
Abstract
Objectives
We explored the effects of regular consumption of wheat fibre in patients with dysmetabolic cardiovascular syndrome (MCVS).
Subjects and methods
Forty-two patients with MCVS (mean age 49 ± 8 years) were randomly assigned to a treated group (n = 21) or to a control group (n=21). Patients in the treated group ate 10.5 g of wheat fibre powder per day for the first week, followed by 21 g per day for the next 4 weeks. A standard high-fibre diet was recommended to both groups. Blood pressure, metabolic parameters, fibrinolytic parameters and factor VII activity were measured at entry and after 5 and 9 weeks.
Results
After completing treatment, patients from both groups lost an average of 1 kg weight. Consumption of wheat fibre resulted in a significant (P<0.05) decrease of systolic and diastolic blood pressure, fasting glucose, glucose 2 h after oral glucose challenge (OGC), total cholesterol, low-density and high-density lipoprotein cholesterol, ranging from 7 to 18%. Furthermore, no significant reductions in fasting insulin, insulin 1 and 2 h after OGC, and glucose 1 h after OGC were found, whereas no differences in fibrinolytic parameters and factor VII activity were observed. Almost all beneficial effects of wheat fibre diminished 4 weeks after its withdrawal. In the non-treated group only a significant decrease of systolic pressure was observed.
Conclusions
Our results suggest that supplementation of wheat fibre, not just a standard high-fibre diet, may improve cardiovascular risk profile in patients with MCVS, in a manner independent of weight reduction. Eur J Cardiovasc Prevention Rehab 11:144–148 © 2004 The European Society of Cardiology.
Introduction
Dysmetabolic cardiovascular syndrome (MCVS) is characterized by the presence of four typical metabolic risk factors (obesity, impaired glucose tolerance, dyslipidaemia and arterial hypertension) [1]. Typically the obesity is of the abdominal type with increased waist to hip ratio. MCVS is commonly accompanied by impairment of the fibrinolytic system, presented as an elevation of plasminogen activator inhibitor type 1 (PAI-1). The estimated incidence of MCVS is 20–25% in the adult population, while in some older groups MCVS prevalence approaches 50% [2, 3]. MCVS significantly increases the risk of coronary artery disease and patients with MCVS are at increased risk of developing type 2 diabetes [4–6]. Insulin resistance is thought to be central to the metabolic abnormalities in MCVS [1]. Current pharmacological treatment of patients with MCVS is focused on treatment of arterial hypertension and dyslipidaemia, whereas non-pharmacological approaches try to decrease the weight, and consequently insulin resistance, by diet and regular exercise. Insulin resistance might be directly improved by metformin. Doubts concerning metformin efficacy will be resolved by ongoing studies [7]. Insulin resistance and consequent metabolic profile could be, at least theoretically, improved by dietary fibre, but this prediction, which might be clinically relevant, has not been completely investigated.
It is known from epidemiological studies that dietary fibre of foods rich in fibre, especially from cereal products, may protect against coronary heart disease and stroke [8–10]. A high intake of dietary fibre improves glycaemic control, decreases hyperinsulinaemia, and lowers plasma lipid concentrations in patients with type 2 diabetes [11–13]. A high-fibre, high-carbohydrate, low-fat diet has been recommended for a long time to patients with MCVS in order to delay the development of diabetes and coronary heart disease, although substantiating proof has been missing. It was first suggested [14, 15], and recently proved, that changes in lifestyle, including high-fibre diet and regular exercise, could delay the onset of type 2 diabetes in subjects with impaired glucose tolerance [16]. However, the effects of diet and exercise were not separated, and the effect of weight reduction could not be separated from the isolated effect of high-fibre diet. Thus, it remains to be established whether fibre can independently (from weight reduction) affect insulin resistance. In the present study we explored weight loss-independent effects of supplementation with wheat fibre in patients with MCVS.
Patients and methods
Patients
Forty-two patients (31 male and 11 female; mean age 49 ± 8 years) who fulfilled the criteria for MCVS were enrolled in the study. The following criteria [1] were used: hyperlipidaemia (low-density lipoprotein cholesterol 4.0 to 6.0 mmol/l or triglycerides 2.3 to 6.0 mmol/l or high-density lipoprotein < 0.9 mmol/l for male and < 1.2 mmol/l for female), obesity [body mass index (BMI) > 27.0 kg/m2 with waist to hip ratio > 0.95 for male and > 0.80 for female], fasting plasma glucose > 6.1 mmol/l or disturbed glucose tolerance test, and arterial hypertension (blood pressure > 140/90 mmHg or treated hypertension). The conclusion that a patient had MCVS depended on exhibiting three out of four criteria. Patients with definite diabetes and patients who used thiazide diuretics or beta-blockers were not included. Patients with manifest coronary (angina pectoris, myocardial infarction or coronary revascularization), carotid (carotid artery stenosis) or peripheral arterial disease (intermittent claudication, amputation due to ischaemia) were not included. The rationale for that criterion was to recruit the patients at an early stage of MCVS, in whom diet intervention, at least in theory, should be the most beneficial. Patients were recruited from a group of highly motivated relatives of other patients with more severe metabolic abnormalities and present manifest atherosclerotic disease. Patients continued to use their medications (statins: 10 patients, fibrates: six patients, angiotensin-converting enzyme inhibitors: 10 patients, calcium antagonists: five patients) in an unchanged manner. Selected patients were randomly assigned to either treated or non-treated groups. The groups did not differ in initial values of any of the measured parameters. A high fibre, high-carbohydrate, low-fat diet was recommended to all patients and explained by a dietitian nurse.
Patients in the treated group ate 10.5 g of wheat fibre powder (Trifyba; Tricum AB, Höganäs, Sweden) per day for the first week, followed by 21 g per day for the next 4 weeks. The dosages of 10.5 and 21 g were chosen; these were the package size of the producer. They estimated that a 21 g dosage is the optimum dosage, which allows the greatest benefit in conjunction with the lowest degree of side effects. A double-blind study could not be performed since the appropriate neutral placebo was not available. Fibre was taken on the basis of the patient's decision; some patients ate fibre all together (mainly during breakfast), others ate it a little at a time during other meals. Blood samples were taken and blood pressure were measured in both groups before starting treatment with wheat fibre, after completing treatment (after 5 weeks) and 4 weeks thereafter. An experienced nurse who was blind to randomization measured the blood pressure. At the first and second admissions an oral glucose tolerance test was performed on all patients.
Blood sampling and laboratory methods
Blood samples were drawn from the antecubital vein between 0700 and 0900 h with minimal venous stasis. Patients ate no fibre or any food 12 h before measurements. Patients were rested, prior to blood sampling, for 20 min in a sedentary position. Plasma was prepared by centrifugation for 30 min at 2000 g and 4°C, snap frozen in liquid nitrogen and stored at −70°C until analysed. The metabolic variables [glucose, total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides] were determined by routine biochemical methods. The serum insulin concentration was measured by a radioimmunoassay (Sorin Biomedica, Italy). Tissue plasminogen activator (t-PA) and PAI-1 antigens were determined by enzyme-linked immunosorbent assay (ImulyseTM tPA and ImulyseTM PAI-1, respectively, both from Biopool, Sweden), whereas t-PA activity and PAI-1 activity were determined by amidolytic assays (Spectrolyse®/fibrin, Biopool, Town, Sweden). Fibrinogen was determined by a clotting assay (Multifibren; Behring, Town, Germany). Activity of factor VII was determined by spectrophotometry (Chromotimer; Behringwerke AG, Marburg/Lahn, Germany).
Normals for measured parameters were as follows: blood pressure (≤140/90 mmHg, total cholesterol (≤5 mmol/l), LDL cholesterol (≤3 mmol/l), HDL cholesterol (≥1 mmol/l), triglycerides (≤2 mmol/l), fasting glucose (≤6.1 mmol/l), glucose 2 h after oral glucose challenge (OGC) (≤8 mmol/l). Values of fibrinolytic parameters and factor VII activity in our population were previously determined. Normals for the age-matched population were: t-PA antigen: 3.0–10.0 ng/ml, t-PA activity: 0.2–2.0 IU/ml, PAI-1 antigen: 3.5–47.5 ng/ml, PAI activity: 0.0–15.0 IU/ml, plasminogen: 0.75–1.50 (relative activity), fibrinogen: 1.9–3.8 g/l, factor VII activity: 0.60–1.60 (relative activity).
Statistical methods
Distribution of variables was tested by the Kolmogorov-Smirnov test. Normally distributed variables were expressed as means and standard deviation, and compared by the t-test for independent samples. Continuous variables which were not distributed normally were expressed as medians with ranges between the first and third quartile, and differences between groups were assessed by the Mann-Whitney U-test. An analysis of variance was performed by two-way mixed ANOVA. Statistical analyses were performed by the Statistica for Windows computer program (Stat Soft, Inc., Tulsa, Oklahoma, USA). A P-value of < 0.05 was taken as statistically significant.
Results
Three patients stopped the study prematurely in the treated group due to self-reported occasional abdominal pain and discomfort attributed to fibre intake. Compliance of patients was checked by interview; in addition, patients returned unused fibre. It was estimated that the patients who finished the study used at least 88% of the prescribed amount of fibre.
Weight and blood pressure
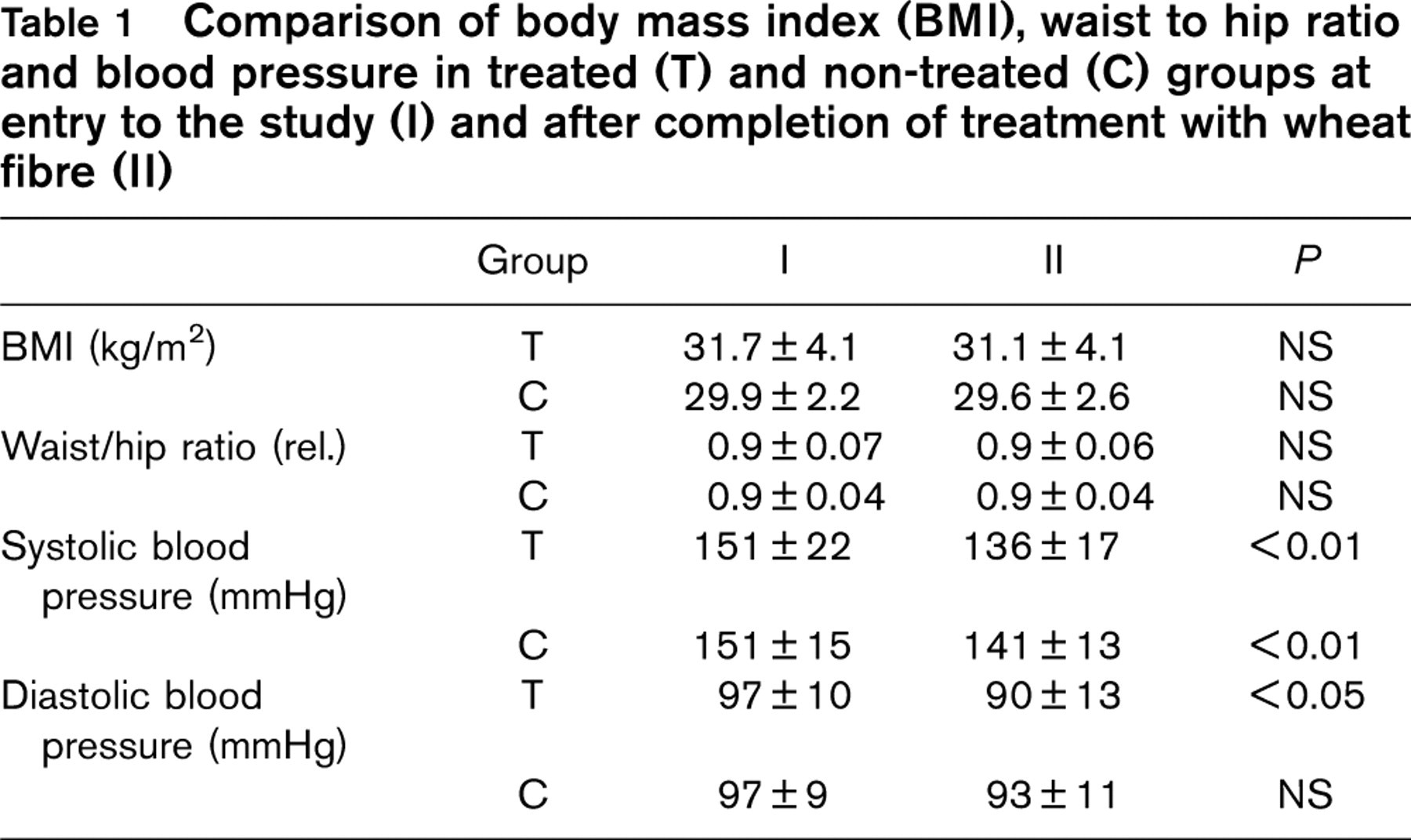
After 5 weeks of treatment the patients in both groups lost an average of 1 kg. There was no difference between the groups. BMI and waist-to-hip ratio did not change significantly in either group (Table 1). Initial waist-to-hip ratio was 0.85 ± 0.07 and 0.95 ± 0.05 for female and male, respectively. After 4 weeks of observation post-treatment, patients did not regain weight. Systolic and diastolic pressures are presented in Table 1. A significant decrease of systolic pressure was observed in both groups, whereas only in the treated group did diastolic pressure also decline. However, the difference between systolic and diastolic pressure of the two groups was not significant. In the treated group, an average decrease of 10 and 7% was observed for systolic and diastolic pressure, respectively. At 4 weeks post-treatment, systolic blood pressure in the treated group was still significantly decreased (134 ± 16 mmHg), whereas diastolic pressure was moderately increased (93 ± 10 mmHg) and not significantly different from pre-treatment values.
Comparison of body mass index (BMI), waist to hip ratio and blood pressure in treated (T) and non-treated (C) groups at entry to the study (I) and after completion of treatment with wheat fibre (II)
Glucose and insulin
Fasting glucose, glucose 1 and 2 h after oral glucose challenge (OGC), fasting insulin and insulin 1 and 2 h after OGC are presented in Table 2. Fasting glucose and glucose 2 h after OGC significantly decreased in the treated group (by an average 8%), and there was also a borderline significant reduction of glucose 1h after OGC as well as fasting insulin and insulin 1 and 2 h after OGC. Four weeks after the end of treatment fasting glucose and insulin reached pre-treatment levels (Table 2). In regard to non-significant decrease of insulin, it is informative to calculate the sample size of the treatment group necessary to obtain a significant paired samples t-test at an alpha level of 5% and 80% power given the observed distributions. For fasting insulin, the required sample size is 88, while for insulin 2 h after OGC, 42 subjects would have been required. In the non-treated group no significant changes or similar trends in the decrease in glucose and insulin levels were observed.
Lipids
Values of total cholesterol, LDL and HDL cholesterol and triglycerides are shown in Table 3. In the treated group significant decreases of total cholesterol, LDL and HDL cholesterol were found (14, 18 and 9% for total, LDL and HDL cholesterol, respectively), whereas triglycerides remained unchanged. No significant changes were observed in the non-treated group. Four weeks after treatment, total cholesterol, LDL and HDL cholesterol had increased to pre-treatment values (Table 3).
Fibrinolytic parameters and factor VII activity
No significant changes in fibrinolytic parameters (t-PA antigen and activity, PAI-1 antigen and activity, plasminogen and fibrinogen) or factor VII activity were found in either treated or non-treated groups (Table 4).
We also performed analysis of variance (two-way mixed ANOVA with group as the between-subjects factor and time as the within-subject factor) for those parameters significant with the t-test (systolic blood pressure, diastolic blood pressure, total cholesterol, LDL cholesterol, HDL cholesterol, fasting glucose and glucose 2 h after OGC). For all outcomes, with the exception of LDL cholesterol, the interaction effect was statistically significant (P < 0.05), which additionally confirms the findings.
Discussion
The aim of our study was to explore the possibly favourable effects of regular supplementation with wheat fibre on cardiovascular risk profile in patients with MCVS. It is not clear if fibre itself (in diet or supplemented) could, independently of weight reduction, influence metabolic risk factors in MCVS patients. We explored these topics by using diet with and without supplementation with moderate amounts of wheat fibre. Wheat fibre was selected since it is known that it is relatively well tolerated by patients. In addition, an important protective role of wheat fibre has been already recognized, namely, that it significantly protects against colon cancer [17].
Comparison of glucose and insulin levels in treated (T) and non-treated (C) groups at entry to the study (I) and after completion of treatment with wheat fibre (II), and four weeks later (III)
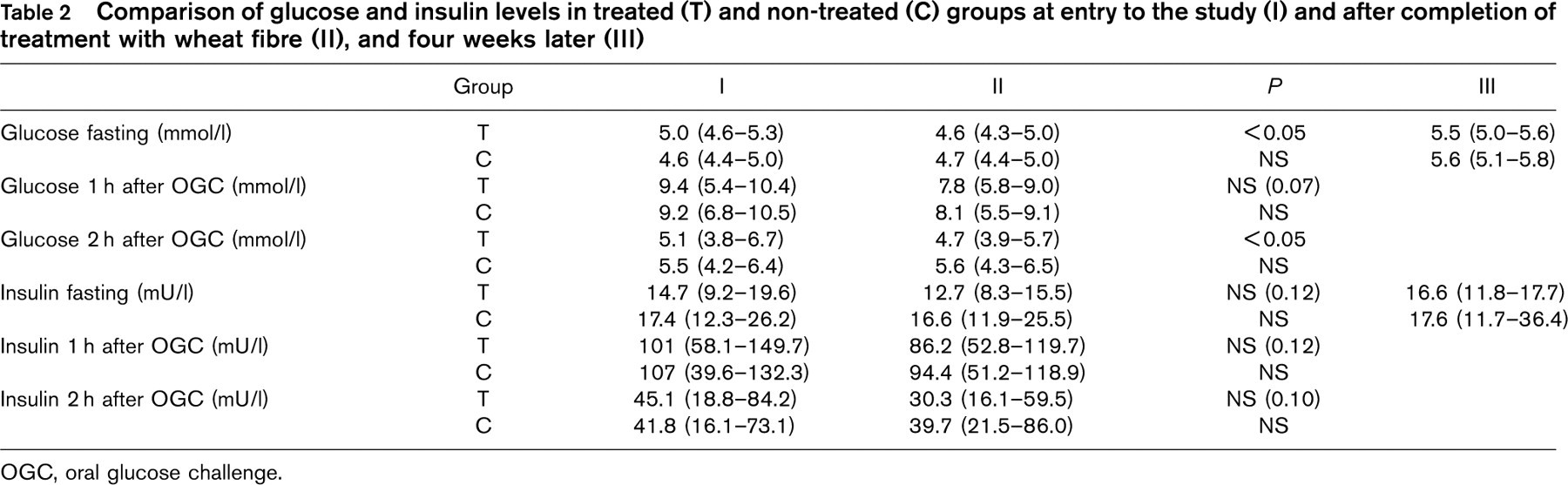
OGC, oral glucose challenge.
Comparison of lipids in treated (T) and non-treated (C) groups at entry to the study (I) and after completion of treatment with wheat fibre (II), and four weeks later (III)
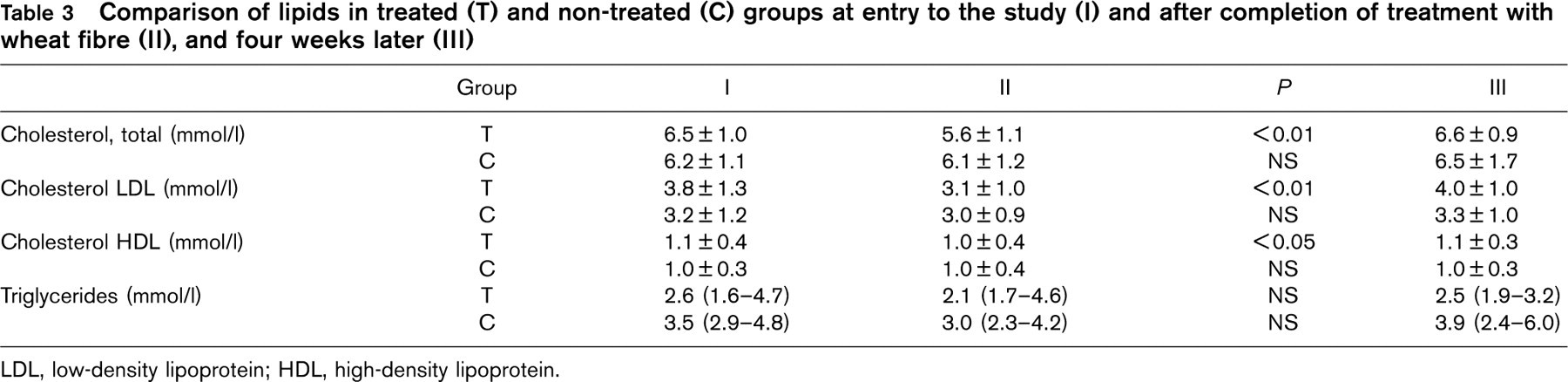
LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Comparison of fibrinolytic parameters and factor VII activity in treated (T) and non-treated (C) groups at entry to the study (I) and after completion of treatment with wheat fibre (II)
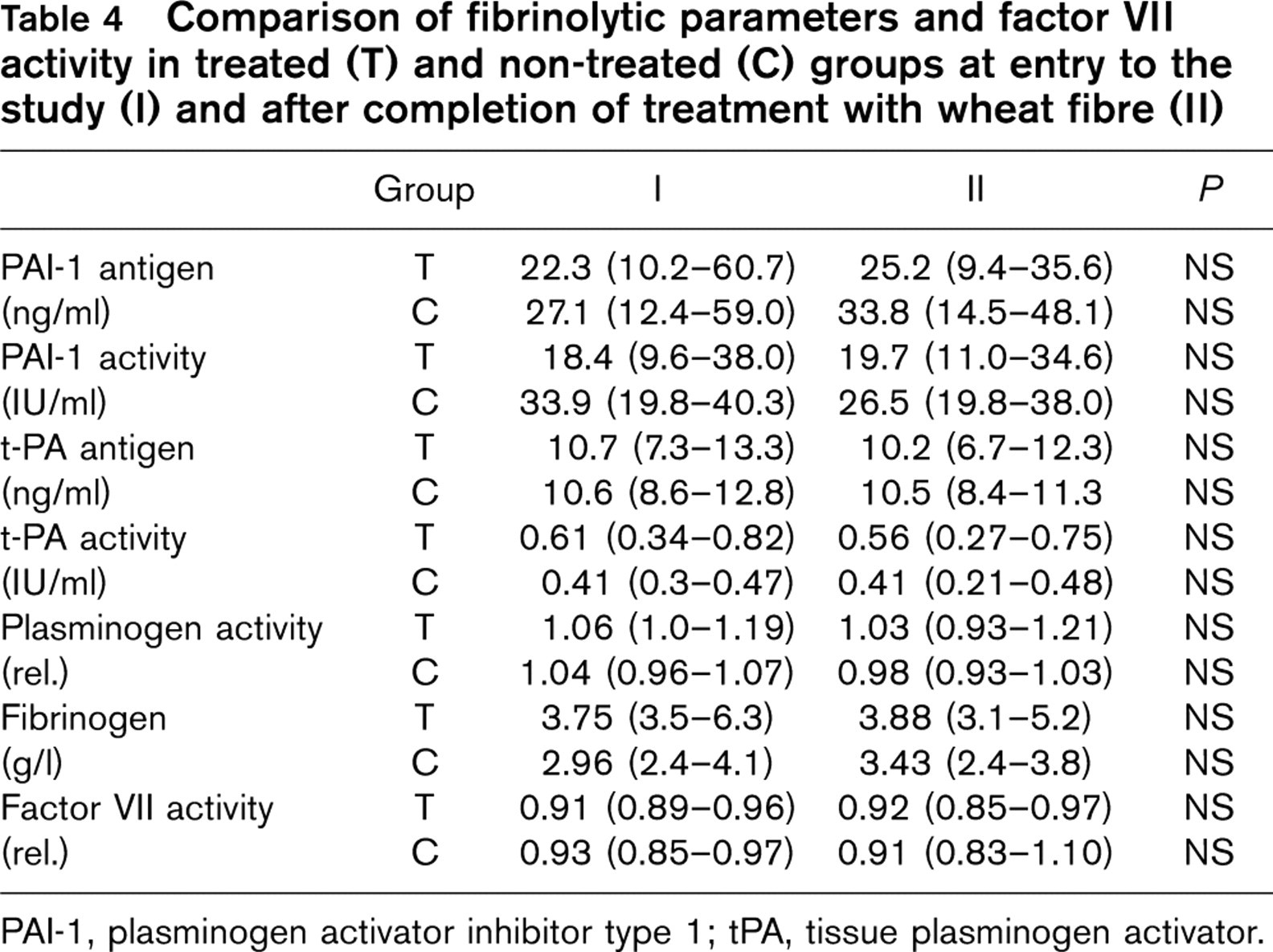
PAI-1, plasminogen activator inhibitor type 1; tPA, tissue plasminogen activator.
We found that regular intake of moderate amounts of wheat fibre (10.5 g of wheat fibre powder per day for the first week, followed by 21 g per day for the next 4 weeks) resulted in a convincing improvement of risk profile in patients with MCVS. Significant decreases of both systolic and diastolic pressure, total cholesterol, LDL and HDL cholesterol, fasting glucose and glucose 2 h after OGC were observed, accompanied by non-significant decreases of fasting insulin and insulin after OGC. The effect on risk factors was mild to moderate, the average decrease of glucose, blood pressure and lipids being in the range of 7 to 18%. The fibre had no significant effect on fibrinolytic parameters or factor VII activity. It is important to emphasize that toleration of wheat fibre was good, with high compliance with treatment.
The mechanisms underlying the observed beneficial effects are not clear. They could be attributed to the recommended diet and/or reduction of weight. However, since a similar diet was followed by the control group and since patients recruited to the non-treated group underwent a similar, minor loss of weight (an average 1 kg), this possibility is ruled out. This is further confirmed by the fact that all beneficial effects disappeared 4 weeks after the end of treatment (despite the patients not regaining the lost weight). Since the beneficial effect was not observed in the non-treated group (patients who consumed only the recommended diet) our results further suggest that a standard high-fibre diet without additional supplementation of fibre is insufficient to achieve optimal favourable metabolic effects in patients with MCVS. It seems likely that patients with insulin resistance demand higher amounts of fibre than subjects without insulin resistance. Whether patients with type 2 diabetes demand even higher amounts of fibre to achieve maximal metabolic benefit (thereby confirming the dose–response relation between fibre and effect) remains unanswered.
The most likely mechanisms for metabolic improvement with wheat fibre include delay of glucose absorption, increased insulin sensitivity at the cellular level, and increase in hepatic extraction of insulin. The lower insulin levels (during treatment with wheat fibre we found not significant decreases in fasting and after OGC insulin levels, which would very likely be significant in a larger sample of patients) have favourable metabolic effects. Insulin could directly produce an increase in lipids by activation of lipase in adipose tissue [18], increase blood pressure by influencing endothelial vasoconstrictor/vasodilator properties of arterial endothelium and by increased synthesis of angiotensin II (with consequent increase in peripheral resistance) [19, 20], and increase PAI-1 production by activation of its synthesis by elevated levels of angiotensin II [18].
In conclusion, while the mechanism underlying the observed mild to moderate improved risk profile observed in patients with MCVS treated with wheat fibre remains uncertain, it appears to be independent of weight reduction and to demand the additional supplementation of fibre, and not just a high-fibre diet.
Footnotes
Acknowledgements
We are grateful for statistical advice to Prof. Janez Stare, PhD and Gaj Vidmar, PhD, of the Institute of Biomedical Informatics, Medical Faculty, University of Ljubljana.