
Abstract
Background
Primary hyperparathyroidism (PHPT) is associated with hypertension, coronary atherosclerosis and other cardiovascular diseases. We aimed to evaluate serum parathyroid hormone (PTH) levels as an independent risk factor for coronary heart disease (CHD) in subjects with serum calcium within the reference range.
Design
Population-based cross-sectional study.
Methods
The Tromsø Study was attended by 27159 subjects aged 25-79 years. Serum PTH was measured in 3570 subjects. They all completed a questionnaire on medical history, including questions on angina pectoris and myocardial infarction along with a food-frequency questionnaire. A total of 1459 men and 1753 women with serum calcium 2.20-2.60 mmol/l, serum creatinine< 121 μmol/l and who did not use diuretics were included in the present study. Linear regression was used to reveal associations between PTH, age, body mass index, serum calcium, calcium intake, cholesterol, blood pressure, glycosylated haemoglobin (HbA1c) and smoking status. A logistic regression model was used to find the independent predictors of CHD.
Results
When stratified for age the rate of CHD was higher in the subjects with serum PTH > 6.8 pmol/l than in those with normal or low serum PTH levels [relative risk 1.67, 95% confidence interval (CI) 1.26-2.23 in men and 1.78, 95% CI 1.22-2.57 in women]. The highest PTH quartile (> 3.50 pmol/l in men and > 3.30 pmol/l in women) predicted CHD, with odds ratios of 1.70 (95% CI 1.08-2.70) for men and 1.73 (95% CI 1.04-2.88) for women, versus the lowest PTH quartile (< 1.90 pmol/l for men and < 1.80 pmol/l for women).
Conclusions
Serum PTH predicts CHD in subjects with calcium levels within the reference range. This may indicate a role for PTH in the development of CHD.
Introduction
Increased levels of parathyroid hormone (PTH) may have harmful effects on the heart. Patients with primary hyperparathyroidism (PHPT) have been reported to have an increased arterial stiffness [1], altered arterial reactivity [2], left ventricular hypertrophy [3], and a high prevalence of mitral and aortic valve calcifications [4]. Similar associations between PTH and cardiovascular diseases have been reported in patients with secondary hyperparathyroidism due to renal failure [5]. Jorde et al. [6] reported a positive association between blood pressure and PTH in patients with secondary hyperpar-athyroidism and a low calcium intake. In addition to these clinical studies there are in-vitro and animal studies indicating a role for PTH by itself in the cardiovascular system. Thus, chronic exposure to an increased PTH level led to abnormal energy metabolism and reduced cardiac output [7] as well as hypertrophy of cultured cardiomyocytes from adult rats [8]. Recently, receptors for PTH and PTH-related peptide (PTHrp) have been found in the heart [9]. So far there are only a few reports on PTH levels in patients with coronary heart disease (CHD); the results are conflicting [10, 11], and none, to our knowledge, are based on epidemiological studies.
In 1994-1995 a general health survey with emphasis on cardiovascular disease was performed in Tromsø. Measurements of serum PTH were taken in a subgroup, thus enabling us to evaluate the relation between CHD and PTH. To exclude confounding effects of primary and also secondary hyperparathyroidism only those with serum calcium within the reference range and without renal failure were included. Furthermore, as diuretics have been reported to induce elevated PTH levels [12], subjects using diuretic drugs were excluded.
Methods
Study population
In 1994-1995, all men and women older than 24 years, living in the municipality of Tromsø, were invited to participate in a health survey. This was the fourth Tromsø Study and it was conducted in accordance with the previous ones [13]. A randomly selected subset of subjects aged 25 to 79 years was invited for further studies including serum PTH measurement. Only subjects with serum calcium and creatinine within the reference ranges, and non-users of diuretics were included in the final analysis.
Measurements
A questionnaire including medical history was completed by the participants at home and returned by mail. Concerning CHD they were asked: ‘Do you have or have you ever had myocardial infarction?’ and ‘Do you have or have you ever had angina pectoris?’ with the possible answers ‘Yes’ or ‘No’. Those answering ‘Yes’ to one or both questions were considered to have CHD. The subjects were also asked about medication, including the use of diuretics. All participants completed a food-frequency questionnaire, and intakes of calcium and vitamin D were measured as previously described [14]. All participants were asked: ‘Do you smoke?’ with the possible answers ‘Yes’ or ‘No’.
Height and weight were measured while subjects wore light clothing and no shoes. Body mass index (BMI) was calculated as kg/m2. Blood pressure was measured with an automatic device (Dinamap Vital Signs Monitor 1846; Criticon Inc, Tampa, FL, USA) [14]. Blood samples were drawn for measurement of serum cholesterol, creatinine, total serum calcium and analysed as previously described [13]. Serum PTH was measured by an Immulite intact PTH assay (Diagnostic Products Corp.) [6]. Determination of glycosylated haemoglobin (HbA1c) in EDTA whole blood was based on an immunoturbido-metric assay with reagents (UNIMATES) from F. Hoffmann-La Roche AG (Basel, Switzerland). The HbA1c percent value was calculated from the HbA1c/Hb ratio. The inter-assay coefficient of variation (CV) was 4.5%. The reference ranges for cholesterol in our laboratory are 3.2-7.4 mmol/l for those aged 25 to 29 years, 3.7-8.3 mmol/l for those aged 30 to 39 years and 4.1-8.7 mmol/l for those older than 40 years; serum creatinine 55-100 μmol/l for women and 70-120 μmol/l for men; total serum calcium 2.20-2.60 mmol/l, HbA1c 4.0-6.5%, serum PTH 1.1-6.8 pmol/l for those 50 years old or younger and 1.1-7.5 pmol/l for those older than 50 years. The subjects were not requested to fast.
Statistical methods
Statistical analyses were carried out using the SPSS for WINDOWS (version 10.0; SPSS Inc., Chicago, Illinois, USA). and Epi Info 6 (version 6.04b) packages. Males and females were analysed separately. All covariates were tested for normal distribution by visual inspection of the distribution curve and by skewness. Differences between means were analysed with ANOVA. A sex-specific multiple linear regression model with serum PTH as dependent variable was applied to examine linear relations with age, BMI, serum calcium, cholesterol, systolic blood pressure, calcium intake and HbA1c.
Logistic regression was used to test the following potential predictors of CHD for independence: age, BMI, serum cholesterol, serum calcium, systolic blood pressure, calcium intake and HbA1c. All covariates were entered as continuous variables, as logistic regression does not assume any particular type of distribution [15]. Serum PTH was divided into quartiles (< 1.90; 1.90-2.60; 2.61-3.50; > 3.50 pmol/l for men and < 1.80; 1.80-2.40; 2.41-3.30; > 3.30 pmol/l for women) and entered into the multiple logistic regression model as a categorical variable with the first group as a reference category to study the odds ratio and association between PTH quartiles (adjusted for other covariates) and self-reported history of CHD.
We used the analysis of frequency tables with stratifying by age to calculate relative risks. Unless otherwise stated, the values are mean ± SD.
All tests are two-sided, and P < 0.05 was considered statistically significant.
Ethics
All subjects gave written consent to participate and the study was approved by the regional ethics committee.
Results
The total number of subjects examined in the Tromsø study 1994-1995 was 27 159. PTH was measured in a subgroup of 3570 subjects, 1605 men and 1965 women. Of these, 88 men and 90 women had a total serum calcium level below 2.20 mmol/l, and 15 men and 44 women had serum calcium above 2.60 mmol/l. Among the remaining 3333 subjects 15 men and 17 women had serum creatinine above 120 μmol/l and 100 μmol/l, respectively. Finally, among the rest of the 3301 subjects, 28 men and 61 women used a diuretic, thus leaving 3212 subjects, 1459 men and 1753 women to be included in the final analysis.
A total of 155 men and 122 women aged 40-79 years reported past or present angina pectoris without the occurrence of infarction, and 131 men and 46 women aged 40-79 years reported previous coronary infarction. Among those who reported infarction, 61 men and 31 women also had angina, thus 286 men and 168 women were considered to have a history of CHD. The remaining 1173 men and 1585 women were without a history of CHD.
All variables, including the dependent variable serum PTH, turned out to be normally distributed both in males and females (skewness < |1.5|). The demographics are shown in Tables 1 and 2. Calcium intake was higher in participants without a history of CHD (470.4 ± 254.9 versus 428.8 ± 221.5 mg/d, P < 0.05 in men and 441.2 ± 241.6 versus 409.2 ± 242.4mg/d, NS in women), while vitamin D intake did not differ significantly between these two groups (7.4 ± 5.1 versus 7.2 ± 5.0 μg/d in men and 7.0 ± 5.3 versus 8.4 ± 5.7 μg/d in women). Vitamin D intake was not included in further analyses. In both sexes there were fewer smokers among those with CHD (25 versus 34%, P < 0.05 in men and 26 versus 32%, NS in women). However, when correcting for the other covariates (age, BMI, serum cholesterol, serum calcium and PTH) smoking status was not a significant predictor of CHD.
In the multiple regression models, for both sexes, age, BMI and systolic blood pressure had a significant positive relation to serum PTH (P < 0.01), while serum calcium and dietary calcium intake had a significant negative relation to PTH (P < 0.05). Neither HbA1c nor smoking status had relation to serum PTH, and were therefore not included in the multivariate model.
In the logistic regression model BMI, serum cholesterol and systolic blood pressure were significant and independent explanatory variables for CHD only in men, whereas age predicted CHD in both sexes (Table 3). The highest PTH quartile (> 3.50 pmol/l in men and > 3.30 pmol/l in women) emerged as an independent significant predictor of CHD in both genders (Figs 1 and 2). It resulted in odds ratios of 1.70 [95% confidence interval (CI) 1.08-2.70] for men and 1.73 (95% CI 1.04-2.88) for women, versus the lowest PTH quartile (< 1.90pmol/l for men and < 1.80pmol/l for women).
Characteristics of the study population
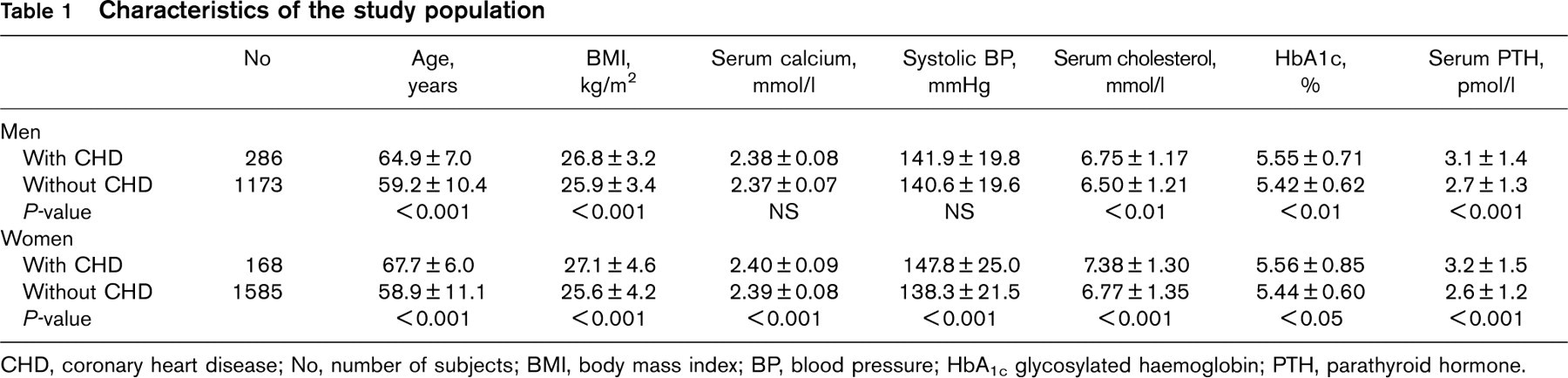
CHD, coronary heart disease; No, number of subjects; BMI, body mass index; BP, blood pressure; HbA1c glycosylated haemoglobin; PTH, parathyroid hormone.
Baseline covariates with respect to PTH quartiles
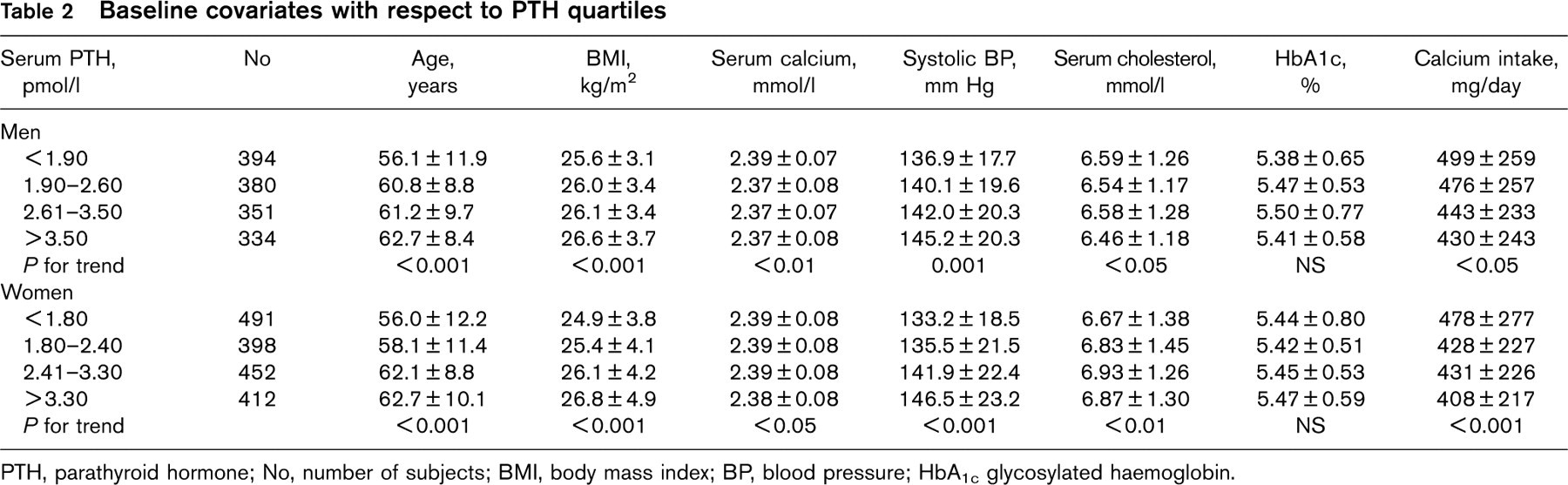
PTH, parathyroid hormone; No, number of subjects; BMI, body mass index; BP, blood pressure; HbA1c glycosylated haemoglobin.
Moreover, the CHD rates, stratified for age, were higher in those with serum PTH level above than in those with serum PTH within the reference range (relative risk 1.67, 95% CI 1.26-2.23 in men and 1.78, 95% CI 1.22-2.57 in women, P < 0.001 and < 0.005, respectively).
Discussion
In the present study we have, as expected [16], found age, serum cholesterol and BMI to be significant predictors of CHD in men. In addition, we found serum PTH to be an independent predictor of CHD in both sexes, which to our knowledge has not been reported before from an epidemiological study.
Previous studies on the relation between PTH and CHD have yielded conflicting results. Thus, in a study by Ljunghall et al. [17] serum PTH levels were elevated in a group of 26 patients admitted for coronary infarction, whereas in a larger study from the same authors this could not be confirmed [10]. Similarly, Herrmann et al. [11] found PTH to be elevated in 26 out of 56 patients with CHD verified by coronary angiography, whereas Watson et al. [18] found no correlation between PTH and coronary calcification quantified by electron beam computed tomography. However, these studies are not directly comparable to ours, as we did not study PTH during the acute phase of the infarction, and our study was not a case-control study, but based on a population survey.
Independent risk factors for CHD
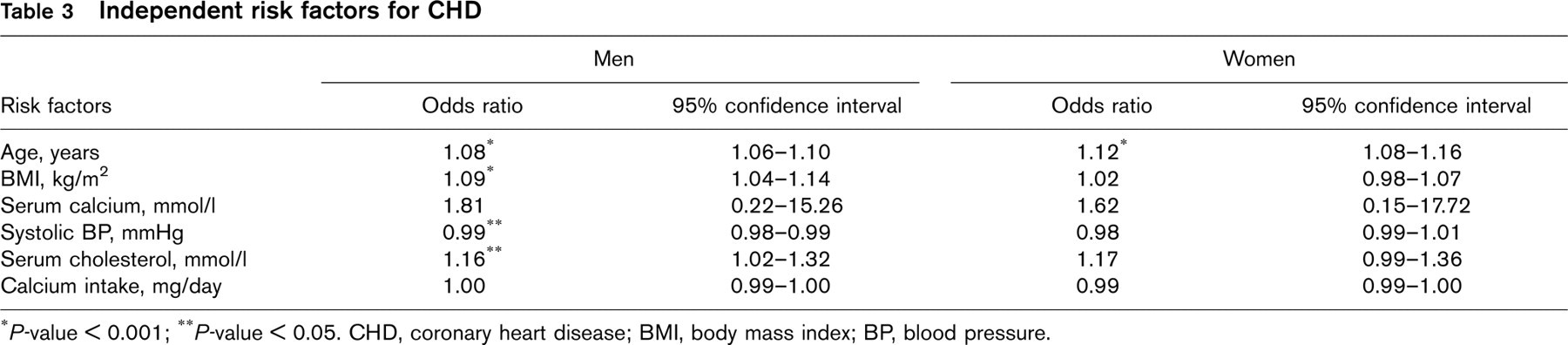
∗P-value < 0.001;
∗∗P-value < 0.05. CHD, coronary heart disease; BMI, body mass index; BP, blood pressure.
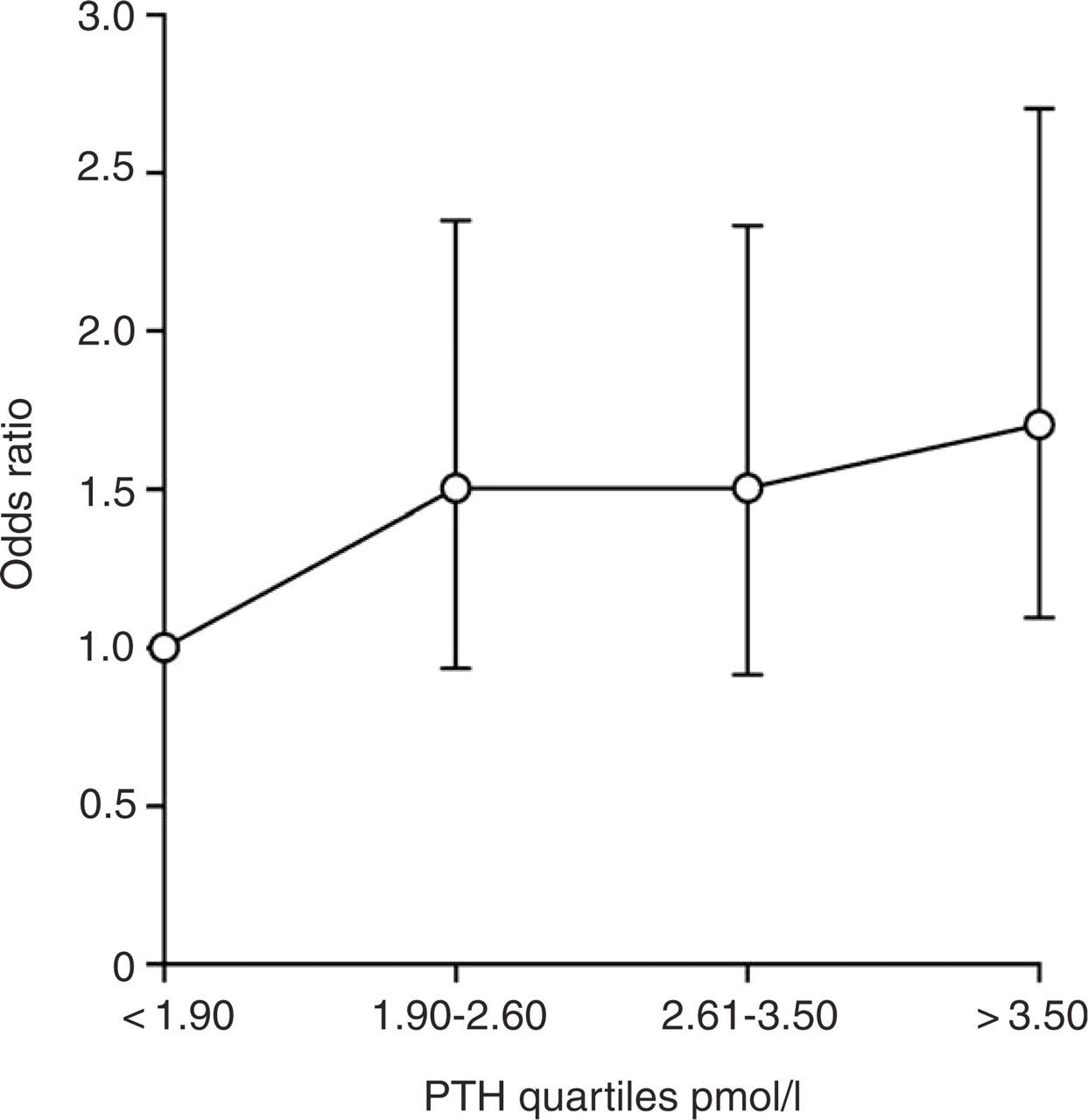
Parathyroid hormone (PTH) quartiles as independent predictors of coronary heart disease (CHD) in men, based on multiple logistic regression. Odds ratio is represented with 95% confidence interval with the first quartile as a reference category. Only the fourth quartile predicts CHD significantly (P<0.05).
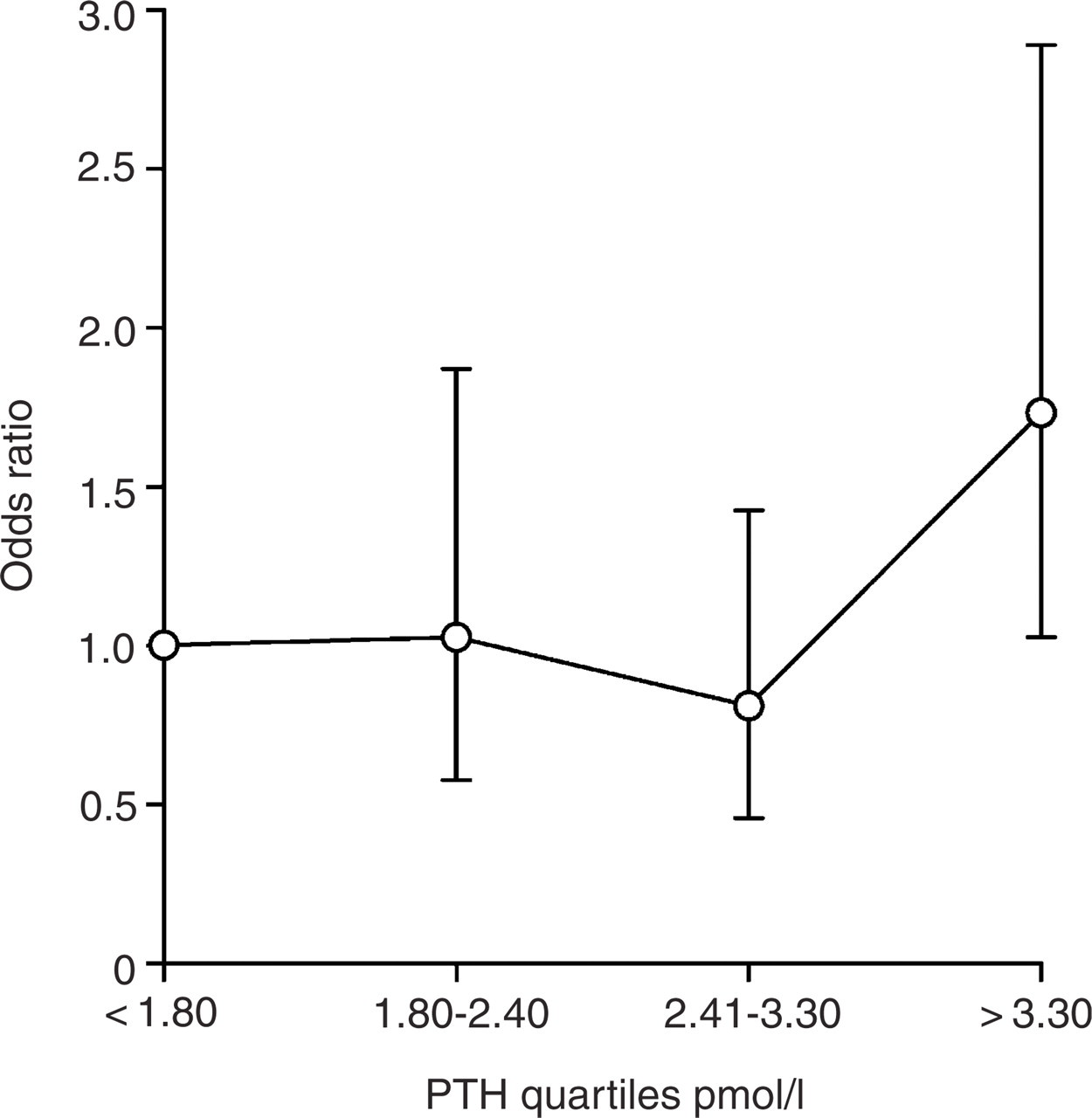
Parathyroid hormone (PTH) quartiles as independent predictors of coronary heart disease (CHD) in women, based on multiple logistic regression. Odds ratio is represented with 95% confidence interval with the first quartile as a reference category. Only the fourth quartile predicts CHD significantly (P < 0.05).
The present study included more than 3000 subjects, and a number of confounding factors was controlled for. Thus, subjects with primary hyperparathyroidism and subjects with secondary hyperparathyroidism due to renal failure are known to be at risk for development of heart disease [19–21]. To avoid influence by these disease states, subjects with reduced renal function and subjects with serum calcium outside the reference range were excluded from the study. Furthermore, inadequate calcium intake is associated with increased blood pressure [14] and could therefore, at least indirectly, contribute to CHD. In our study calcium intake was higher in those without a history of CHD, and when including calcium intake along with serum calcium in the linear regression, both had a negative relation to PTH. Accordingly, the association between PTH and CHD cannot be explained by covariation with calcium. Serum PTH is known to increase with age, BMI, blood pressure [22] and possibly also HbA1c values [23]. These variables were therefore also included in the analyses. Finally, as it has recently been reported that the use of diuretics may increase the serum PTH level by approximately 25% [12], the users of diuretics were excluded from the final analysis.
We found no effect of vitamin D intake on CHD, but we did not measure the actual vitamin D levels. A low vitamin D level is associated with an elevated serum PTH and in this light our finding of high PTH levels in those with CHD may therefore be an epiphenomenon. Thus, Scragg et al. [24] reported an inverse relationship between vitamin D and myocardial infarction. However, in another study by Arad et al. [25] no such association was seen.
In our analysis only age and serum PTH turned out to be independent predictors of CHD in both sexes, when adjusted for BMI, total serum calcium, serum cholesterol and systolic blood pressure. In the multiple logistic regression analysis with PTH entered as quartiles, PTH was a significant predictor of CHD at levels above 3.5 pmol/l in men and 3.3 pmol/l in women. This indicates that serum PTH leads to increased risk for CHD even within the reference range, but in the highest quartile only.
This association between PTH levels and CHD is, of course, no proof of a causal relation. However, there are mechanisms by which PTH could have harmful effects on the cardiovascular system, both directly and indirectly. Thus, receptors for PTH have been identified in the heart [26], and in-vitro studies have indicated an effect on isolated cardiomyocytes causing them to hypertrophy [27]. PTH also increases the entry of calcium into the cardiomyocytes [28], and may have effects on relaxation due to altered endothelium-dependent vasodilatation [29]. Indirectly, PTH may also have an effect on development of heart disease as there is a positive association between PTH and BMI [22] and also between PTH and blood pressure [30].
The present study has several shortcomings. The presence of CHD was based on that reported on the medical history questionnaire and not confirmed by medical records. However, inclusion of subjects without CHD in the group with CHD, and subjects with CHD in the control group, would probably reduce the relations found and not create them. Furthermore, the study was retrospective and the observed associations, in addition to reflecting covariations with cardiovascular events, may also be the result and not the cause of CHD.
In spite of this, we feel that our results add to the number of indications that an elevated serum PTH may have harmful effects on the heart, and that large prospective studies with supplementation of calcium and/or vitamin D to subjects with elevated serum PTH levels are indicated.
Footnotes
Acknowledgements
The superb technical assistance by Inger Myrnes and Astrid Lindvall is gratefully acknowledged.