
Abstract
In very elderly participants of the Framingham Heart Study (mean age 79 years, 276 men and 462 women), interleukin-6 correlated with C-reactive protein (CRP) levels. Interleukin-6, tumour necrosis factor alpha and interleukin-1 production, and CRP were not associated with prevalent cardiovascular disease, and nonsteroidal anti-inflammatory drug use did not influence cytokine or CRP levels. Further studies are warranted to examine the prognostic implications of CRP and related cytokines for CVD in the elderly.
There is increasing interest in the role of systemic inflammation in promoting cardiovascular disease (CVD) in adults [1]. The evidence suggests that elevated markers of acute phase response may predict risk of CVD. Further, the anti-inflammatory agent aspirin is effective in reducing the risk of initial and recurrent CVD associated with a persistent acute phase response [1, 2]. However, data are sparse regarding the association of inflammation with risk for CVD in very elderly persons, who comprise a rapidly growing segment of the population.
We examined the association of systemic inflammation and cytokine production by peripheral blood mononuclear cells (PBMC) with prevalent CVD and interactions with nonsteroidal anti-inflammatory drug (NSAID) use in a population-based cohort of very elderly men and women. Serum C-reactive protein (CRP), serum interleukin-6 (IL6), and production of tumour necrosis factor alpha (TNF) and interleukin-1 (IL1) by PBMC, were determined in 276 men and 462 women (mean age 79 years) in the Framingham Heart Study. The Framingham Heart Study methods have been previously described [3]. The study subjects were participants in a study of ageing and inflammation during 1988–1992 [3] and were ambulatory and free of hepatic or renal disease. CRP was measured by immunoprecipitation assay (Incstar Corp., Stillwater, MN, USA) and IL6, IL1 and TNF by specific radioimmunoassays [3]. CVD was defined as prevalent coronary heart disease (CHD), stroke or intermittent claudication confirmed by a review of a physician endpoint committee.
Clinical characteristics of the study population are presented in Table 1. There were 246 (33%) subjects with prevalent CVD, CHD in 158, stroke in 81 and intermittent claudication in 81, and 49% of subjects were taking a NSAID. IL-6 production was positively associated with CRP (r = 0.10, P = 0.011). Levels of IL-6, TNF and IL-1 were not associated with CVD (table). In multiple logistic regression analysis comparing the highest quartile with other quartiles of TNF levels, there were modest increases in risk of CVD (OR 1.39, 95% CI 0.96–2.02, P=0.08) and CHD (OR 1.22, 95% CI 0.80–1.86, P = 0.36) of borderline significance, but there were no significant associations with IL-6 or IL-1. CRP was not associated with prevalent CVD or with the individual endpoints CHD, stroke or intermittent claudication. The results of these analyses were not altered when stratified by NSAID use (Table 2).
Clinical characteristics of the study population
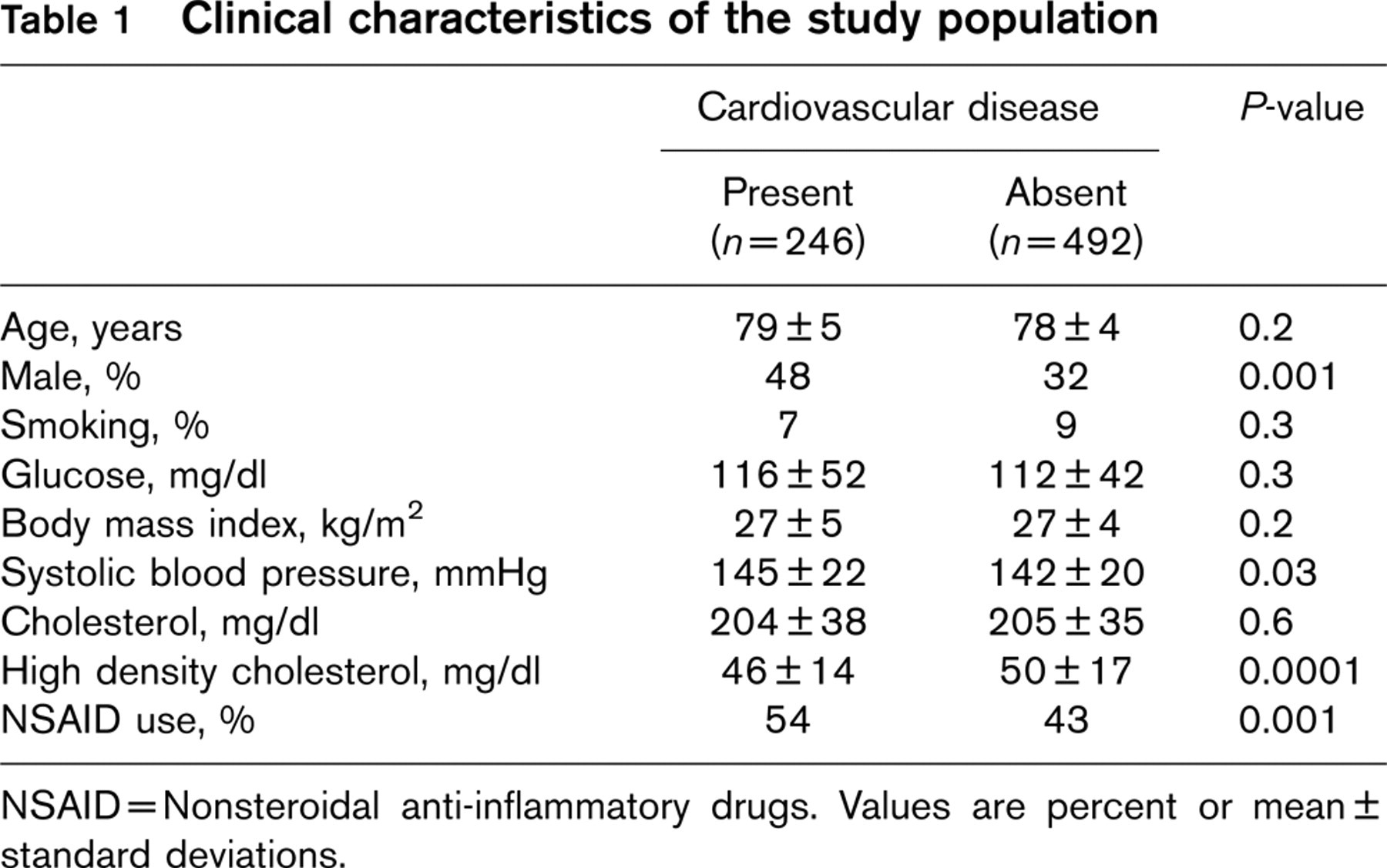
NSAID = Nonsteroidal anti-inflammatory drugs. Values are percent or mean ± standard deviations.
Our study is among the first to examine associations of serum IL-6, PBMC-production of TNF and IL-1, as well as CRP, with prevalent cardiovascular disease in a free-living elderly population. We were unable to detect an association of CRP with CVD, and NSAID use did not influence cytokine or CRP levels. A raised concentration of CRP is a prognostic indicator of subsequent events in persons with prior CVD or multiple risk factors, in the elderly and in healthy male physicians [1, 2, 4, 5]. These findings with CRP, a nonspecific inflammatory marker, have stimulated the hypothesis that cytokines, adhesion molecules or chemokines might be the specific mediators of the underlying inflammatory condition that increases risk for CVD. While we did not find associations with CRP in our very elderly cohort, it is possible that this in part is due to use of the less sensitive CRP assay. However, we also did not observe any significant association of a range of putative cytokines with CVD in our very elderly subjects.
Since our study is cross-sectional, further studies are warranted prospectively to examine the associations of CRP and related cytokines with incident CVD. However, several hypothesized explanations for an absence of association may serve as the focus for future investigations. For one, ex-vivo cytokine production may not reflect in-vivo levels [6]. However, a number of studies have shown that ex-vivo IL-1 production correlates with in-vivo levels and with other markers of inflammation [7]. Alternatively, although our subjects were ambulatory and they were free of clinically overt inflammatory conditions, it is possible that in older subjects there is a higher prevalence of subclinical inflammatory degenerative disorders which may dilute associations with CVD. Finally, if atherosclerosis itself causes inflammation, our observations would be consistent with the hypothesis that CRP and inflammatory cytokines may simply be markers of the burden of subclinical atherosclerotic disease, which may be high in elderly survivors without as well as with clinically apparent CVD. Thus, CRP and related cytokines would tend to lose predictive value in the very elderly.
Cytokine distribution in the study population
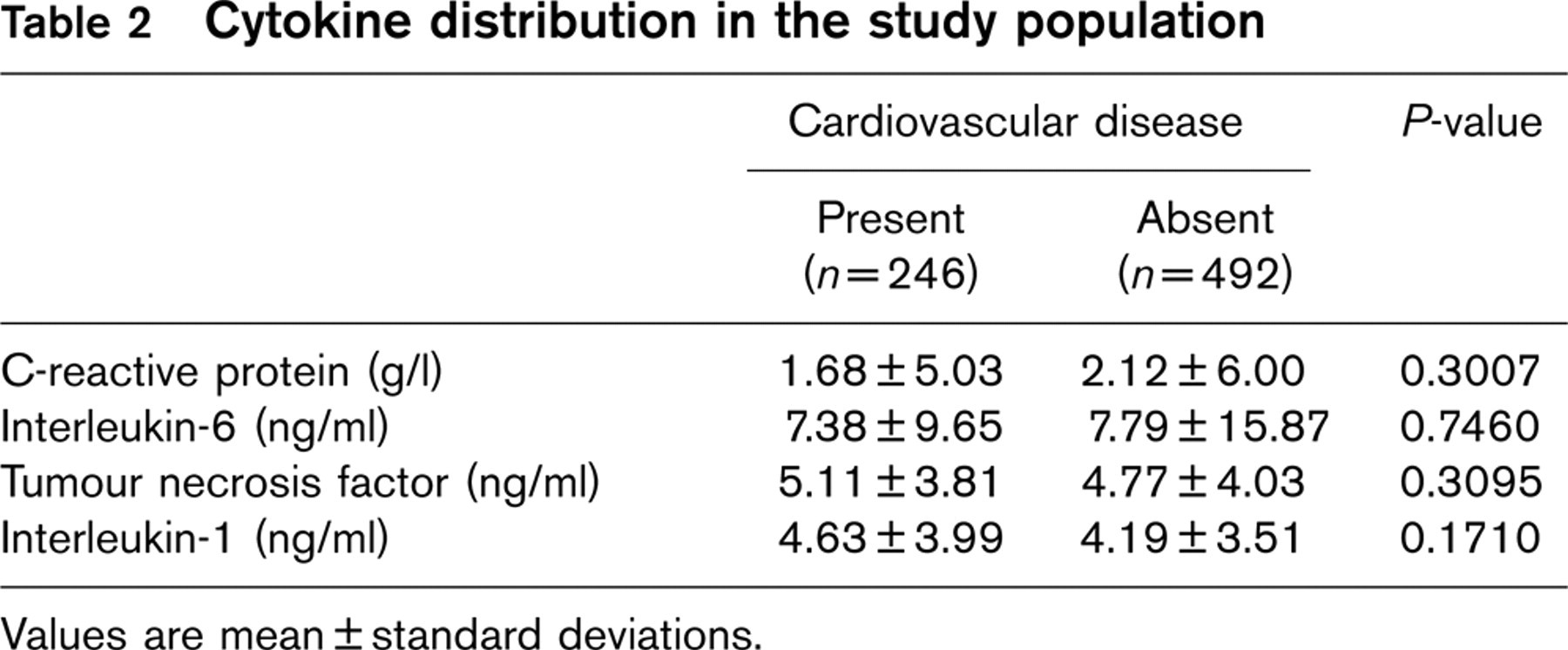
Values are mean ± standard deviations.
In this well characterized, very elderly population cohort, IL-6 correlated with CRP levels. However, IL-6, TNF and IL-1 production was not associated with cardiovascular disease, and NSAID use did not influence cytokine or CRP levels. Further studies are warranted to examine the prognostic implications of CRP and related cytokines for CVD in the elderly.