
Abstract
Purpose
The aim of this study was to evaluate the predictive factors of return to work after coronary bypass graft surgery, for the subgroup of professionally active patients aged less than 60 years included in the PERISCOP study.
Methods
In the principal, prospective, multicentre study, 2065 patients were evaluated 20 ± 10 days after surgery by exercise testing, echocardiogram and 24-h ambulatory ECG monitoring. A questionnaire was completed one year after surgery. We studied a subgroup of this population, consisting of 530 patients previously defined (94.5% men; mean age: 50.5 ± 5.8 years).
Results
One year after surgery, five of these patients had died and 21 were lost to follow-up. Among the remaining patients, 340 patients (67.5%) had returned to work. Forty patients (7.9%) had retired, 45 (8.9%) were on sick leave, 22 (4.4%) were unemployed, 49 (9.7%) returned to work after the deadline of 12 months, eight (1.6%) had given insufficient information on return to work. In multivariate analysis, the independent predictors of a failure to return to work were age > 51 years [OR: 0.39 (95% CI: 0.25-0.59)], being a manual worker [OR: 0.49 (95% CI: 0.31-0.79)], being from South East France [(OR: 0.42 (95% CI: 0.23-0.74)], presence of angina [OR: 0.40 (95% CI: 0.20-0.82)], dyspnoea [(OR: 0.46 (95% CI: 0.28-0.77)] and a duration of exercise < 420s [(OR: 0.50 (95% CI: 0.33-0.76)].
Conclusions
Return to work after coronary bypass graft surgery is observed in 67.5% of cases and depends essentially on socio-professional factors and residual symptoms. A regional effect was also observed, which requires further study.
Introduction
The restoration of normal functional capacity and quality of life, in which the resumption of professional activity is an important element, is a major objective of coronary artery surgery. The predictive factors for a return to work after myocardial infarction are well known, but few studies have focused specifically on the resumption of employment after coronary bypass graft surgery (CABG) [1–6]. Since the first coronary bypass interventions were performed in 1968 [7], there has been a considerable evolution in the indications for such surgery and the techniques used. Angioplasty, with or without stenting, is increasingly used in place of CABG. The possibility of associating the two methods makes it possible to achieve the goal of complete revascularization in most cases [8, 9]. The use of arterial grafts since the 1980s has improved long-term functional and vital prognosis [10] without affecting the frequency of return to work [11].
PERISCOP [12, 13] is a national, prospective, multicentre study including 2065 patients with coronary disease referred for cardiac rehabilitation between May 1998 and February 1999, following CABG. The main objective of PERISCOP was to assess the predictive value of non-invasive cardiac evaluation for mortality and cardiovascular events, and the therapeutic management of lipid abnormalities. One of its secondary objectives was to investigate the resumption of professional activity after treatment.
The aim of the present study was to evaluate the factors predicting a return to work one year after CABG in the subgroup of patients who were working before surgery. Only patients below the legal retirement age of 60 years were included in this study.
Methods
PERISCOP is a prospective multicentre cohort study with classification of judgment criteria by an event validation committee.
Inclusion criteria
Patients were considered eligible for inclusion if they were born and living in France (in order to facilitate the follow-up), were likely to remain in France for at least a year, were aged over 18 years and agreed to participate in the study and follow-up. Return to work was analysed only for patients aged less than 60 years who were employed before surgery.
Exclusion criteria
We did not include patients with pacemakers, patients who had undergone associated surgery (correction of valve disease, resection of an aneurysm, vascular surgery) and patients with a history of cardiac surgery other than coronary artery surgery.
Determination of the size of the cohort
The number of subjects required for the PERISCOP study [12, 13] was determined on the basis of the principal judgment criterion: mortality and cardiovascular events. It was estimated to be 2000 patients.
Cardiac evaluation
The evaluation [13] was routinely carried out 20 ± 10 days after surgery, and consisted of a symptom-limited exercise test, an echocardiography with evaluation of ventricular function (wall motion index) and 24-h ambulatory ECG monitoring (AECG).
Working status
The evaluation criterion was return to work rate one year after CABG, as evaluated by a self-completed questionnaire sent to the patients. If no response was received, a complementary interview was carried out by phone.
Statistical analysis
The rates of unemployment and the number of physicians for a given number of inhabitants were determined from a census of the French population carried out in 1999 and data for the National Council of the Order of Physicians from the same year, for the 15-60 year age group of the active population. Quantitative values are expressed as mean ± standard deviation. Qualitative values were compared using the χ2 test, and quantitative values were compared using Student's t-test. The multivariate logistic regression models were generated for the variables correlated with the resumption of employment in the univariate analysis. Values of P < 0.05 were considered statistically significant. The statistical analysis was carried out with NCSS 2000 software (NCSS Statistical Software, Kaysville, UT, USA).
Results
Characteristics of the population
Of the 2065 patients included in the PERISCOP study, 690 were less than 60 years old and 160 of these patients were without employment at the time of inclusion (Figure 1). In total, we studied the resumption of employment of 530 patients. The clinical characteristics of the patients at the time of inclusion are described in Table 1. The study population had a mean age of 50.5 ± 5.8 years and consisted mostly of men. Slightly more than one third of the patients had a history of myocardial infarction. They had a mean of 2.5 coronary artery lesions. Myocardial revascularization was complete in 77.7% of cases (411 patients).
The results of non-invasive cardiac evaluation are described in Table 2. All the patients underwent exercise testing and 528 patients underwent echocardiography. Wall motion index was determined for 517 patients. The study population was arbitrarily divided into five regional groups according to the dialing code of the telephone number of the rehabilitation centre that included the patient. The patients were distributed as follows: 107 patients (20.2%) in Ile de France (region 1), 146 patients (27.5%) in the North West (region 2), 66 patients (12.5%) in the North East (region 3), 77 patients (14.5%) in the South East (region 4) and 134 patients (25.3%) in the South West (region 5). The unemployment rates for members of the active population aged 15 to 59 years, according to the 1999 French census, were 11.6% for region 1, 11.8% for region 2, 13.47% for region 3, 14.37% for region 4 and 12.92% for region 5. The density of physicians in 1999, for all specialties, was 8.71 per thousand inhabitants aged 15-59 years for region 1, 6.22 for region 2, 6.62 for region 3, 8.25 for region 4 and 7.77 for region 5.
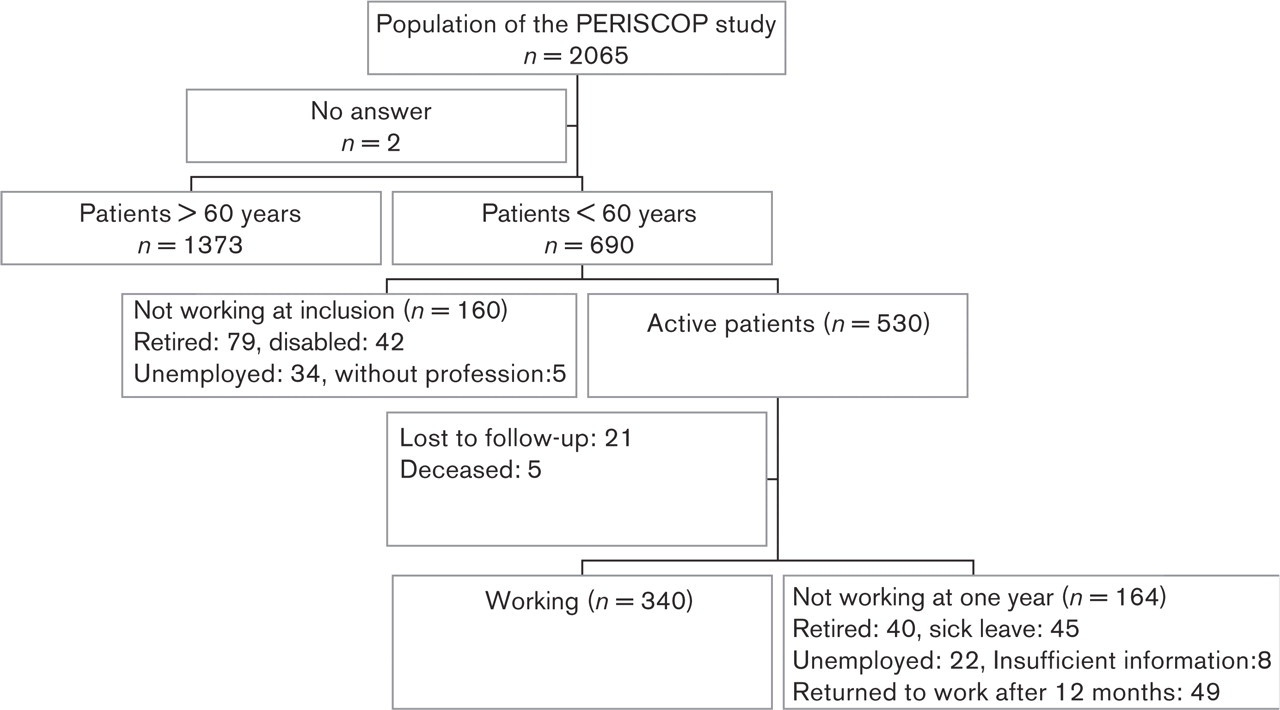
Flow chart of the study.
Baseline characteristics of the population (n = 530)
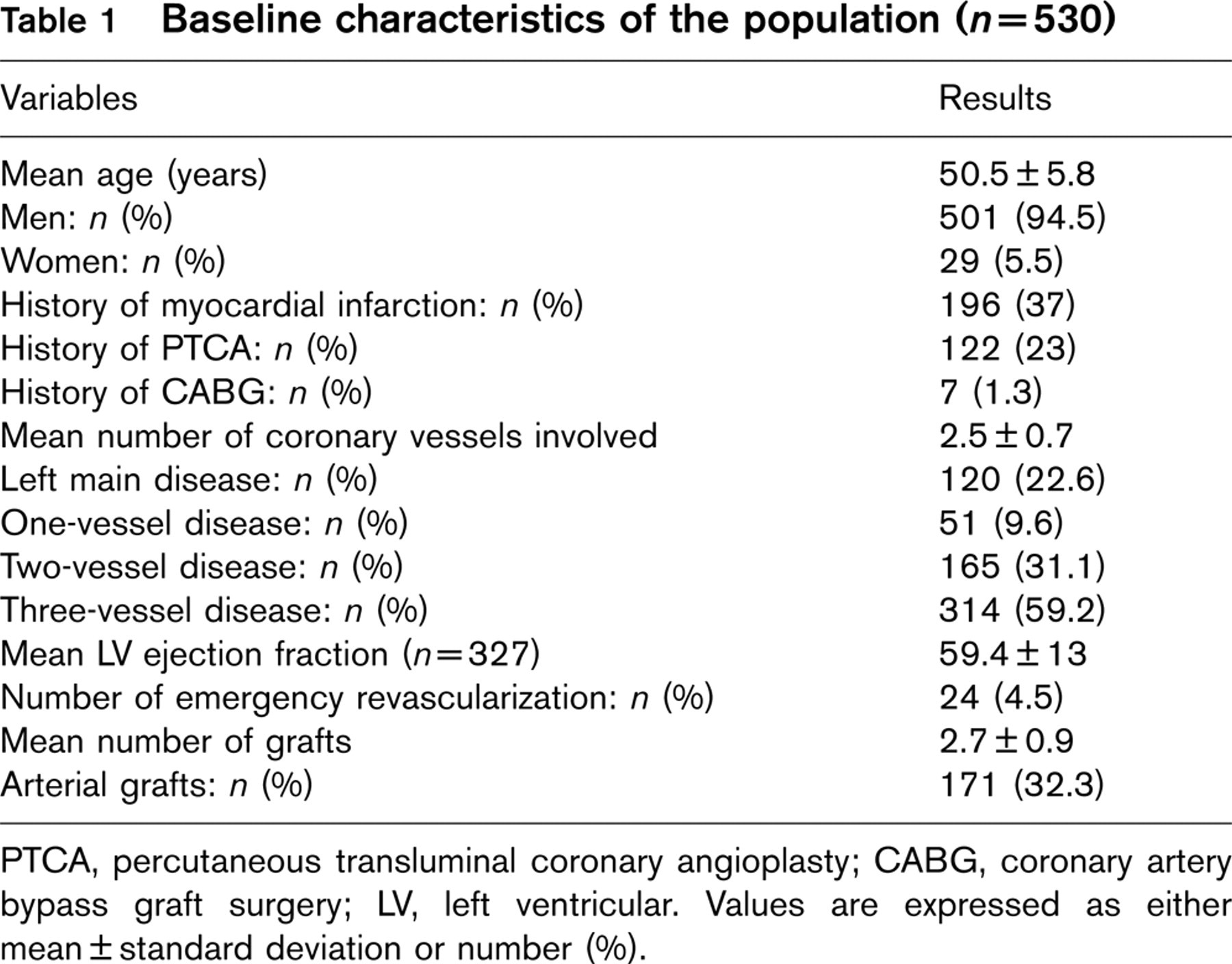
PTCA, percutaneous transluminal coronary angioplasty; CABG, coronary artery bypass graft surgery; LV, left ventricular. Values are expressed as either mean ± standard deviation or number (%).
Results of non-invasive cardiac evaluation (n = 530)
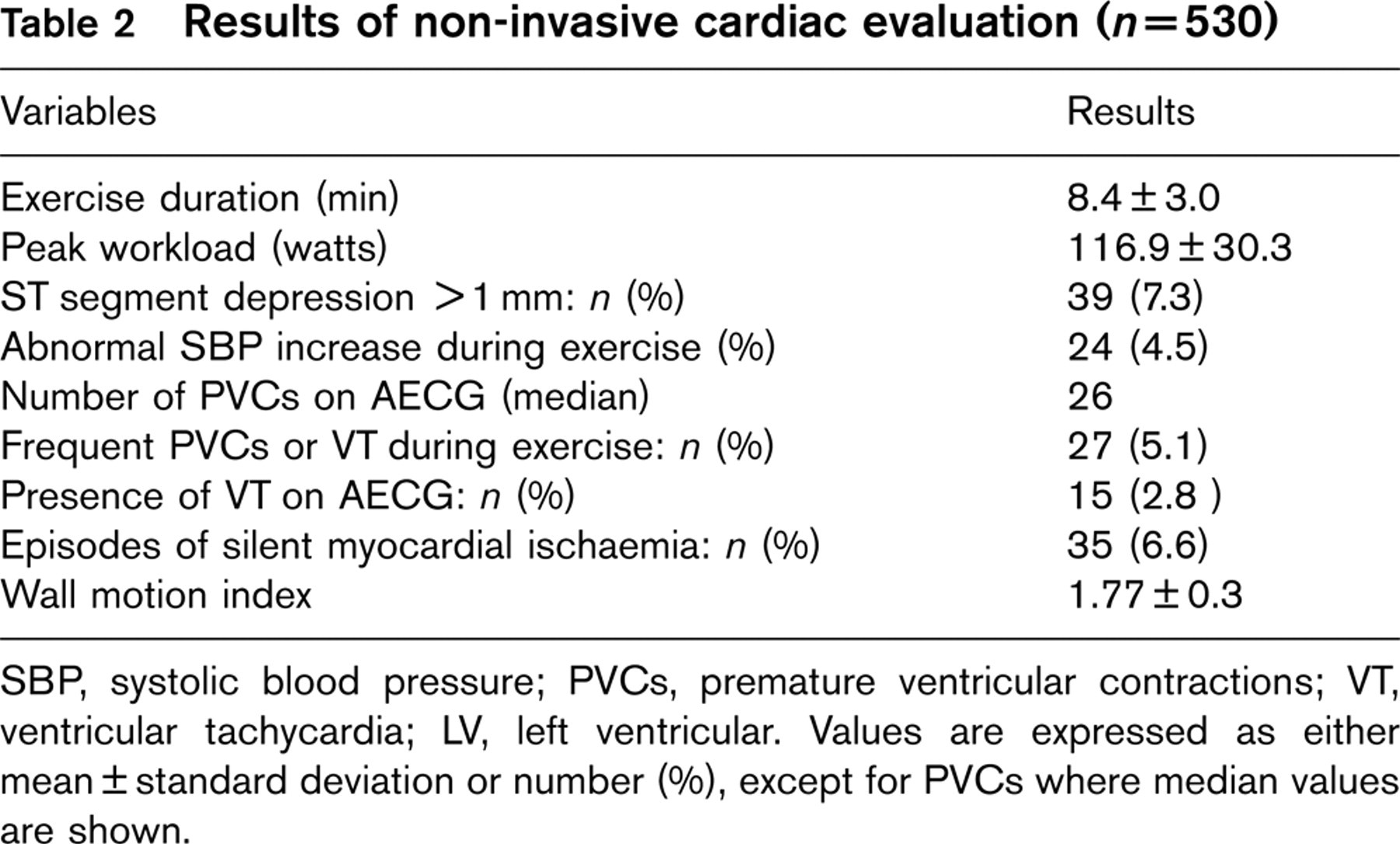
SBP, systolic blood pressure; PVCs, premature ventricular contractions; VT, ventricular tachycardia; LV, left ventricular. Values are expressed as either mean ± standard deviation or number (%), except for PVCs where median values are shown.
The patients were assigned to one of the six socio-professional categories derived from the INSEE French national classification of occupation [14]:
Category 1: Farmers and agricultural workers: 15 (2.5%)
Category 2: Craftsmen, tradesmen and entrepreneurs: 81 (15.4%)
Category 3: Executives and intellectual professions: 102 (19.4%)
Category 4: Intermediate professions: 100 (18.9%)
Category 5: Employees: 105 (19.9%)
Category 6: Manual workers: 126 (25.9%)
The distribution of socio-professional categories in each region is shown in Figure 2.
Follow-up and return to work
The follow-up period covered one year after surgery. Five of the 530 patients died during this period and 21 were lost to follow-up. Return to work was therefore analysed for 504 patients. Among these patients, 340 (67.5%) returned to work before the twelfth month, 40 (7.9%) took retirement, 45 (8.9%) were placed on sick leave and 22 (4.4%) were unemployed. Forty-nine patients (9.7%) returned to work after the deadline of 12 months, and therefore were considered as not resuming work in the analysis. Eight patients (1.6%) had not given sufficient information on return to work at one year. The mean time between surgery and return to work was 3.2 ± 2.2 months and 50% of the patients had returned to work before the third month. The cumulative proportion of patients returning to work is shown n Figure 3.
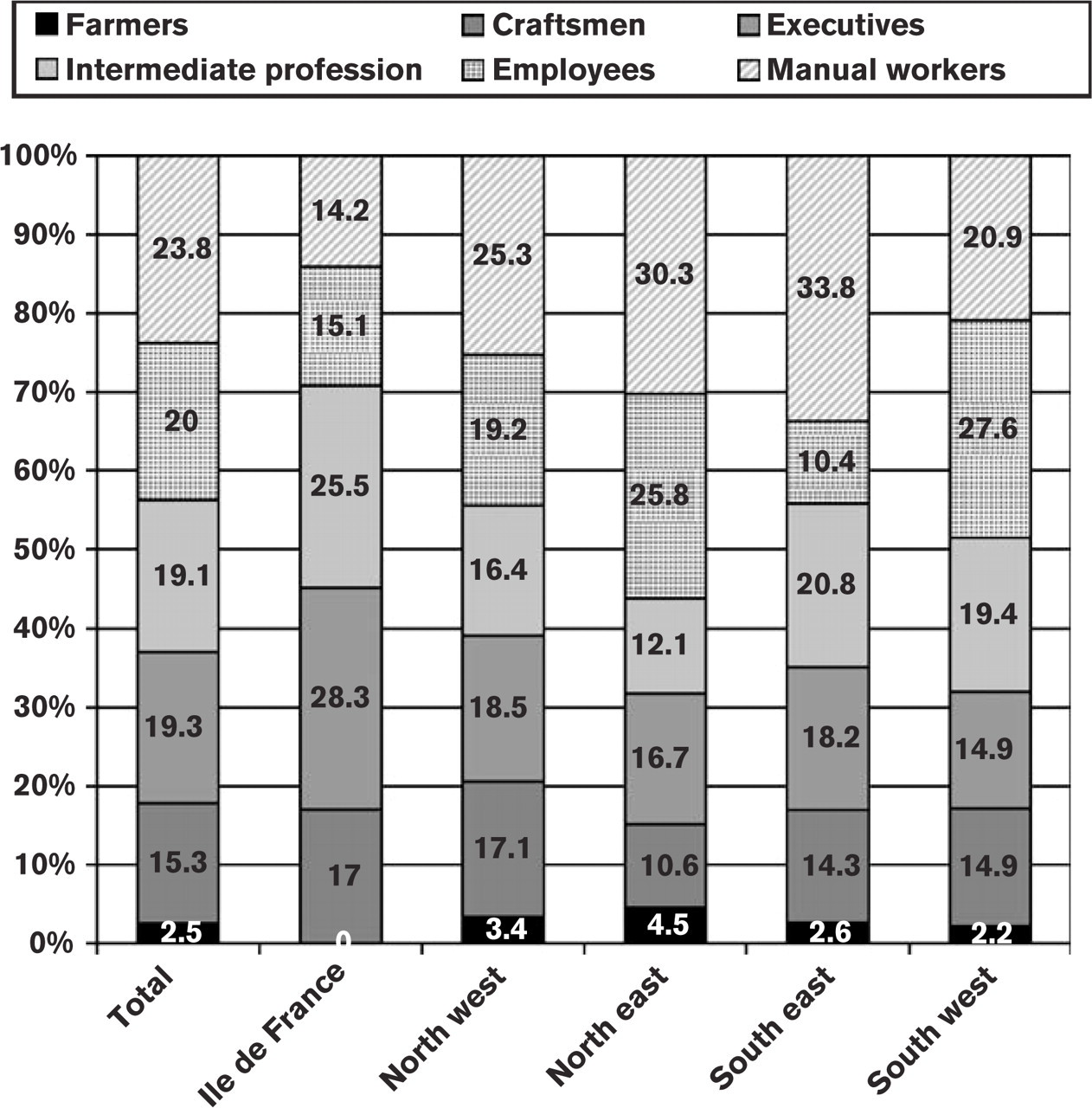
Distribution of socio-professional categories by region. Number in the columns represent percentage of each socio-professional category in the region.
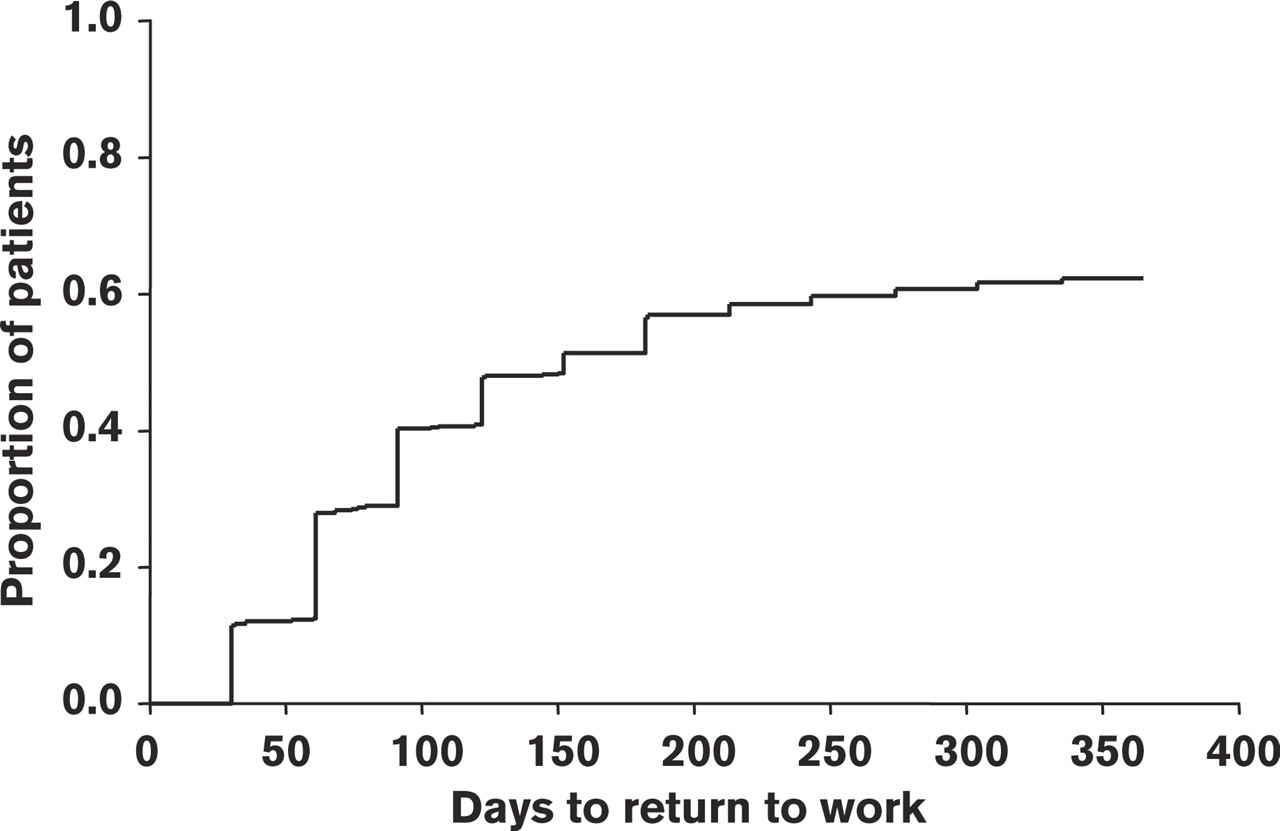
Cumulative Kaplan-Meyer curve showing the cumulative proportion of patients returning to work during the one-year follow-up.
The factors significantly associated with return to work in univariate analysis are listed in Tables 3 and 4. The patients who did not return to work tended to be older, manual workers. They had lower exercise capacity and frequently had residual symptoms. We observed also differences between the regions: the frequency of return to work was significantly lower for patients from the South East than for patients from other regions. The presence of an arterial graft was more frequent in patients resuming their work than in the case of no work resumption. In contrast, complete revascularization was not associated with the frequency of return to work.
Interestingly, patients who did not return to work have been included in centres located in ‘departments’ (French administrative region) where the unemployment rate is slightly higher than in ‘departments’ of patients resuming work (12.73 ± 2.53% vs. 12.21 ± 2.01%; P = 0.013). At the opposite, the density of physicians in the inclusion region had no significant effect on return to work rate (7.87 ± 2.78 vs. 7.64 ± 2.06 per thousand inhabitants, P = 0.34).
For multivariate logistic regression analysis of all the variables associated with the resumption of employment, we transformed the variable ‘age’ into a two-class variable with the median (51 years) used as the cut-off point. We performed a similar transformation for the duration of exercise test (median: 420 s). After logistic regression analysis (Table 5), the following variables were found to be significant independent predictors of a lower probability of return to work: older age, low socio-professional category, inclusion in the South East of France, presence of angina or dyspnoea and a poor performance during the exercise test.
Discussion
The frequency of return to work (67.5%) was similar to that previously observed after cardiac rehabilitation following CABG. Monpère [15] studied return to work in 57 consecutive patients below the age of 60 years, all of whom were active and referred during the first 22 days following surgery; 73.2% patients resumed their employment within 109.9 ± 84 days. The rates of return to work obtained in our study were similar to those in other published studies: 56% at 12 months in the study by Engblom [16], 72% at one year in the BARI study [17], 77% at 2 years in the study by Smith [4], and 77% at 2 years for Pocock [18], following CABG or angioplasty.
Advanced age was strongly, negatively correlated with return to work in the PERISCOP study. Similar results have repeatedly been reported in previous studies in the BARI study [17] and others [3, 4, 18–22]. Hlatky [19], reported frequencies of return to work of 79% for the under 55 years age group, 74% for the 55 to 59 year age group, 58% for the 60 to 64 year age group and 65% for the over 65 years age group. Pocock [18] observed a major decrease in the rate of return to work at 2 years in the over 55 years age group.
Influence of socio professional variables on return to work (n = 504)
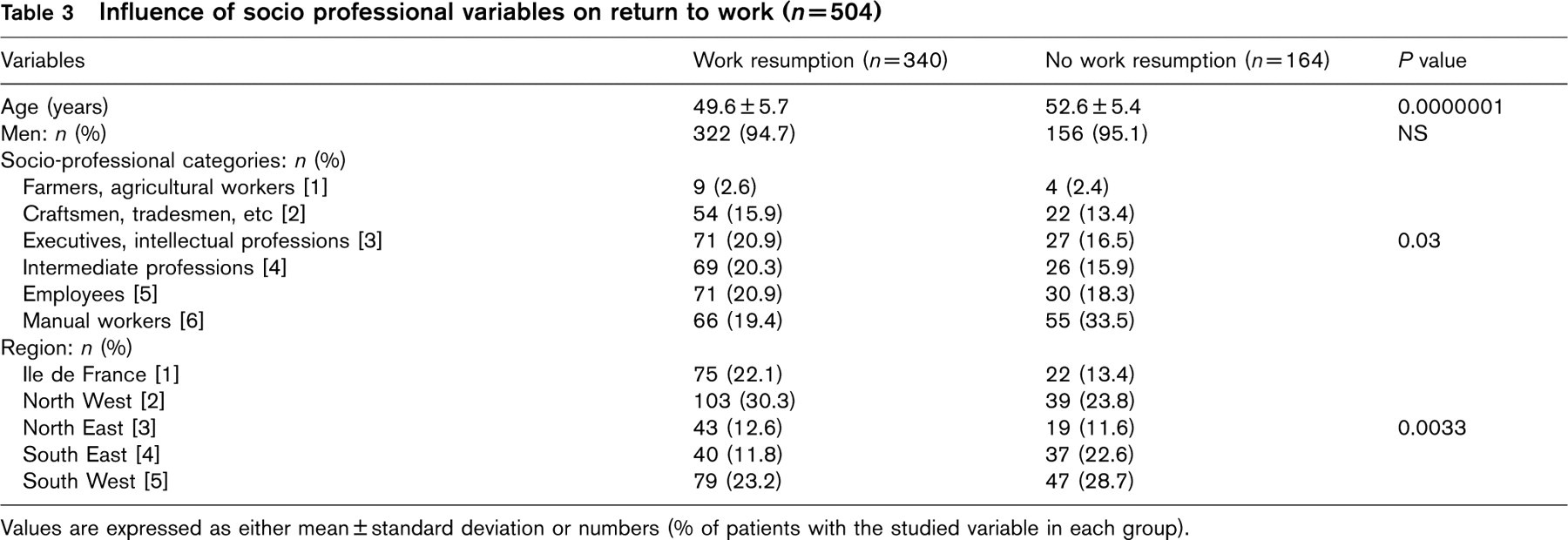
Values are expressed as either mean ± standard deviation or numbers (% of patients with the studied variable in each group).
Influence of medical variables on return to work (n=504)
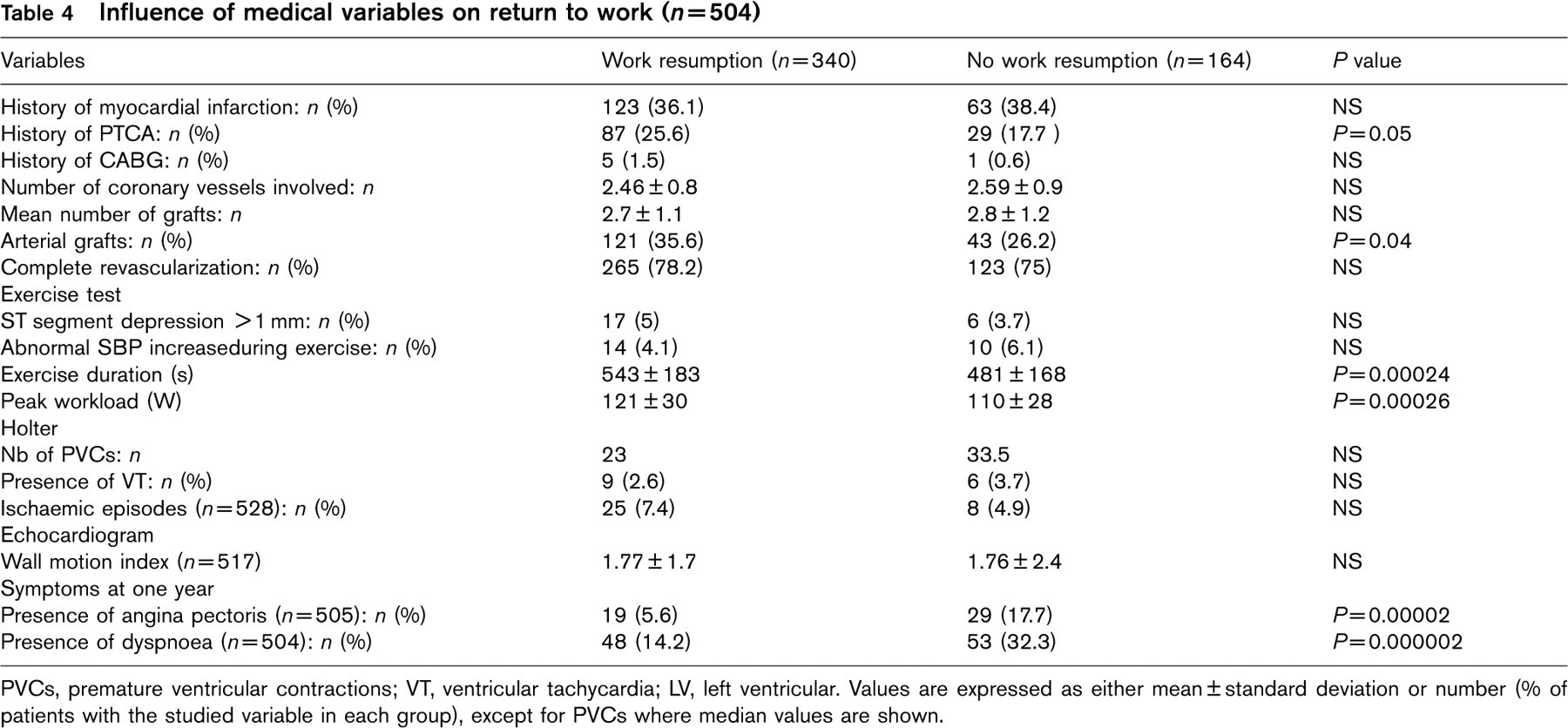
PVCs, premature ventricular contractions; VT, ventricular tachycardia; LV, left ventricular. Values are expressed as either mean ± standard deviation or number (% of patients with the studied variable in each group), except for PVCs where median values are shown.
Independent predictors related to return to work (logistic regression)
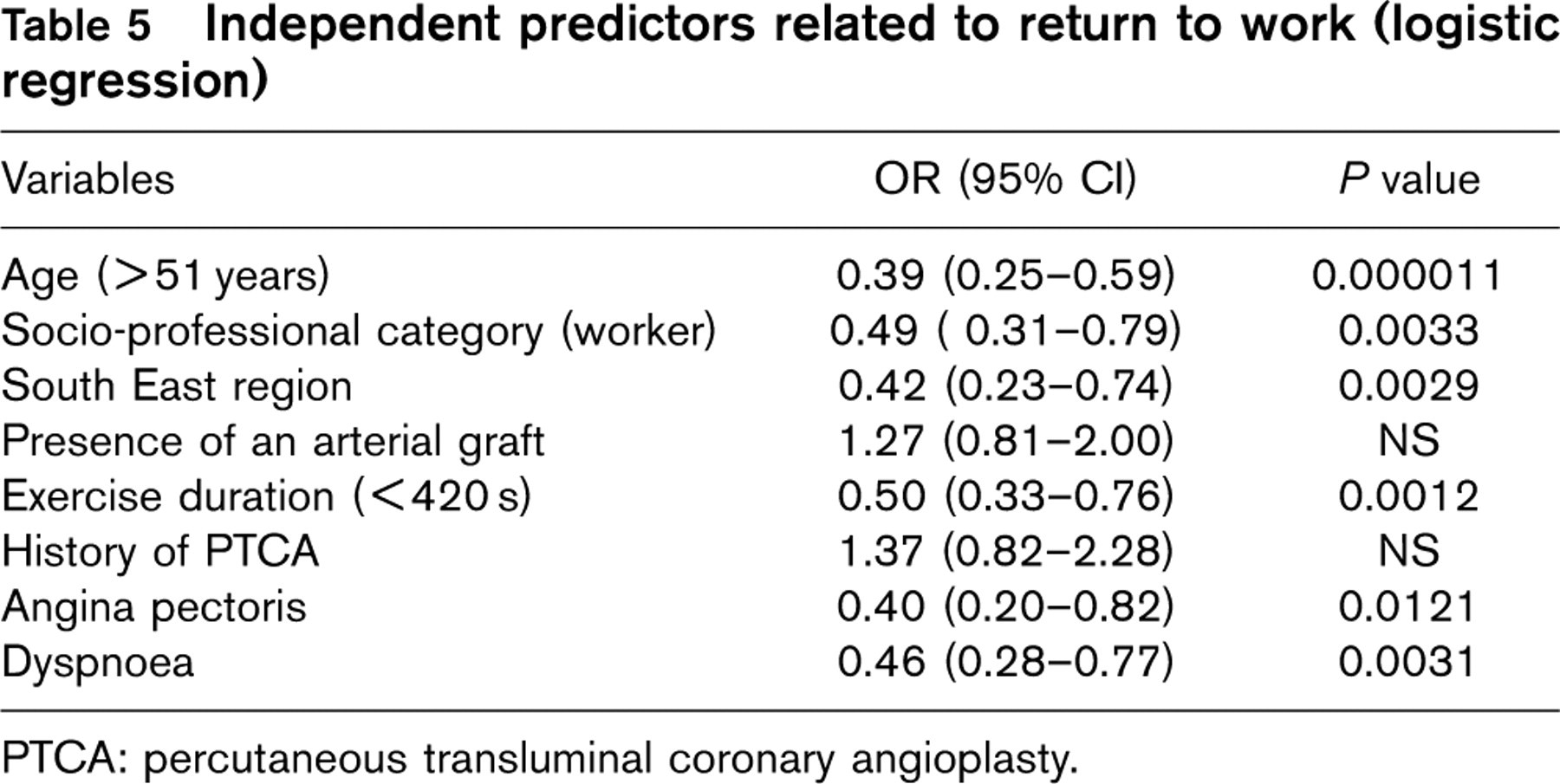
PTCA: percutaneous transluminal coronary angioplasty.
In the PERISCOP study, the socio-professional category ‘manual worker’ was independently associated with a lower rate of return to work. Similar results have regularly been reported in other studies [15, 19, 20]. Monpère [15] observed a positive correlation between the rate of return to work and social category, with frequencies of return to work of 60% for manual workers, 65% for craftsmen, 70% for employees and 100% for executives. Speziale [20] reported a frequency of return to work of 79% for executives, versus only 52.6% for manual workers and craftsmen (OR = 0.65; 95% CI: 0.15-0.95). According to Hlatky [19], manual workers are less likely to go back to work than employees and executives, 1 year or 3 years after surgery (76% after 1 year and 63% after 3 years for employees and executives, versus 66% and 54%, respectively, for manual workers; P= 0.04). However, this difference disappeared in multivariate analysis, in which the only independent factors identified were employment status before surgery, level of education and social protection status.
In PERISCOP, the frequency of return to work was lowest in South East France. The influence of the region of origin has been little studied. Speziale [20] observed a lower frequency of return to work (40.7%) in patients from southern Italy than in patients from central Italy (57.1%). In PERISCOP, this regional difference was not a consequence of a higher rate of employment or the overrepresentation of a particular social category (manual worker) in this region (Figure 2). The obligatory medical insurance and retirement regime in France provides highly uniform protection. Other factors not analysed in PERISCOP may account for this result. Such factors include particular social or professional characteristics, different levels of income and differences in quality of life specific to the sample from this region.
Our study, like others, showed that the persistence of angina is frequently associated with a low rate of return to work [3, 4, 18, 20, 21]. According to Pocock [18], the risk of being without employment for cardiac reasons 2 years after surgery is three times higher in patients with angina. For Anderson [3], in patients under the age of 55 years, angina is the most important reason for not returning to work. Skinner [21] found angina to be an independent risk factor for a low rate of return to work, both at 1 year and at 5 years after surgery; the frequency of angina was 59% among patients who had returned to work and 78% among those who had not (OR =2.41; 95% CI: 1.414.40) after 1 year and 68% and 91%, respectively, after 5 years (OR = 4.9; 95% CI: 2.51-9.87). However, Hlatky [19], Hammermeister [22] and Mark [23] all reported no effect of angina on the frequency of return to work.
Cardiac failure or left ventricular dysfunction, in the absence of symptoms or presence of weak symptoms, has diverse effects on the frequency of return to work. According to Speziale [20] and Laird-Meeter [24], neither left ventricular dysfunction nor cardiac insufficiency is negatively correlated with a lack of return to work. According to Smith [4], cardiac insufficiency is associated with a lack of return to work, but has a much weaker effect than angina. In contrast, Mark [23] found that this factor had a major negative effect on the likelihood of returning to work (OR = 0.20; 95% CI: 0.100.39). Maor [25] found that patients with a left ventricular ejection fraction below 40% were less likely to return to work than other patients (OR = 1.71; 95% CI: 1.24-2.36).
Some studies have evaluated the effect of functional capacity, as determined by exercise electrocardiogram, on the rate of return to work after CABG. Engblom [16] obtained results similar to those obtained here. The exercise level was significantly higher in the group that returned to work (161 ± 36 W vs. 123 ± 41W).
The results of our study were consistent with those of previous studies in that the number of coronary branches affected [20, 21–24], the nature of the graft—saphenous, arterial or mixed—[23] and the achievement of complete revascularization [4] were all found to have no predictive value for return to work.
Limits of the study
The percentage of women in this substudy population is low (5%). This is the consequence of the rarity of CAD in women: 14% in the main study [12, 13]. This figure is further diminished by the inclusion of working people < 60 years in this substudy, which favours inclusion of men, because CAD is more frequent in men before 60 years of age. So the results of this study are not easily applicable to women.
The use of a self-reporting questionnaire may be criticized, as possibly leading to questionable reliability of data. We did not test the reliability of the questionnaire on this point. However, the risk for the patient to report better results than the real outcome for pleasing his/her physician is unlikely: the questionnaire was sent by mail by the rehabilitation centre. The use of a self-reported questionnaire is a widely used mean of assessing the return to work rate in such population, already used in other well-known studies already mentioned in the discussion [22–24]. Errors made by patients completing this type of questionnaire probably occurred in both directions: this kind of error decreases the precision of OR, but does not modify the direction of the relationship.
This study was not designed to evaluate the effects of cardiac rehabilitation on return to work. So, no conclusion in this field may be drawn.
Conclusions
Despite improvements in surgical techniques, the rate of return to work after CABG is observed in two-thirds of cases and has not changed in the last 20 years.
Advanced age and belonging to the socio-professional class ‘manual worker’ were consistently associated with a low rate of return to work. The surgical technique used (use of arterial grafts), the quality of revascularization and the consequences of myocardial ischaemia (ventricular arrhythmias or dysfunction) were all found to have no effect on the likelihood of returning to work. However, a high level of workload reached during exercise testing on the 20th day was found to be an independent factor predictive of a higher likelihood of returning to work.
Despite the existence of similar medical management and social protection levels throughout France, we found that ‘region’ had an effect on the frequency of return to work that was independent of socio-professional category and medical variables. Other factors not taken into account in this study, such as quality of life, level of income (for the principal salary) and specific personal retirement plans may account for this finding.