
Abstract
The epidemic of obesity and overweight poses a major challenge to the prevention of chronic noncommunicable diseases throughout the world. In some developing countries it presents a double burden alongside enduring problems of undernutrition.
Current IOTF estimates suggest that at least 1.1 billion adults are overweight including 312 million who are obese. The prevalence of obesity has doubled or even risen threefold in less than two decades, while in children this is rising at an even faster rate in some regions of Europe to levels of up to 36% in parts of Italy and elsewhere.
The comparative burden of disease due to raised body mass index is among the top five leading risk factors in both developed and low mortality developing countries. When viewed in conjunction with the burden of raised cholesterol and hypertension, these components of the metabolic syndrome form the major cause of mortality and disease in Europe and are guaranteed to increase with the rising trend in overweight and obesity while amplifying the burden of cardiovascular disease. The increase in childhood obesity will, unchecked, accentuate the rise in early adult type 2 diabetes and cardiovascular disease.
Conclusion
A fundamental policy shift is required to widen responsibility for the prevention of diet, activity and weight-related ill health across the whole of Europe's population. Only such a comprehensive approach offers any realistic prospect of averting a public health catastrophe for Europe and indeed for the whole world.
Introduction
The epidemic of obesity and overweight poses a major challenge to the prevention of chronic non-communicable diseases throughout the world. In some developing countries it presents a double burden alongside the enduring problems of undernutrition, recognized in the World Health Organization (WHO) report, Obesity-preventing and managing the global epidemic [1].
Current International Obesity TaskForce (IOTF) estimates suggest at least 1.1 billion people are overweight and 312 million of them obese [body mass index (BMI) ≥ 30]. In many countries more than half the adult population is overweight and 20-30% of adults are categorized as clinically obese in Europe, where prevalence has doubled or even risen threefold in less than two decades. In the USA prevalence is higher still with obesity affecting 31% of all adults, but with even more elevated levels among certain subgroups. More than half of black American women are obese, with almost one-third of that group having a BMI ≥ 40 [2].
The prevalence of overweight and obesity among children is rising at an even faster rate. In Europe rates are escalating with up to 36% affected in some regions. The increasing evidence of type 2 diabetes among children and adolescents, a disease confined largely to older adults little more than a generation ago, indicates the seriousness of the childhood obesity problem [3]. There is evidence from many regions to illustrate that this is not confined to western populations. The recent evaluation of a mass screening programme of children in Taiwan identified a 6: 1 ratio of type 2 to type 1 diabetes, with obesity a major risk factor. The odds ratio for type 2 diabetes in obese children (above the 95th centile) was 18.8 compared with those at the 50th centile [4].
Obesity, particularly abdominal obesity, is a substantial risk factor for cardiovascular diseases. In addition factors such as elevated fasting blood triglycerides, low levels of high-density lipoprotein cholesterol, high fasting blood glucose and hypertension are accentuated markedly by weight gain. A combination of two of these factors together with a large waist circumference is a common diagnostic set of criteria, including the ATP III for what is now termed the metabolic syndrome.
The metabolic syndrome is common, but poorly recognized and is therefore inadequately treated. As many as 47 million adult Americans are affected with a recent analysis of US data from the National Health and Nutrition Examination Survey (1988-1994) identifying the early onset of metabolic syndrome in an estimated one million youngsters aged 12-19, or 4.2% of all teenagers. The syndrome was notably present in 28.7% of obese adolescents-four times the 6.8% level found in ‘at-risk’ overweight adolescents. The syndrome occurred in only 0.1% of those classified below 85th centile [5].
The diagnostic thresholds shown in Table 1 were proposed by the National Cholesterol Education Program (NCEP) in the United States in 2001 [6]. The treatment guidelines emphasize weight management and increased activity. A comparison with WHO criteria undertaken by the US Centers for Disease Control demonstrated that the NCEP tended to underestimate the syndrome's prevalence, with a marked variation in the detection of African American men and concluded that a common definition needs to be agreed [7].
Comparable data for Europe are limited. The European Group for the Study of Insulin Resistance (EGIR) reported an analysis of eight European studies showing that among non-diabetic subjects the frequency of the syndrome, invoking WHO criteria, varied between 7 and 36% for men age 40 to 55 years and for women of the same age, between 5 and 22%. Using the EGIR's own criteria, the syndrome appeared less frequently and particularly in men due to the differing definitions of central obesity: the WHO definition included simply a BMI ≥ 30 [8]. However a recent re-evaluation of data applying adapted NCEP criteria to the West of Scotland Coronary Prevention Study showed that the identification of metabolic syndrome predicts coronary heart disease events, and type 2 diabetes, enabling identification of those most likely to benefit from lifestyle measures to prevent these diseases [9].
The driving force behind the obesity epidemic and the consequent widespread metabolic syndrome is a diet dominated by an excess of energy-dense foods, high in fat, sugar (and in addition salt) combined with an insufficient consumption of fruits and vegetables. This dysfunctional diet is compounded by predominantly sedentary lifestyles and reduced opportunities for physical activity [10].
Prevalence
Figure 1 illustrates the range of obesity levels reported across Europe, reflecting differential progress of the obesity epidemic, but also variations in the age of surveys [11]. Few countries have undertaken regular, reliable national population surveys. However available studies suggest prevalence may vary from 5% of women and 6% of men in Switzerland to 35% of women and 22% of men in Malta. In the United Kingdom, Finland and Germany more than one in five adults are obese, but recent data from the Health of England Survey 2001 showed that almost one in four women are obese and of those, one in 10 is morbidly obese.
Even higher levels have been found to be prevalent in parts of Eastern Europe. Selective data from the WHO MONICA Study in middle-aged adults show almost 40% of Russian women above BMI 30 in certain towns in the mid-1980s, but national data suggest overall 25% of adult women and 10% of men are obese - a similar prevalence to that of Turkey [12]. A study of Russian males in West Siberia noted low physical activity and a high incidence of obesity among 10677 railway workers who had experienced the ‘nutritional shift’ to a high fat diet [13].
Diagnostic thresholds for metabolic syndrome. Clinical identification of the metabolic syndrome - any three of the following
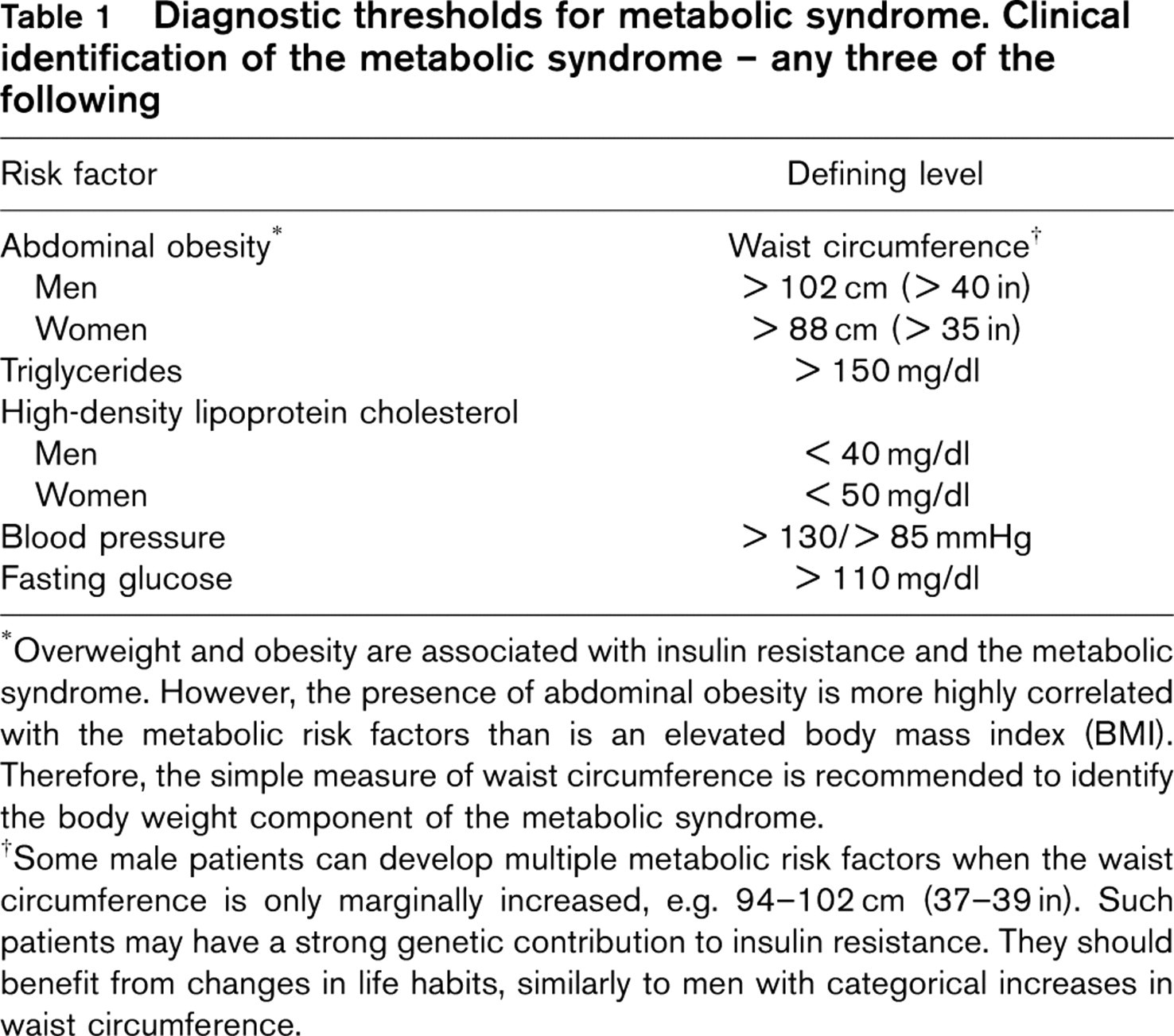
∗Overweight and obesity are associated with insulin resistance and the metabolic syndrome. However, the presence of abdominal obesity is more highly correlated with the metabolic risk factors than is an elevated body mass index (BMI). Therefore, the simple measure of waist circumference is recommended to identify the body weight component of the metabolic syndrome.
†Some male patients can develop multiple metabolic risk factors when the waist circumference is only marginally increased, e.g. 94-102 cm (37-39 in). Such patients may have a strong genetic contribution to insulin resistance. They should benefit from changes in life habits, similarly to men with categorical increases in waist circumference.
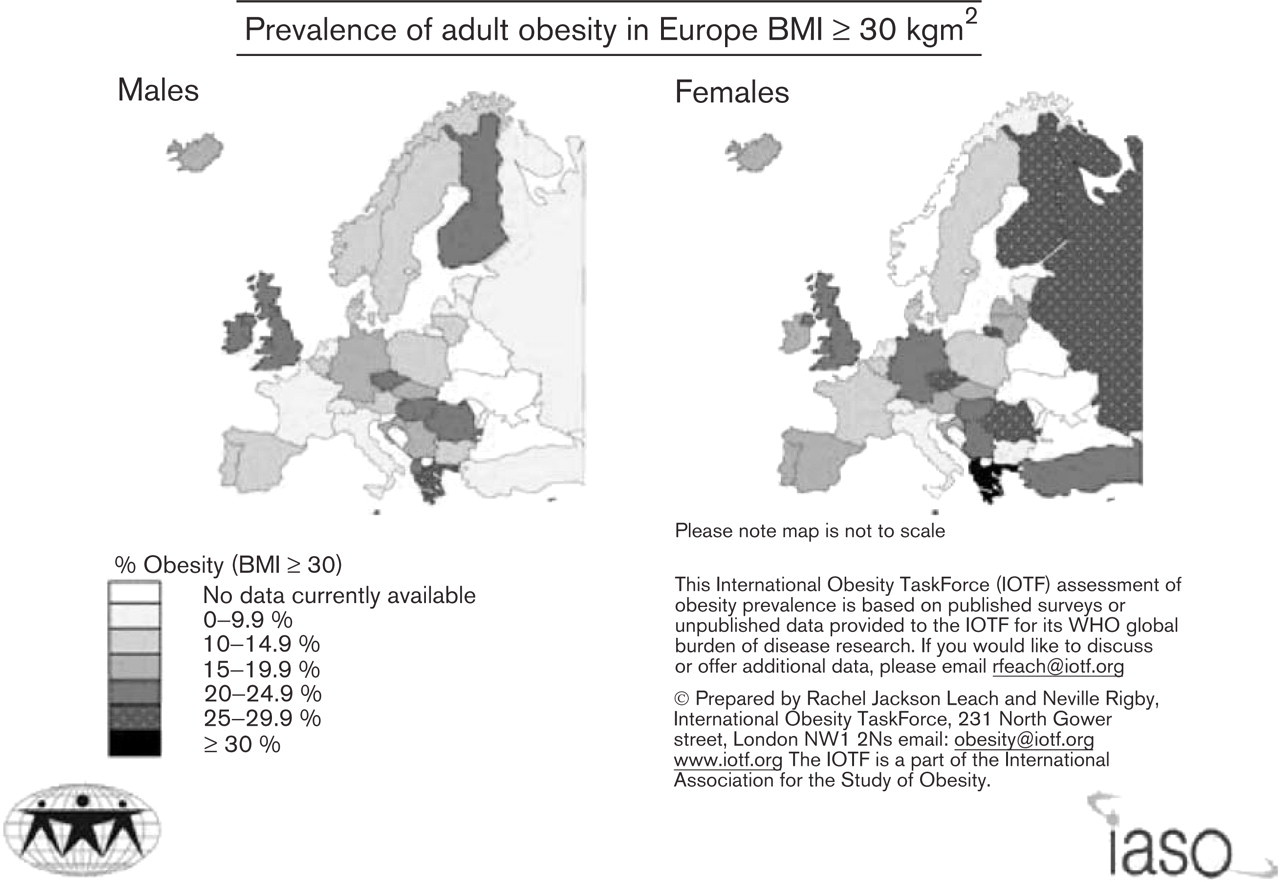
Prevalence of adult obesity in Europe BMI > 30 kgm2
Upward trends
The trend is consistently rising although the rate of increase varies. Scandinavian populations with greater inclination towards outdoor activities are still affected. Thus in Denmark data from the WHO MONICA project show that those with BMIs > 25.0 increased from 10 to 13% in men, and from 9 to 11% in women over a 10-year period up to 1992 [14]. Moreover, national data show Finland's prevalence of 19% for men and women in 1997 is almost double the 10% level of 1979 [15]. In Sweden obesity rates rose from 6.6% of men and 8.8% of women in 1981 to 10% of men and 11.9% of women in 1997 [16]. The contrast with the UK is marked: from the same base of 6% of men and 8% of women in 1980 to obesity levels of 21% of men and 23.5% of women in 2001 [17]. No European country has stopped the accelerating epidemic and its impact is still largely unrecognized.
Burden
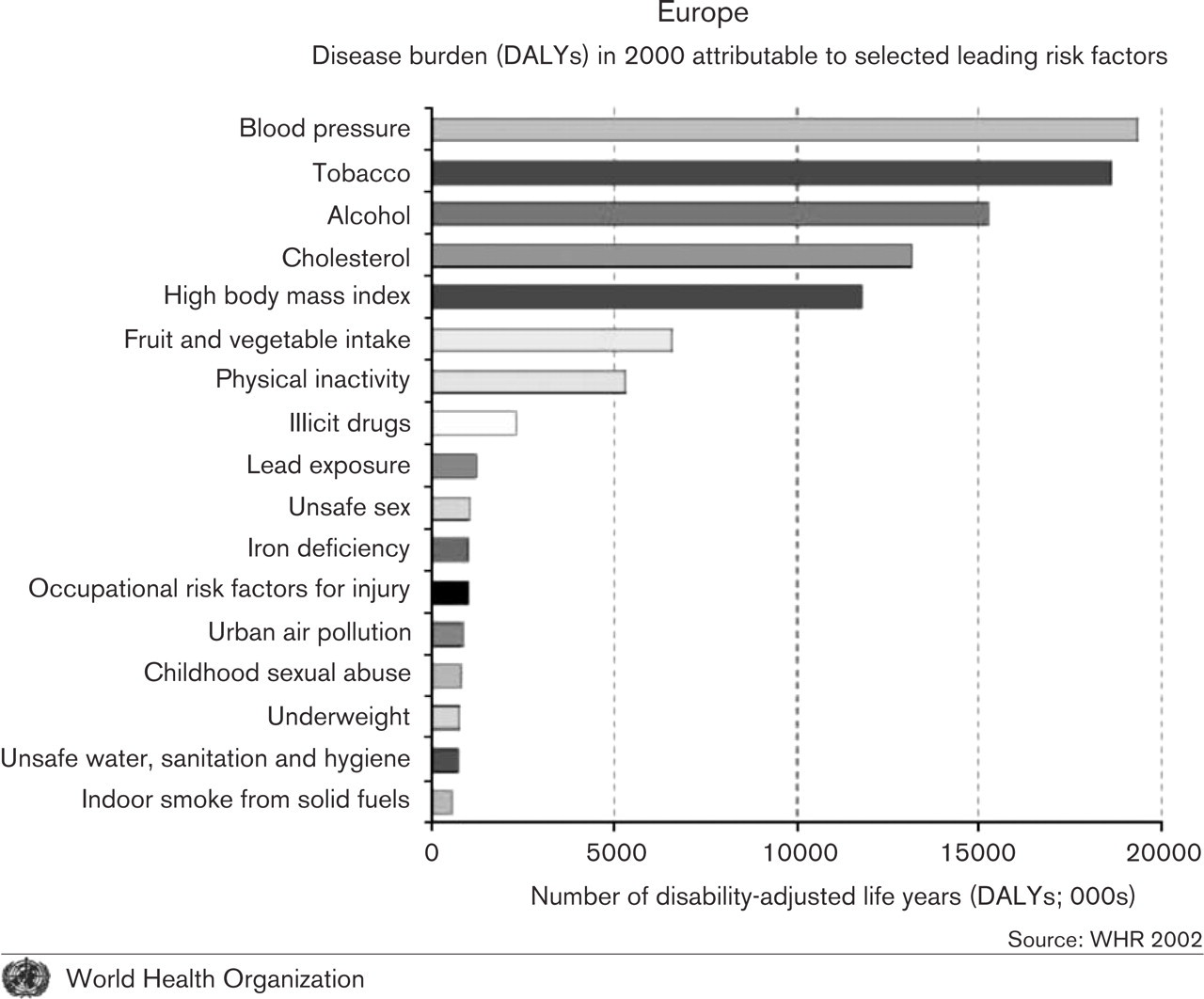
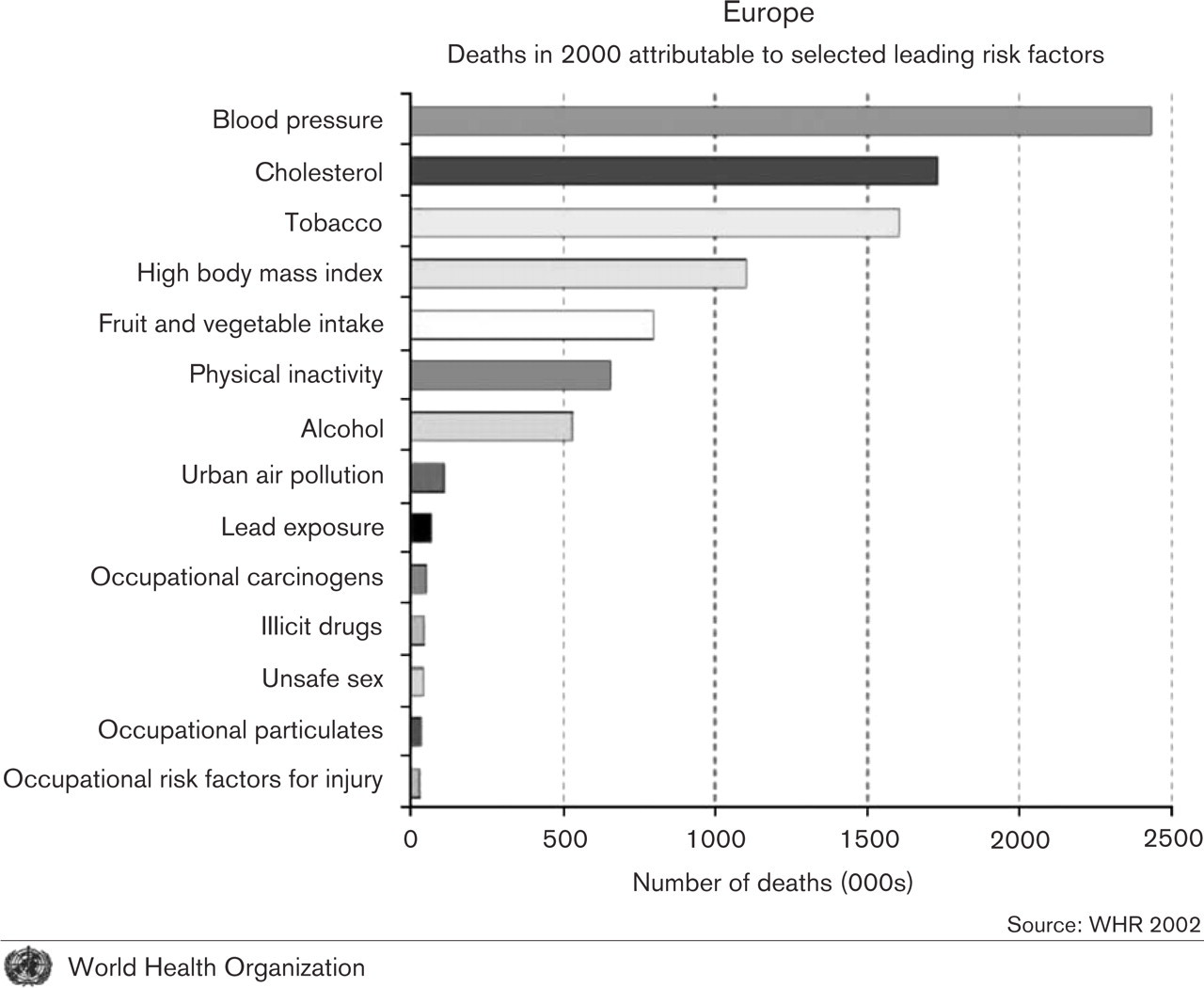
The comparative burden of disease due to raised BMI is illustrated in Figures 2 and 3, incorporating IOTF analyses for the WHO global burden of disease project. These show that raised BMI is among the top five leading risk factors for the burden of disease, and fourth in the causes of death. When viewed in conjunction with the burden of raised cholesterol and hypertension, it is clear that these components of the metabolic syndrome form the biggest single cause of mortality and disease in Europe. Table 2 shows the burden of disease, calculated in disability-adjusted life years (DALYs), in a global context, where the cluster of hypertension, raised cholesterol and raised BMI feature strongly in both developed and low mortality developing countries, where poor dietary intake and physical inactivity are also significant factors.
Cardiovascular diseases and diabetes are intimately related. At present diabetes prevalence varies from 2% in Iceland to more than 10% in Bulgaria and Germany. Overall, the diabetes prevalence in Europe in 2003 is estimated at 7.8% for adults aged 20-79 years. In addition impaired glucose tolerance is estimated to affect 10.2% of adults. A very high proportion is type 2 diabetes, and this is guaranteed to increase with the rising trend in overweight and obesity while amplifying the burden of cardiovascular disease. Already around 20% of the four million annual deaths in Europe due to heart disease occur before the age of 65, and much of this premature mortality could be avoided.
Risks relating to cancer have been evaluated by the International Agency for Research into Cancer. An expert group concluded that excess body weight and physical inactivity were the most important avoidable causes of a range of cancers, accounting for approximately one-quarter to one-third of breast cancer, and cancers of the colon, endometrium, kidney (renal cell) and oesophagus (adenocarcinoma). Overall excess body weight accounts for an estimated 5% of all cancers in the European Union, (3% in men and 6% in women), with 27 000 male and 45 000 female new cancer cases each year from this cause alone [18].
World Health Organization
World Health Organization
Burden of disease due to leading regional risk factors. Attributable disability-adjusted life years (DALYs) by risk factor as a percentage of regional DALY (ranking within region)
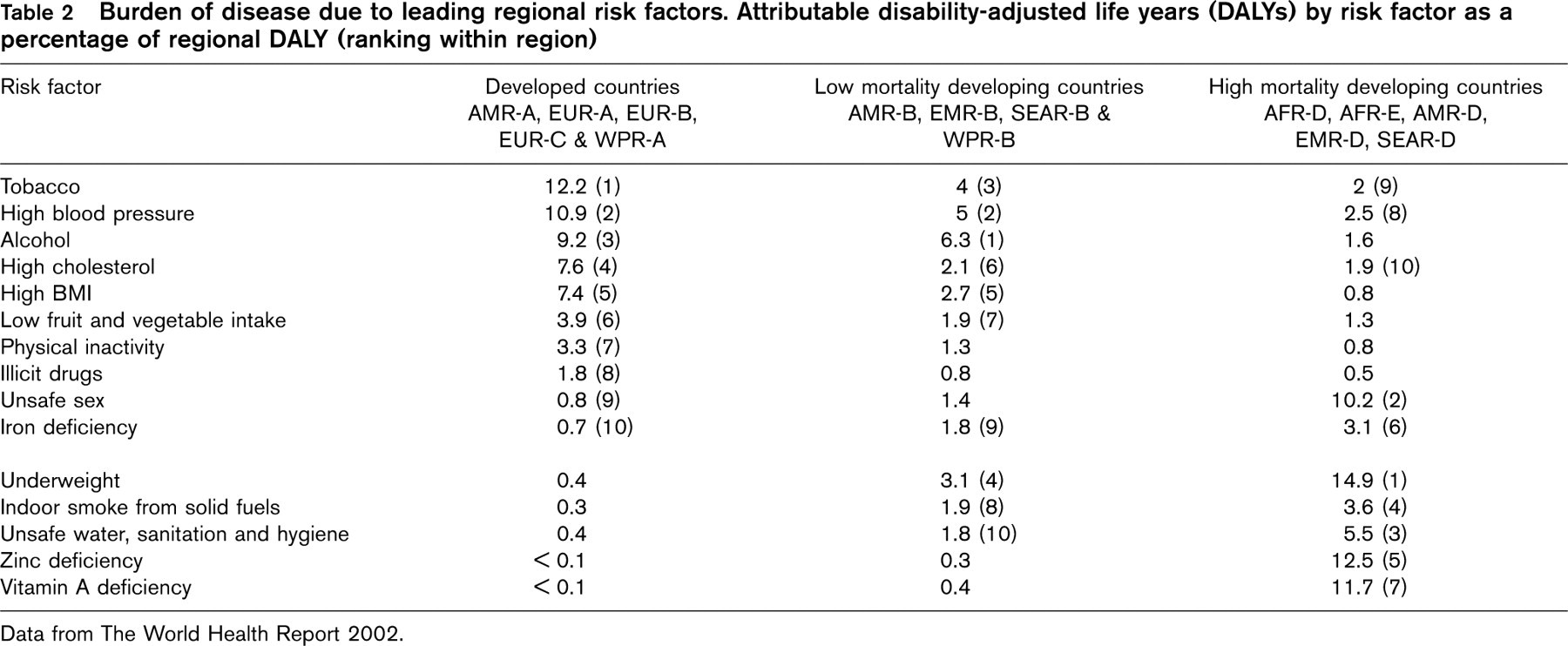
Data from The World Health Report 2002.
Bearing the cost
The costs of obesity and its co-morbidities are routinely underestimated with crude estimates of costs amounting to 7% of total health care budgets in some countries. In England, the National Audit Office estimated costs of £3 billion (2003 adjusted) [19], while recent estimates of diet-related disease overall were as high as £15 billion [20]. In Germany estimates have even suggested costs of 20 billion DM at 1995 values [21] (equivalent to US$14.3 billion at the time). An IOTF working group has developed a new approach to evaluating the economic costs of obesity, related co-morbidities and consequential losses in terms of quality of life, disability and years of life lost. This should allow a more realistic assessment of the economic impact of obesity to be made in the future.
Childhood
Obesity affects one in five children in some age groups in many countries. Some youngsters manifest early insulin resistance, plasma lipid disturbances and higher blood pressures and in some cases develop frank non-insulin-dependent diabetes mellitus and cardiovascular disorders in adolescence. Data for childhood obesity, using the IOTF's criteria for evaluating childhood and adolescent overweight and obesity (relating this to WHO adult cutoff levels of BMI 25 and BMI 30), illustrate wide variations, with a surprising north-south European gradient with the highest prevalences in the Mediterranean countries, e.g. 36% in Italy. This increase in childhood obesity prevalence will, unchecked, markedly accentuate the rise of early adult type 2 diabetes and cardiovascular disease.
Strategies to arrest the epidemic
The IOTF has made a series of recommendations to encourage comprehensive strategies in Europe and elsewhere to address the problem of overweight and obesity. A recent IOTF position paper, Obesity in Europe 2, prepared for an EU ministerial conference in Milan convened to consider healthy lifestyles, recommended a set of actions to address the ‘toxic obesity-inducing environment’ which predisposes large sections of the population to overweight and obesity [22, 23]. An earlier document, prepared in collaboration with members of the European Association for the Study of Obesity's task forces on management, prevention and childhood obesity, was published for the European Union's Obesity Summit meeting in Copenhagen in September 2002 [24]. Subsequently the EU council of health ministers adopted a strengthened position, increasing funding for research. The European Commission also adopted a stronger position, most recently expressing a resolve to act on the issue, with food labelling one of the key targets for action.
In September 2000 all 50 participating member states within WHO Europe approved the First Action Plan for Food and Nutrition Policy, which emphasized concerns about overweight and obesity in the context of food safety and nutrition. Governments in Europe have been slow to respond but will be called to account in a review of actions taken in 2005. The European Union is reviewing the impact of television advertising on children, but needs to adopt a broader vision to regulate and modify the marketing of the foods high in fat, sugar and salt which contribute to the obesity epidemic and the rising levels of heart disease.
No longer can we take just the individual approach to preventing cardiovascular disease: we have to recognize that the European population is getting heavier with all its accompanying cardiovascular risk factors. So a fundamental policy shift is required to widen responsibility for the prevention of diet, activity and weight-related ill health across the whole of Europe's population to encompass non-health sectors such as culture, commerce, education, transport and planning. Only such a comprehensive approach offers any realistic prospect of averting a public health catastrophe for Europe and indeed for the whole world.
{kind=link}