
Abstract
Background
To do a gender comparison of absolute risk of recurrent myocardial infarction (MI).
Design
Registration of all first and second MI amongst Icelandic males and females 1981–1999.
Methods
The whole of Icelandic population, 40–74 years of age.
Results
The mean recurrence rate (second attack) for men was 45.7/1000 MI survivors/year and for women 39.0/1000 per year. The male/female (M/F) ratio was 1.17, 95% confidence interval 1.00–1.37, P = 0.05 and did not change significantly with age. The M/F ratio for first MI in comparison was two to seven, lowest in the oldest group. The recurrence rate decreased significantly and similarly in both sexes during the observation period.
Conclusion
The absolute risk of MI is closely similar amongst both sexes and has decreased similarly suggesting that the same kind of secondary intervention is effective amongst both sexes in a general population. Eur J Cardiovasc Prevention Rehab 11:121–124 © 2004 The European Society of Cardiology.
Introduction
The risk of first myocardial infarction (MI) is two- to seven-fold amongst men compared to women. This risk ratio decreases with age [1, 2]. This excess amongst men has been explained by some protective effect associated with the female sex. One such favourable factor is higher concentration of high-density lipoprotein amongst women [3]. The MONICA study has shown that women are more likely to die in hospital when presenting with acute myocardial infarction whereas the pre-hospital mortality is higher amongst men [4]. This might suggest that male/female differences may be due to sex differences in the disease pathophysiology rather than treatment bias. A gender comparison of long-term recurrence rate for acute MI has been infrequently reported on. Such information might, however, be of importance especially with regard to possible gender-specific therapies. We have therefore looked at the rate of first episode of recurrent MI amongst both sexes for the whole of Iceland 1981–1999.
Study population and methods
The registration of MI in people aged 40–74 years has been conducted for the whole of Iceland (population 280,000) for the years 1981–1999 according to the MONICA criteria [5] (definite and possible acute myocardial infarction or coronary death). Possible cases were found by reviewing a centrally compiled register of case files of all living patients with discharge diagnoses of 410–411 and fatal cases with diagnoses of 410–414 according to ICD-9, as well as all death certificates and all autopsy records.
We have looked specifically at the first MI and the first episode of recurrent MI (occurring more than 28 days after the first MI) amongst both sexes in the age group 40–74 years. Follow-up time started 28 days after the first MI and extended until the date of first recurrent MI or coronary heart disease (CHD) death or the date of censoring (December 31, 1999). Those individuals who had a previous myocardial infarction according to the MONICA protocol before the study started in 1981 were excluded from the analysis. The MONICA Data Centre in Helsinki generated quality scores for coronary event and demographic data in the MONICA project ranging from 0 (denoting at least one serious problem with the data) to a perfect score of 2.0. The quality score for coronary events for Iceland was 1.8 [6].
Statistical methods
All events of MI in Iceland 1981–1999 were available with date of MI and date of death, (if dead), together with population figures. Sex and age-specific incidence rates (5-year age intervals) were obtained for first MI and expressed per 1000 persons in age range 40–74 years. Numbers of first recurrence (second MI) were counted according to sex, 5-year age interval and 5-year calendar period for those surviving more than 28 days after their first MI and expressed as number per 1000 persons alive having sustained one MI. Risk period of a second MI was computed as the time elapsed from 28 days after the first MI until second MI or death, or December 31, 1999 or age 75 years, whichever occurred first. Recurrence rates were calculated as the number of second MI's divided by the number of risk years.
Cox regression was applied to assess the dependence of the risk of second MI on gender. By including these variables into the regression an adjustment to age and calendar time was made. Curves for cumulative risk were computed from the results.
Results
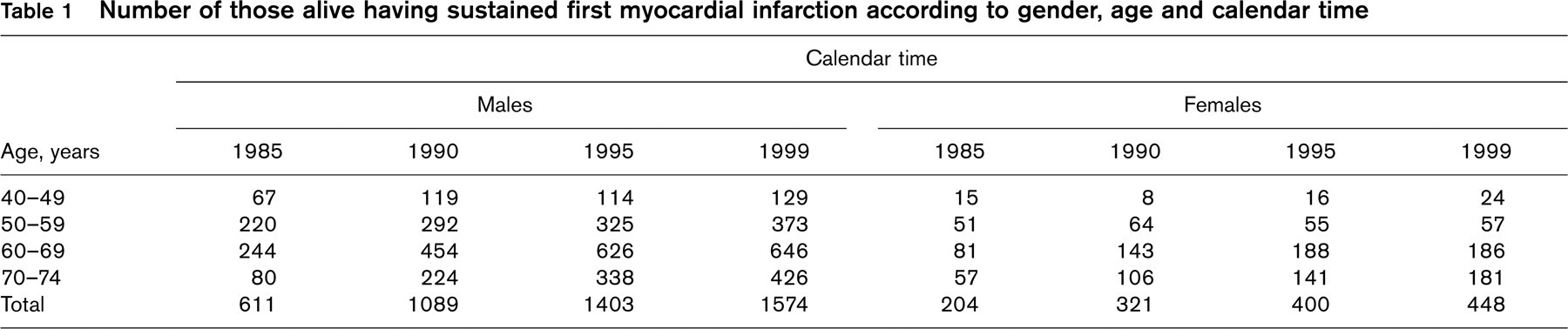
We identified 2891 male and 1004 female survivors after their first MI during the years 1981–1999 in the age range 40–74 years. Of those 762 men suffered first recurrent MI (second MI) during this time period, 346 fatal and 416 non-fatal cases. One hundred and ninety-five women suffered first recurrent MI (second MI), 87 fatal and 108 non-fatal. Table 1 shows the number of men and women who had survived the first MI and were alive at different time periods. The mean age at first MI for men was 60 years and the mean duration of follow-up 5.7 years. For women the corresponding figures were 64 years and 5.0 years of follow-up. The mean time-to-recurrent MI was 3.6 years for men and 3.2 years for women. The total follow-up person years for men was 16700 and for women 5000.
Table 2 shows the incidence rate of first MI and recurrence rate (second MI) in Iceland between 1981–1999 and the M/F ratio for both rates. The mean recurrence rate (second event) during the years 1981–1999 was for males 45.7/1000 MI survivors/year and for females 39.0/1000/year. The crude risk ratio of males versus females was 1.17 [95% confidence interval (CI) 1.00–1.37, P = 0.05].
Figure 1 shows the cumulative percentage of those who had sustained a second MI adjusted for age and adjusted to calendar time year 1985 and 1995. The risk ratio adjusted to age and calendar time was 1.34 (95% CI 1.14–1.57, P<0.001) calculated by Cox regression. The difference between this figure and that obtained by crude mean recurrence rate (1.17) was not significant (P = 0.24). The decline in rate of second event of MI between 1981–1990 and 1991–1999 was 47% for men and 49% for women, the difference was not significant, P = 0.83.
Discussion
Our study, which has the advantage of analysing a complete registration of all MI for the whole of Iceland, has shown a closely similar rate of first recurrent MI amongst men and women. This applies to all age groups from 40–75. It is notable that the recurrence rate in our population-based study group was closely similar to that in the control group in the HERS study in USA [7].
Our study has confirmed the two- to seven-fold increased risk amongst men compared to women to sustain the first MI, which is closely similar to the findings in the Framingham study [1]. Women and men share the same major risk factors for CHD although women experience a lower absolute risk [8]. Several studies have shown that primary cardiovascular risk factors remain important after MI [9, 10]. Our study has shown that after the first MI the female advantage over men is lost to a large extent.
Number of those alive having sustained first myocardial infarction according to gender, age and calendar time
The incidence and first recurrence of myocardial infarctions in Iceland 1981–1999. Numbers, rates per 1000 per year and male/female ratio (M/F) according to age and calendar period
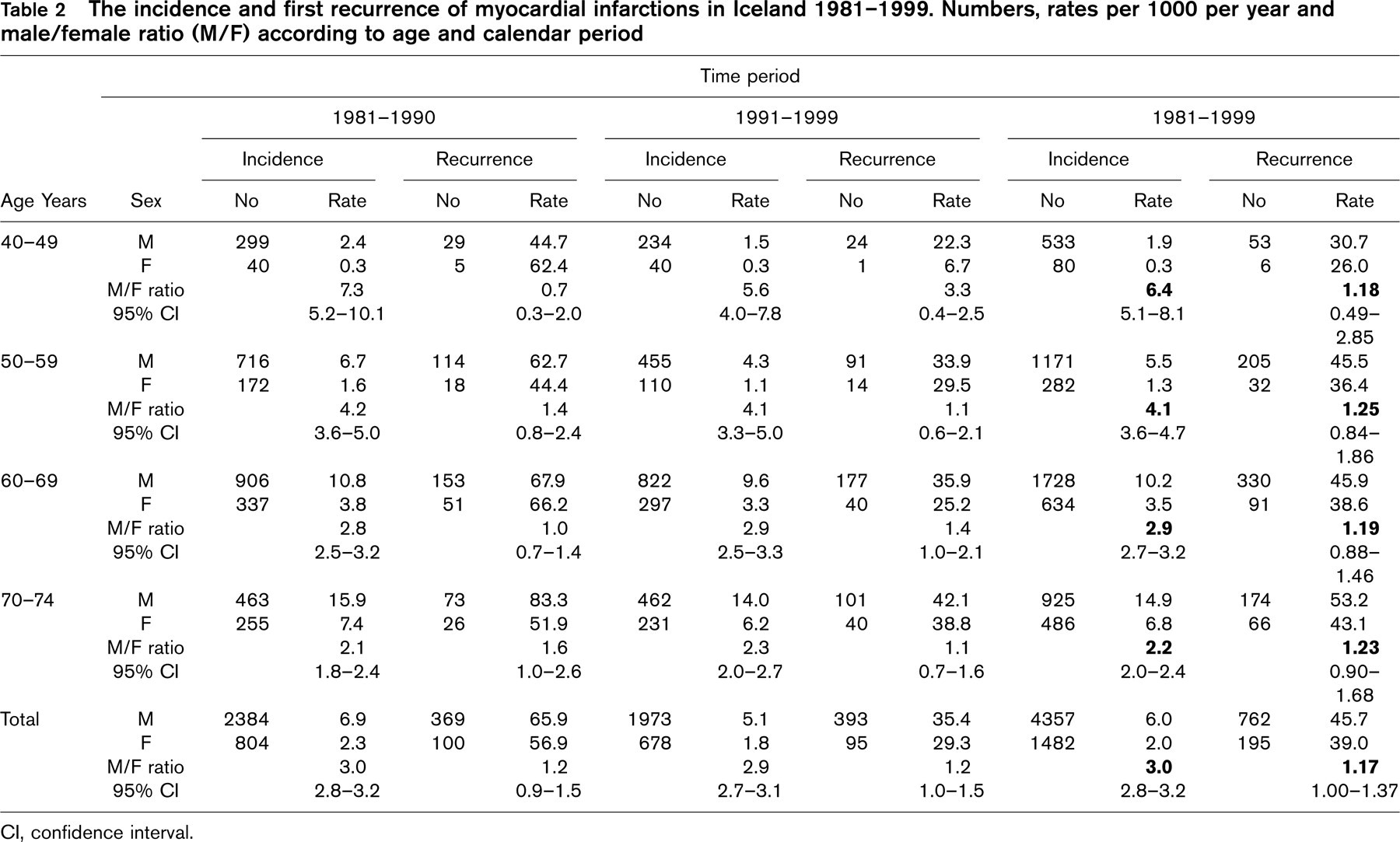
CI, confidence interval.
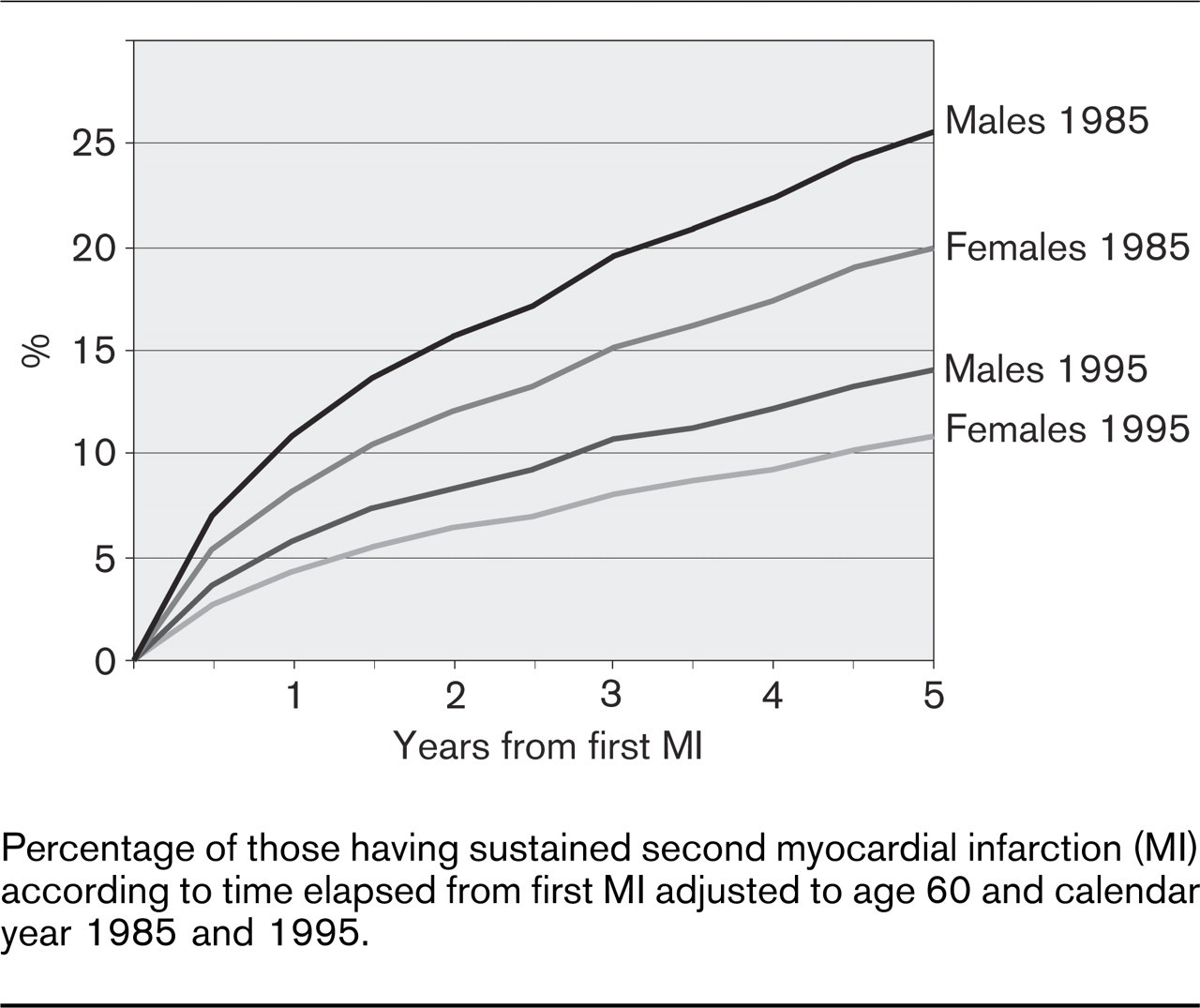
Percentage of those having sustained second myocardial infarction (MI) according to time elapsed from first MI adjusted to age 60 and calendar year 1985 and 1995.
This is reflected in the finding that the risk of a 60-year-old woman to sustain the second MI is five-fold greater than the risk of a 60-year-old woman to suffer the first MI. For men this risk ratio is two-fold (data not shown).
Previous studies on gender difference have mostly looked at survival post-MI and have given inconsistent results [11–14]. Some studies indicated a worse prognosis for women than men after MI, particularly black women [13]. The Framingham Heart Study showed that twice as many women as men suffered another heart attack [12]. This discrepancy may be explained by different study groups since some studies have included the in-hospital mortality and others not [11–13]. It is well known from the international MONICA study (including ours) [6] and other studies [15–17], that women have higher in-hospital mortality for an unexplained reason, but the overall 28-day mortality is closely similar for both sexes. Many of these studies were based on data from clinical trials and may not correctly represent the average MI patient. The FINMONICA Study showed, however, a similar recurrence rate amongst both sexes but higher mortality rate amongst men [18]. Similar to that study our results showed that the average time interval from first to second event was comparable in both sexes.
Several secondary intervention studies have shown similar positive results for both sexes [10, 19–21], which suggests that the same approach could be used for men and women post-MI. A gender-specific therapy, for example estrogen therapy, has, on the other hand, not turned out to be effective [22]. Our study would therefore support the notion that the same approach should be used for both sexes to prevent recurrence of MI. This is further supported by the fact that a similar striking decline in recurrence rate of MI was observed for both sexes when looking at the period 1981–1990 and 1991–1999. This great improvement in preventing recurrence may possibly be explained by a considerable increase in the usage of effective preventive measures, especially well proven in secondary prevention studies [19–21]. Thus, between 1986 and 1996 the use of aspirin increased more than six-fold in MI patients in Iceland, the use of beta-blockers increased by 31% (from 47.5–62%), the use of thrombolytics increased three-fold and the use of invasive coronary artery procedures has increased six-fold [23]. Since the results of the Scandinavian 4S Study were published in 1994 [10] the usage of statins has increased considerably.
The Icelandic experience has thus proven similar effectiveness of secondary prevention amongst both sexes by changes in life-style and risk factors [24] as well as by usage of medical and surgical advances in acute and long-term care of coronary heart disease patients.