of LVH on baseline ECG. However, multivariate analyses adjusted for history of prior MI are reported. Echocardiography is more sensitive in detecting increased left ventricular mass and echocardiographic LVH has been shown to increase the risk of death [37]. Echocardiography is, however, more costly and remains less frequently employed than ECG. Finally, the majority of our patients were Caucasian and it is unclear if the study results apply to other racial groups such as African Americans.
Conclusions
In conclusion, our study provides strong evidence for the importance of ECG-LVH as a potent predictor of CV risk in a broad range of patients with CVD. Clinicians should aggressively pursue the use of preventive therapies in all CV patients with ECG-LVH. In the HOPE trial only 45.8% of patients with ECG-LVH had a mean blood pressure (averaged for multiple measurements obtained over the duration of the study) of <140/90 mmHg and the rate of use of lipid lowering drugs was 26.9% at baseline (data obtained in 1993-1995), although this rate increased to 45.2% at study end (1999), consistent with an impact of clinical trials and changing clinical practice guidelines. These data suggest that in many such high-risk vascular disease patients with ECG-LVH control of risk factors may be suboptimal. This is by far the largest study evaluating ECG-LVH in a high-risk population with established vascular disease. The large number of patients and of outcome events allowed us to provide estimates of risk associated with ECG-LVH for specific outcomes and to explore the effect of ECG-LVH in different subgroups. ECG-LVH was a particularly powerful predictor of death and heart failure. The data provided by our study on the risk of heart failure associated with ECG-LVH are unique in this population of patients with vascular disease. Further evaluation of diastolic versus systolic dysfunction in the causation of heart failure in vascular disease patients with ECG-LVH is warranted and may better define prevention and management strategies. The risk prediction for stroke associated with ECG-LVH was also significant in unadjusted analyses and after adjustment for age and gender. However, in multivariate analyses ECG-LVH was not an independent predictor of risk for stroke and the relationship of ECG-LVH with MI was relatively weak. The presence of LV strain in addition to voltage criteria for LVH increased the associated risk of death and of heart failure and the risk of stroke associated with ECG-LVH with LV strain remained statistically significant in multivariate analyses.
The very simple ECG criteria used to define LVH make our findings easily applicable. We believe, therefore, that this simple tool should be consistently used in identifying a subset of individuals at particularly high risk for CV morbidity and mortality, who should be targeted for aggressive risk reduction.