
Abstract
Background
Ventricular arrhythmia is a risk factor for myocardial infarction and mortality but many individuals with this abnormality live long and healthy lives. The aim of this study is to analyse the prognostic significance of frequent and complex ventricular arrhythmia in men who differed regarding ability to adapt to a stressful situation.
Design
Prospective cohort study.
Methods
The serial Color Word Test is a semi-experimental way to assess how individuals behave in a stressful encounter. This test was included in the prospective cohort study ‘Men born in 1914’ together with 24-h ambulatory electrocardiographic recordings at a baseline examination in 1982/83. Behaviour in the test was categorized as either adaptive or maladaptive. Behaviour in the test and occurrence of ventricular arrhythmia at baseline were analyzed in relation to incidence of myocardial infarction and mortality during approximately 14 years of follow-up.
Results
Multivariate analyses showed that ventricular arrhythmia was not associated with the incidence of myocardial infarction or all-cause mortality in the presence of an adaptive behaviour. Ventricular arrhythmia together with a maladaptive behaviour was associated with the incidence of myocardial infarction [relative risk (RR) 2.43; 95% confidence interval (CI) 1.37 to 4.31] and with all-cause mortality (RR 1.56; 95% CI 1.01 to 2.41) during follow-up.
Conclusions
A maladaptive behaviour in a stressful encounter makes men with electrocardiographically detected ventricular arrhythmias more vulnerable and thereby exposed to an increased risk of a future myocardial infarction and overall mortality.
Introduction
The increased incidence of myocardial infarction (MI) and death associated with ventricular arrhythmia (VA) has been demonstrated both in clinical and population-based studies [1–4]. The prognostic significance related to this abnormality is, however, far from uniform because many remain alive and healthy even in advanced age. This difference in outcome suggests a potential for prevention but the factors and circumstances that may influence vulnerability have so far received relatively little scientific attention.
The central nervous system is involved when psychological stress is experienced and, through the heightened sympathetic and hypothalamic activity which is caused by the stress experience, the cardiac autonomic tone is set [1]. The electrical stability of the myocardium is thereby decreased and the threshold for ventricular arrhythmia is lowered [5–7]. Psychological stress may in itself produce ventricular arrhythmia by sympathetic activity and increased levels of catecholamine [7]. Consequently, a natural link between stress and arrhythmia exists.
‘Men born in 1914’ is a prospective study of the distribution and incidence of cardiovascular disease in ageing men. The baseline assessments took place in 1982/83 and 24-h Holter monitoring was included. The occurrence of complex and frequent ventricular arrhythmias was associated with an increased risk of an MI and mortality in ischaemic heart disease (IHD) during the approximately 10-year follow-up [2].
In the study, the serial Color Word Test (CWT) [8] was used to assess how individuals managed and adapted to a cognitive conflict task. The test is a version of the Stroop test [9], which was designed for the study of interference. The serial model of the CWT was founded on a model where perception and personality are considered a unit [10]. Personality determines which strategies an individual utilizes when controlling needs, when mediating between conflicting needs, or when adjusting needs to reality. Through ontogenesis, certain strategies become preferred or habitual and these characteristic strategies are also used when the individual has to adapt to new and conflicting demands. By constructing a serial CWT, where temporal aspects of behaviour could be studied from start until final mastery, these strategies would become evident.
The Stroop test or the CWT has been used to induce stress in many experimental studies on the relationship between psychological stress and the cardiovascular system [11, 12]. We have previously shown, in this male cohort, that inability to adapt to the stressful situation, as assessed by the CWT, was associated with an increased vulnerability among those exposed to hypertension [13, 14]. Two categories of behaviour in the stressful encounter were applied: adaptive and maladaptive. Men with an adaptive behaviour are assumed to view the cognitive task in a more objective manner and will not let themselves be disturbed by irrelevant stimuli although a certain amount of fatigue could hamper performance level towards the end of the session [8]. The maladaptive behaviour reflects repeated efforts and failures to find and maintain successful strategies in managing the conflict. Men with this behaviour are supposedly influenced by more subjective perceptions and by a sense of gradually losing control [15].
The objective of this study is to compare the incidence and prognostic significance of ventricular arrhythmia in groups defined in terms of ability to adapt to a stressful situation.
Methods
Study population
‘Men born in 1914’ is designed as a prospective cohort study on the epidemiology of cardiovascular diseases in men. At baseline in 1982/83, 621 men, all born in an even numbered month of 1914, were invited to take part in an extensive health examination. All men were residents of the city of Malmö, the third largest city of Sweden. Five hundred (80.5%) men participated in all, or parts, of the investigations. In a special study of non-participants in this health-survey, findings indicated that men who declined to take part in the study were more likely to belong to a lower socio-economic class, be single or hospitalized, and have negative attitudes towards participating in health-surveys [16]. The cohort of this study included 408 men who had participated in the serial CWT and had analysable data from the 24-h electrocardiographic (ECG) examination.
Myocardial infarctions and mortality
All men were followed from baseline measurements in 1982-83 until the occurrence of a MI, death, or 31 December 1996. An MI was defined as a fatal or non-fatal MI, corresponding to the International Classification of Diseases, Ninth Revision (ICD-9) codes 410 and 412 [17]. All cases were obtained from the Malmö Myocardial Infarction Register [18] and only the first MI during follow-up was used for the analyses. Mortality due to IHD corresponded to ICD-9 codes 410-414.
Mean follow-up time for an MI was 10.3 years (range 3 months to 14 years 4 months) and 11.0 years for mortality (range 3 months to 14 years 4 months). Mortality and cause of death have continuously been registered by records linked to the National Cause of Death Register. Event rates were expressed as MIs or deaths per 1000 person-years of observation.
Adaptive behaviour - the serial Color Word Test
Description
A semi-experimental design, the serial Color Word Test [8], was chosen to assess how individuals cognitively manage and adapt in a conflict situation. The origin of the test is the Stroop test [9]. The design of the test is very simple. On a sheet of paper the words ‘yellow’, ‘blue’, ‘green’, and ‘red’ are printed in an incongruent colour, in a design of 10 words × 10 rows. The object of the test is to name the colour in which the word is printed and ignore the written word. The challenge is, thus, to handle the interference, which in this case is the conflict between reading what is printed, and naming the colour in which the word is printed.
Administration and scoring
The men were presented with the test and asked to name the colour of the print as quickly and correctly as possible. The serial version of the Color Word Test is a construction where five identical tests are repeated and each repetition is labelled a subtest. Scoring of each subtest was made by the test administrator after 20, 40, 60, 80 and 100 responses and was expressed as time consumption in seconds. The scoring was straightforward as every two rows in the test were given a time measure. Before the actual test started, an opportunity to practise was given.
When classifying behaviour in a test session it is possible either to regard behaviour as dependent on the particular context or on the individual's personal history and development [19]. The former type of behaviour can be called situational and is categorized according to which particular pattern that occurs most frequently during the test session. Behaviour, dependent on the person, is labelled habitual because it is assumed to reflect how an individual generally behaves in challenging cognitive tasks. Different patterns of habitual behaviour can be categorized by analysing the temporal aspects of behaviour, which also allows us to regard cognitive adaptation as a process. This process is two-dimensional, consisting of both linear change (of time consumption), the Regression, and of nonlinear change, the Variability. All test-scores are compared with the reference medians of the entire cohort [20] whereupon four patterns of adaptation in each dimension are categorized. The four patterns are equally named in both dimensions. Detailed information on the administration and analyses of the test is found in the manual [8], recently revised and translated into English [21].
To distinguish among the patterns it is possible to describe them in the following manner. The Stabilized patterns show even and stable time consumption through all the subtests. The Cumulative patterns show increasing time consumption within subtests and from one subtest to the next. The Dissociative patterns show recurrently increasing and decreasing time consumption in all five subtests. The fourth pattern, the Cumulative-dissociative, shows increasing time consumption from the first subtest until the last, combined with intermittently increasing and decreasing time consumption in each subtest. More information on, and graphic illustrations of, the adaptive patterns have been given in detail [8, 13, 22].
Interpretation and association with myocardial infarction
In general, it can be said that Stabilized and Cumulative patterns are representations of normal adaptive behaviours, whereas disturbances in adaptive behaviour are represented by patterns with high variability (the Dissociative and the Cumulative-dissociative patterns of both the Regression and the Variability dimensions) [8].
The Variability dimension, used in this present study, has been associated with an increased incidence of MI in hypertensive men [13]. The patterns Stabilized and Cumulative have been called adaptive behaviour, a behaviour that was present in 207 men (50.7%). The Dissociative and Cumulative-dissociative patterns have here been called maladaptive behaviour. This behaviour was shown by 201 men (49.3%).
Ambulatory 24-h ECG recording
The manner in which the ambulatory electrocardiographic recordings over 24 h was performed and the instruments used have been presented in detail elsewhere [2] and therefore only a brief introduction of the definition of frequent and complex ventricular arrhythmia will be described below.
Ventricular arrhythmia
The cardiac arrhythmias were classified as a single ventricular extrasystole, bigeminy or trigeminy ventricular systole, couplets of ventricular extrasystoles, ventricular tachycardia and R-on-T ventricular extrasystole. The arrhythmias were grouped into the following categories according to the Lown classification [23]. Grade 0 showed no ectopic beats. Grade 1 showed < 720 ventricular extrasystoles over 24 h. Grade 2 was categorized at ≥ 720 ventricular extrasystoles per 24 h. Multiform ventricular extrasystoles or bigeminal or trigeminal ventricular extrasystoles were categorized as grade 3. Grade 4a was categorized when the ECG showed ventricular extrasystoles in couplets and grade 4b if ventricular tachycardia appeared. Grade 5 showed ventricular extrasystole of the R-on-T type. Lown grades 2 to 5 were used as a definition of frequent or complex arrhythmias.
Ischaemic heart disease
Prevalent ischaemic heart disease was defined as angina pectoris according to the Rose questionnaire [24] or if hospitalization had been recorded due to an MI.
Blood pressure and antihypertensive treatment
Blood pressure was measured with a sphygmomanometer after 15 min rest. The pressure was recorded to the closest 5 mmHg level and the arithmetic mean from three consecutive assessments was calculated. Blood pressure levels, systolic ≥ 160 mmHg and/or diastolic ≥ 95 mmHg, were used as a cut-off for elevated blood pressure [25]. The use of antihypertensive drug treatment was recorded if drugs, independent of type, to lower blood pressure had been prescribed. Beta-blocker therapy was the only drug-therapy that was separately recorded.
Diabetes mellitus
Registration of diabetes mellitus was made according to medical history, enzyme strips and oral glucose tolerance tests. Fasting blood glucose at ≥ 7.0 mmol/l was used as a definition [26].
Cholesterol and triglyceride levels
Plasma cholesterol and triglyceride levels were measured according to standardized procedures and expressed in mmol/l.
Tobacco and alcohol habits
Smoking was assessed by means of a structured questionnaire. The men were categorized into three groups: the first group consisted of men who had never smoked, the second of men who had quit smoking and maintained abstinence for at least 1 month prior to the examination, and the third group was made up of those who currently smoked. Alcohol habits were categorized according to amount consumed per week: < 250 g and ≥ 250 g.
Statistical analyses
Behaviour in the stressful encounter was divided into adaptive versus maladaptive behaviour in the Variability dimension of the serial CWT. Univariate associations between ventricular arrhythmia and incidence of MI and all-cause mortality was calculated using the Cox proportional hazards model. The Pearson chi-square and oneway ANOVA were used for comparison of the distribution of baseline risk factors when dividing the cohort into adaptive and maladaptive behaviour. Incidence rates per 1000 person-years of observation in MI, fatal MIs, all-cause mortality, and IHD-mortality were calculated in groups defined in terms of absence/presence of VA respectively adaptive/maladaptive behaviour.
Cox proportional hazards model was also used when applying multivariate analyses. In these analyses the risk of a future incidence of MI and all-cause mortality were calculated for each stratum in relation to other relevant cardiovascular risk factors. These factors were blood pressure level of systolic blood pressure (SBP) ≥ 160 and/or diastolic blood pressure (DBP) ≥ 95 mmHg, prevalent ischaemic heart disease, antihypertensive treatment, prevalent diabetes mellitus, plasma cholesterol and triglyceride levels and tobacco and alcohol habits. All covariates were entered simultaneously into the models and identical procedures were applied for both models. All confidence intervals were calculated at the 95% level.
Results
During follow-up, 98 men (24.0%) of the study cohort experienced an MI, 56 (13.2%) died in a diagnosis of IHD, and 128 (31.4%) from other causes. Frequent and complex ventricular arrhythmia was associated with an increased incidence of MI [unadjusted relative risk (RR) 1.93; 95% confidence interval (CI) 1.30 to 2.87] and all-cause mortality (unadjusted RR 1.40; 95% CI 1.05 to 1.88) during the approximately 14 years of follow-up (not in table).
Multivariate analyses
Behaviour and MI
In the absence of a maladaptive behaviour, VA was not associated with an increased incidence of MI (Table 1). Adjusted for presence of other cardiovascular risk factors the RR for men with VA together with a maladaptive behaviour pattern was 2.43 (95% CI 1.37 to 4.31). The event rate in that group was 37.0/1000 person-years. Thirteen of the 28 events (46.4%) were fatal. A fatal event was here defined as death on the same day as the MI.
Behaviour and mortality
VA was similarly in the absence of a maladaptive behaviour neither associated with any statistically significant increased incidence of deaths (RR 1.54; 95% CI 0.99 to 2.39) (Table 2). A maladaptive behaviour was in men with VA associated with an increased risk of death (RR 1.56; 95% CI 1.01 to 2.41).
Distribution of cardiovascular risk factors in men with adaptive and maladaptive behaviour
Baseline cardiovascular risk factors of the study cohort and distributed by adaptive and maladaptive behaviour in the Variability dimension are presented in Table 3. Presence of VA did not differ between men with adaptive or maladaptive behaviour patterns. The proportion of never smokers was the largest in men with an adaptive behaviour whereas men with a maladaptive behaviour had the largest proportion with a high consumption of alcohol.
Incidence rate of myocardial infarctions during follow-up in relation to presence of ventricular arrhythmias during 24-h ambulatory electrocardiographic recording and behaviour categorized according to the Variability dimension of the serial Color Word Test (Cox proportional hazards model) (n = 408). Figures in parentheses refer to fatal events
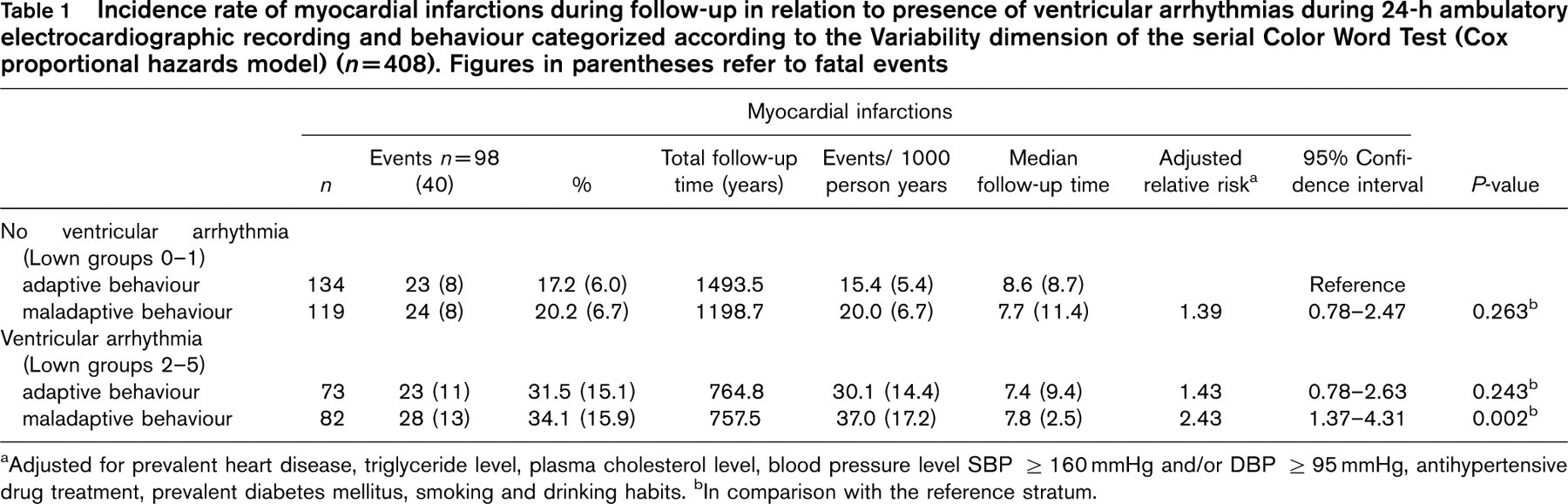
aAdjusted for prevalent heart disease, triglyceride level, plasma cholesterol level, blood pressure level SBP ≥ 160 mmHg and/or DBP ≥ 95 mmHg, antihypertensive drug treatment, prevalent diabetes mellitus, smoking and drinking habits. bIn comparison with the reference stratum.
All-cause mortality rate during follow-up in relation to behaviour categorized according to the Variability dimension of the serial Color Word Test and presence of ventricular arrhythmias during 24-h ambulatory electrocardiographic recording (Cox proportional hazards model) (n = 408). Figures in parentheses refer to ischaemic heart disease-related deaths
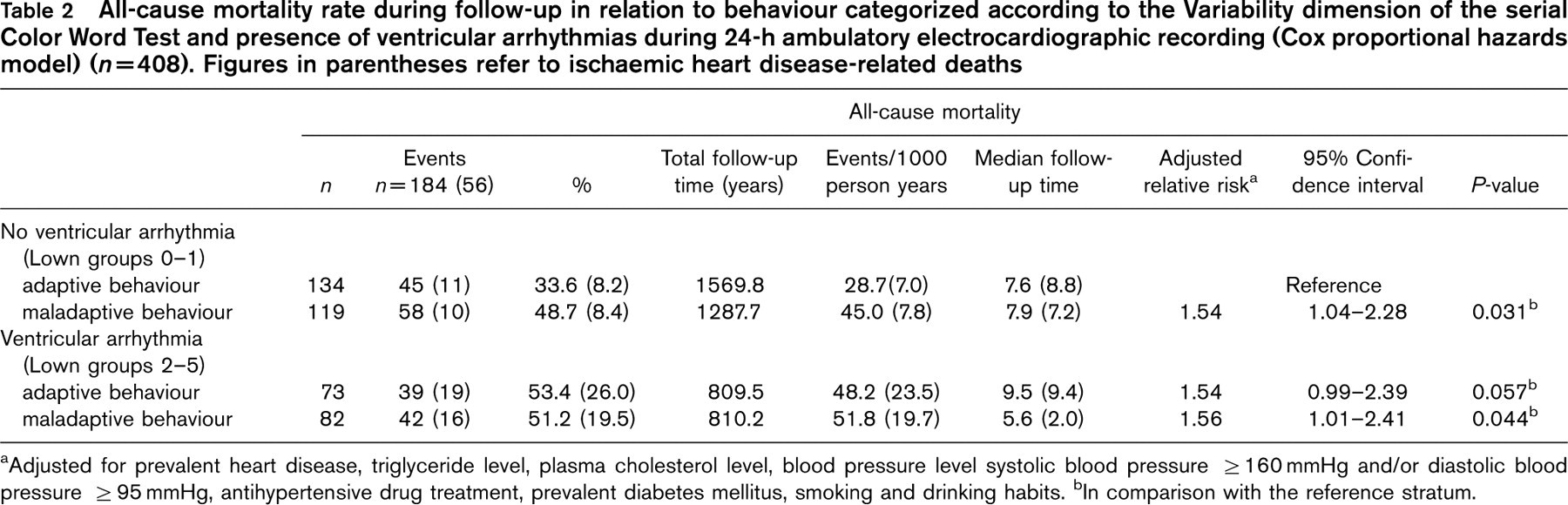
aAdjusted for prevalent heart disease, triglyceride level, plasma cholesterol level, blood pressure level systolic blood pressure > 160mmHg and/or diastolic blood pressure ≥ 95 mmHg, antihypertensive drug treatment, prevalent diabetes mellitus, smoking and drinking habits. bIn comparison with the reference stratum.
Baseline characteristics of study cohort distributed by adaptive and maladaptive behaviour categorized according to the Variability dimension of the serial Color Word Test (n = 408)
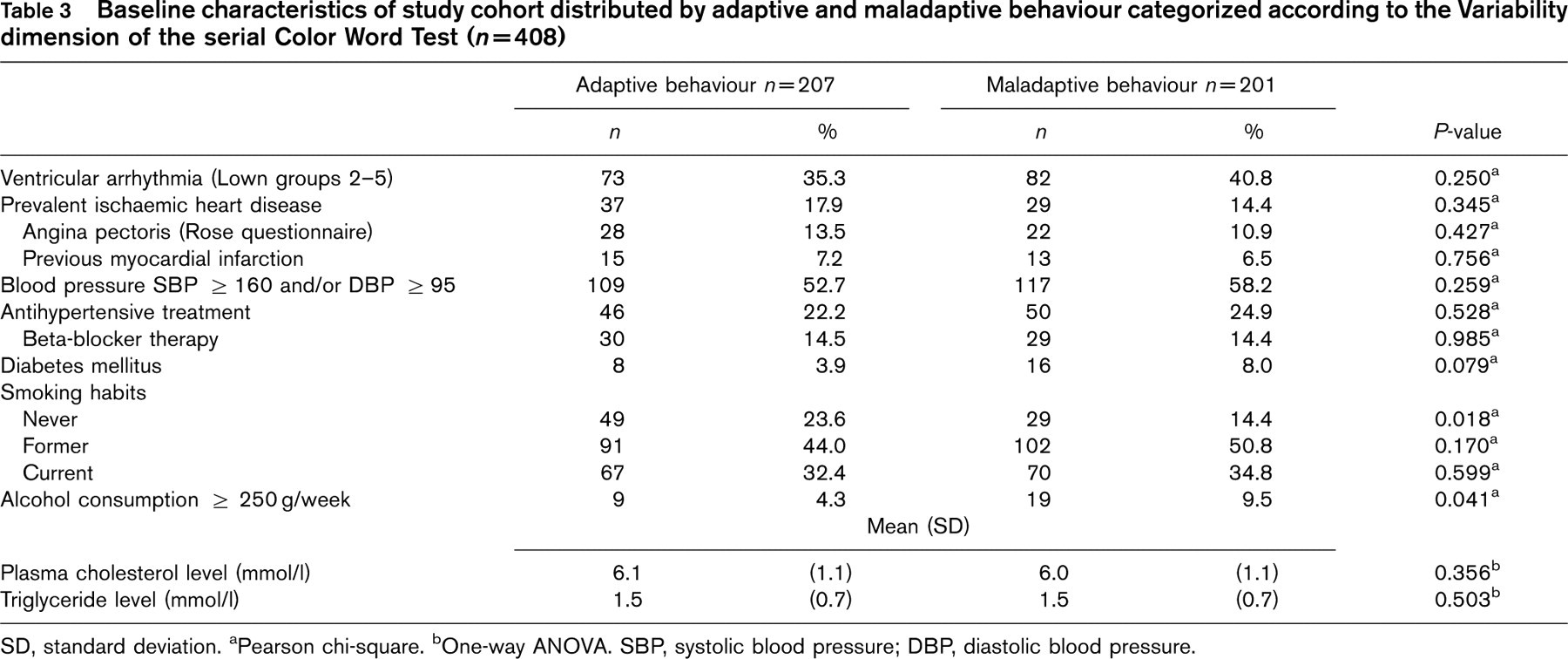
SD, standard deviation. aPearson chi-square. bOne-way ANOVA. SBP, systolic blood pressure; DBP, diastolic blood pressure.
Discussion
At baseline, 14 years prior to end of follow-up, there existed no statistically significant difference between men with adaptive and maladaptive behaviour patterns in the serial CWT regarding occurrence of frequent and complex ventricular arrhythmia during the 24-h Holter monitoring. However, during follow-up, differences in outcome could be established. This study shows that the increased incidence of MI and death in association with VA could only be observed in men with a maladaptive behaviour pattern. VA in the presence of an adaptive behaviour was not associated with an increased incidence of MI or death. These associations were independent of well-established cardiovascular risk factors, such as clinically prevalent heart disease, elevated blood pressure level or use of antihypertensive medication.
Stress is a subjective phenomenon, which is not uniformly defined, but when experienced the organism is forced to adapt to it. A potential stressor is identified as such in an initial phase, which by Lazarus has been called cognitive appraisal [27]. This phase determines how the individual will respond and may also explain differences in response patterns between individuals. Personality type, past experience of exposure to stress as well as the state of the individual's physical health [28] are examples of why individuals differ in their response to a stressful situation. Physiologic adaptation involves altered activity in the systems that are activated when reactions to stress take place. The most important systems in this context are the hypothalamic-pituitary-adrenocortical and sympathetic-adrenomedullary systems [28, 29]. Concurrent responses of the cardiovascular system in challenging situations are increased cardiac output and muscle blood supply, which in turn results in elevated pressure and increased heart rate [30]. Just as a response in a certain context is specific, so are the physiological correlates of the response. Active coping in a stressful encounter is associated with sympathetic nervous activity and catecholamine release but more passive behaviours are related to increased levels of corticosteroids [31]. Alterations of neurohormonal levels may in itself not be harmful but the threat to health rather consists of excessive, prolonged or inefficient responses of adjustment [28].
An association between cardiovascular reactivity (the manner in which the cardiovascular system responds to psychological stress) and stable personality traits has been proposed. This has been suggested because individuals differ in reactivity when exposed to a mental stressor [11, 32]. In a study on blood pressure responsiveness to psychological stress it could be shown that reinfarction or the incidence of stroke was higher among those postinfarction patients who showed the most obvious reactivity [33]. If measures of cardiovascular reactivity are aggravated across many tasks, laboratory as well as real-life situations, the links between enhanced reactivity and disease become even more obvious and support the position that cardiovascular reactivity is related to personality factors [34]. Cardiovascular reactivity has been associated with exaggerated blood pressure responses [35], carotid artery atherosclerosis and its progression [12], increased serum lipid concentrations, haemostatic factors and blood viscosity [36]. This increased cardiovascular reactivity may also act as a risk factor for the development of coronary artery disease [1].
The Stroop test is known to be both challenging and frustrating and by this serial application it was possible to distinguish two different types of behavioural response: adaptive and maladaptive. It is reasonable to believe that the maladaptive pattern, as defined in this study, is related to cardiovascular reactivity and that men with this behaviour are more prone to sudden elevations of blood pressure. The two adaptive patterns which make up the maladaptive behaviour, the Dissociative and the Cumulative-dissociative of the Variability dimension of the serial CWT, are also more frequent among psychosomatic patients than in healthy individuals [22]. In addition, the Cumulative-dissociative pattern of the Variability dimension has been related to high levels of tension [37].
The models by which acute stress could trigger a cardiac event in individuals diagnosed with coronary artery disease can briefly be outlined as follows [5, 6]. One model suggests that sympathetic activity influences endothelial function which results in a growth of vulnerable plaque. These plaques could rupture as a consequence of sudden elevations of blood pressure levels, which could have been provoked by stress-induced sympathetic activity. Other models concern platelet activation either through haemostatic changes or altered levels of haemoconcentration, which constitute a risk for coronary thrombosis. An additional model focuses on the potential of sympathetic activity to alter arrhythmic threshold, which could cause lethal arrhythmia as in the case with ventricular fibrillation. Psychological stress has been shown to increase dispersion of repolarization in patients with CAD but not in patients free of CAD [38].
In order to reduce the incidence of cardiac deaths, it is important to broaden the understanding of which individuals are at an increased risk and thereby identify them. Since the advent of the concept of the Type-A personality behaviour [39] and its possible association with the development of coronary heart disease, the links between psychosocial factors and coronary heart disease and death have been explored. A recent review of studies aimed at analysing the association between psychosocial factors and sudden cardiac death, ventricular arrhythmia and cardiac autonomic function concluded that surprisingly many studies reported findings confirming positive associations [1]. The studies reviewed had considered, for example, social position, life event stressors and in some instances recordings were made during simultaneous presence of a stressor. Population-based studies were, however, lacking and so were prospective studies where real life stressors had been examined in patient populations. The present study, which was population based, showed that a maladaptive behaviour pattern in a stressful situation interacted with VA in such a manner that the outcome was a worse prognosis regarding incidence of MI and death than it was for men who showed an adaptive behaviour.
The participants in this study were representative of a general male population, they were of the same age and came from an urban environment. The points of criticism, which can be raised against this study, still involve generalizability of results. To a considerable degree, lack of data in relevant variables circumscribed the study population. The participants were initially 500 men but in the present analyses data from only 408 men could be used. Lack of measures of cardiac function, as, for example, left ventricular hypertrophy, explains why such variables were not controlled.
The serial CWT has not been validated against any internationally well-known personality inventory. Its prognostic value in ‘Men born in 1914’ has, however, been shown in previous studies where the dimension Variability was associated with the incidence of a future cardiac event in hypertensive men [13] and the Regression with stroke incidence, also in hypertensive men [14]. In addition, the serial CWT has been validated against psychiatric syndromes and diagnoses in clinical settings [15], and it has discriminated between different psychosomatic disorders [22, 40] and between various groups with and without clinical symptoms [41]. The most consistent observation where the test has been used is that control individuals more often have been categorized as Stabilized of either dimension whereas more severe disturbances have been associated with Dissociative and Cumulative-dissociative patterns, likewise of either dimension. One must, however, bear in mind that the behaviours of this cohort of men are representations of behaviour within the ranges of normal psychology because the men constituted their own norm when behaviour was categorized [20].
The findings of the present study are consistent with a view that men with VA are at an increased risk of experiencing a future MI and premature death if stressful encounters are managed in a maladaptive manner. A maladaptive behaviour as defined in this study can generally be characterized by a failure to find a successful strategy in managing a stressful situation or solving a conflict. By the use of the serial CWT it was possible to show that there exist individuals who are more vulnerable than others to the damaging effects of stress. These individuals do not work methodically but instead try several strategies without allowing time for the strategy to prove itself. The serial CWT could be used to identify these men.
Footnotes
Acknowledgements
The authors are grateful to Professor Gudmund Smith, Department of Psychology, Lund University, for his support in preparation of this manuscript.