
Abstract
Study objective
Environmental-factor changes may largely be accountable for the dramatic increase of obesity prevalence in industrialized countries. This study investigated the relationships between body mass index (BMI) and various socioeconomic, clinical, behavioural and reproductive factors in a population from Southern France.
Methods
Using a cross-sectional study, a sample of 3127 current and former salaried workers (1658 men and 1469 women) completed a questionnaire on personal and medical histories, and had a clinical examination including height and weight measurements. Age-adjusted and multiple linear regression analyses were performed.
Results
The overall prevalence of obesity (BMI ≤ 30kg/m2) was 9.8% and was higher in men than in women (11.1 versus 8.3%). Multivariate analyses showed that in both sexes, low educational level, television watching, low physical activity and ex-smoking habits, were independently associated with a higher BMI. Furthermore, in women, we found independent and positive associations between BMI and the number of naps per week, short sleep duration, daily alcohol consumption, the number of pregnancies, early age at menarche or the non-use of oral contraceptives.
Conclusions
Our results reveal the complexity that exists between BMI and environmental factors and stress the need to analyse and to handle these factors simultaneously.
Introduction
Data originating from the USA and European countries suggest that obesity prevalence has increased to such an extent over the past 20 years that it should be now qualified as a pandemic [1, 2]. Obesity and weight gain are both associated with increased morbidity and mortality [3], and are highly and independently responsible for several chronic diseases, including coronary artery disease, diabetes mellitus, hypertension and some types of cancers [4]. The conjunction of high fat intake, sedentary lifestyle [5, 6] and changes in the quality of life plays a determining role [7]. The identification of body mass or mass gain related factors is essential to improve public health policy [2, 8]. The dramatic increase of obesity and overweight prevalence during these past few years, in developed countries and in populations from genetically different origins seem to imply that environmental factors, individual and collective behavioural changes may largely be accountable for such a trend.
Many studies have investigated the relationships between body mass and sex, age [9, 10], socio-economic status [11, 12] and several environmental factors, such as smoking [13, 14], television watching [15–18], alcohol consumption [19–21], sleep duration [18] and in women, parity [22], the number of pregnancies [23] and the age at menarche [24, 25]. However, only very few studies were able to analyse all these characteristics simultaneously.
The aim of this study was to analyse the relationship between body mass index (BMI) and various socio-economic, clinical and behavioural factors in a population from Southern Europe.
Methods
Population sampling
The participants were recruited in the first cross-sectional study of the prospective VISAT study [26], conducted in 1996. Among the 4258 current and former salaried workers who were recruited, 3236 subjects agreed to participate in the study (participation rate 76%). The sample comprised 1660 men and 1576 women, aged 62, 52, 42 or 32 years when elected. Globally, the participation rates were equally distributed in each stratum. Subjects were drawn from occupational physicians' lists of patients in three Southern French regions (Midi-Pyrénées, Aquitaine, Languedoc Roussillon). These lists include all the salaried workers since in France all the firms have a legal obligation to have their employees registered in occupational medical services. In case of a subject's refusal or unavailability, the following subject on the list, complying with the required criteria (age and sex), was selected. Physicians were volunteers and specifically trained by the research team. A written protocol, specifying the various stages of the study, the questionnaire administration and the measurement techniques, was distributed to each investigator.
Data were collected during the yearly compulsory medical examination, a component of the legal health screening in French companies. Retired workers in the 62-year old group were specially requested to participate in the study and were screened by the occupational physician employed by the company for which they had worked. All the subjects participating in the study were volunteers. Authorization from the appropriate ethics committee was obtained.
Personal and medical history
The medical investigators administered questionnaires concerning the participants' past and present medical histories. A self-administered questionnaire was also completed regarding the participants' social, family and occupational status and on their way of life. All the socioprofessional salaried working classes (French nomenclature) were represented: executives, technicians, supervisors, white- and blue-collar workers. Workers were categorized according to their current occupation and retired subjects were categorized according to their last occupation.
Sleep duration was quantitatively assessed as follows: the period between the beginning of the sleeping phase and the waking-up time. This sleep duration did not include afternoon naps, and they have been reported separately. A binary variable ‘sleeping time' (≤ 6 h/day versus > 6 h/day) was created because of the lack of significant difference in the BMI when the sleeping period exceeded 6 h. A similar method was applied to the number of naps per week (< once/day versus ≤ once/day). Leisure-time physical exercise level and TV watching were assessed as follows: number who exercised less than twice a week versus those who exercised twice a week or more and number who watched TV for less than 1 h/day versus those who watched for 1 h/day or more. Educational level (determined by the number of years of schooling), number of pregnancies and age at menarche were considered as categorical variables. Menopause was defined as follows: amenorrhoea ≤ one-year duration or bilateral ovariectomy.
Clinical measurements
The medical examination included height, weight, blood pressure and heart rate measurements. Height and weight were measured according to a standardized protocol. Weight was measured using digital scales. Height was measured in a standing position, without the shoes, using a flexible non-extendable tape. Body mass index was calculated as follows: [weight (kg)/ (height (m))2].
Data analysis
Data were analysed separately for men and women. Statistical analyses were performed using the STATA statistical software release 6. One-way analysis of variance was used to test the statistical significance between the classes of categorical variables. Age-adjusted comparisons were processed using an analysis of covariance. Associations between the BMI and independent variables were assessed in a backward linear regression analysis. The significance level for removing variables was P ≤ 0.10. In order to minimize possible confusion due to differences between the various types of hormonal contraceptive composition, we performed separate multivariate analyses for the 431 women in the 32-year old group. Tests for trend were performed for each ordinal variable in the final model, including all the dependent variables significantly associated with the BMI. Two men and 107 women were excluded from the statistical analysis because of incomplete data. Statistical analyses were performed on 1658 men and 1469 women.
Results
The proportion of men and women in the whole sample was 51.3 and 48.7% respectively and the distribution of sex in age groups was globally similar. Using the WHO recommended 30 kg/m2 cut-off point, the overall prevalence of obesity was 9.8% (11.1% among men and 8.3% among women). Furthermore, 32.4% of subjects (44.4% of men and 19.9% of women) had a BMI between 25 and 29 kg/m2.
Body mass index of 1658 men according to clinical and socio-economical characteristics
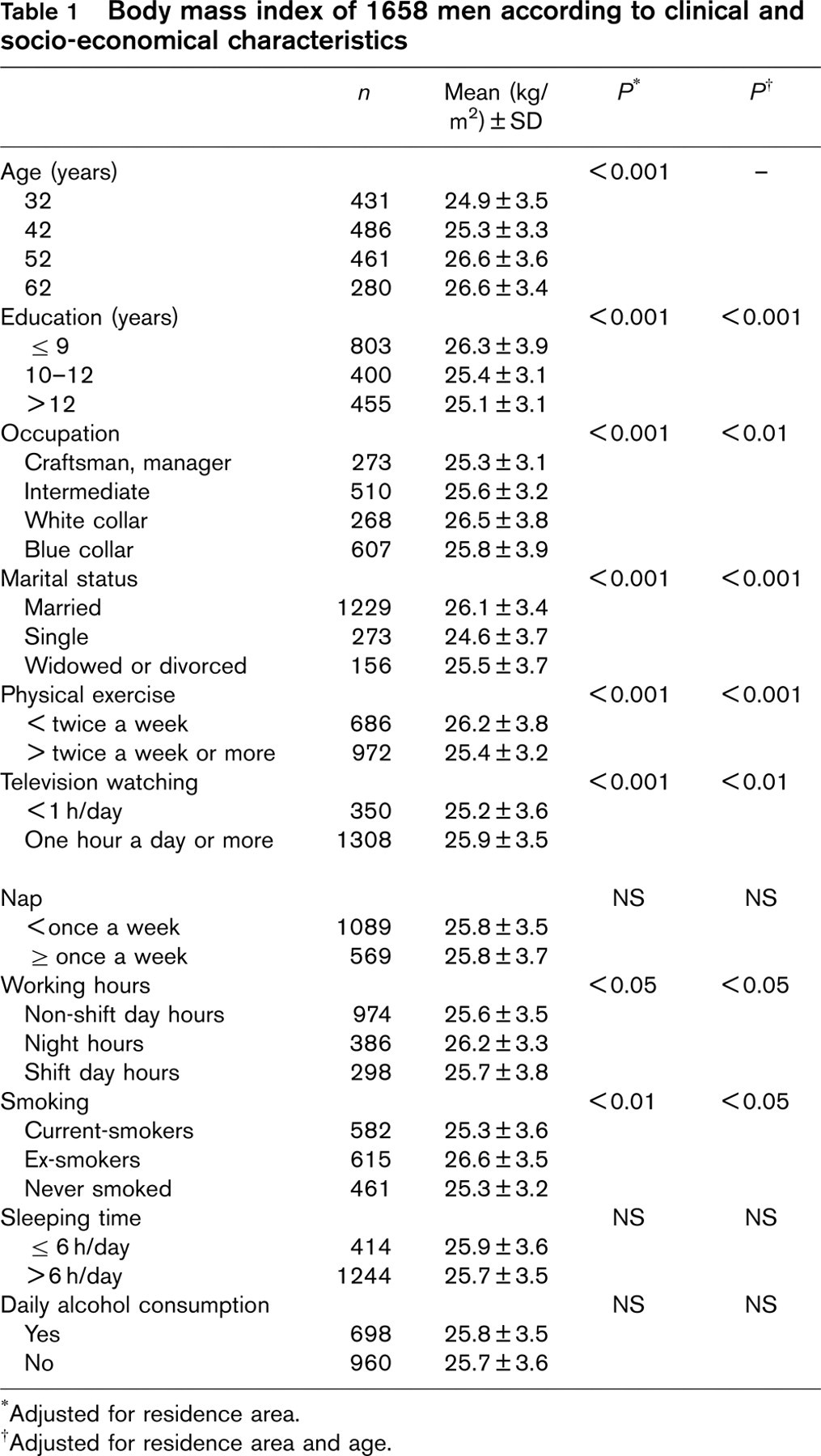
Adjusted for residence area.
†Adjusted for residence area and age.
The mean BMI, according to lifestyle factors, socioeconomical and clinical characteristics, are reported in Tables 1 and 2. In both men and women, BMI was significantly associated with age, increasing from age 32 to 52 years. Low educational level, low physical activity and television watching were found significantly associated with a higher BMI. Craftsmen, managers and intermediate workers had a lower mean BMI than white-and blue-collar workers. The BMIs among married, widowed or divorced subjects were significantly higher than among single subjects. Night workers' BMI was higher than day workers'. Women who had daily alcohol intake had a higher BMI. In women, the BMI was significantly higher in subjects napping at least once a week and in subjects sleeping less than 6 hours per night. The BMI was significantly higher (P < 0.001), in subjects where the difference between the total time spent in bed (non-sleeping + sleeping periods) and the period of actual sleep, was ≤ 2 h. This relationship remained significant after adjustment for age and TV watching (P < 0.04).
Body mass index of 1469 women according to clinical and socio-economical characteristics
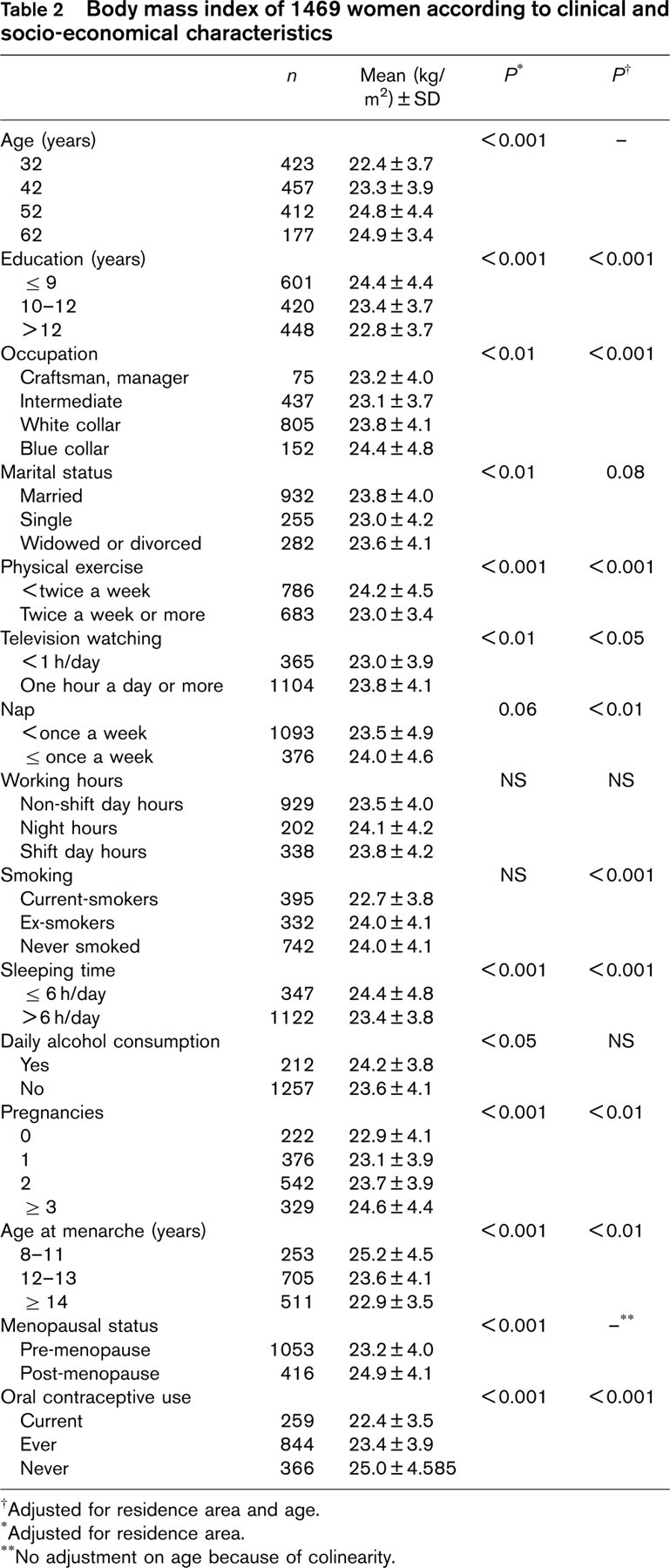
†Adjusted for residence area and age.
Adjusted for residence area.
No adjustment on age because of colinearity.
Moreover, women were significantly heavier in postmenopausal status than in pre-menopausal status. In postmenopausal status, there was no significant relationship between the BMI and the use of hormonal replacement therapy (not shown).
Linear regression coefficients with their standard error and P value describing the relationships between BMI and selected covariates among 1658 men (adjusted for residence area)
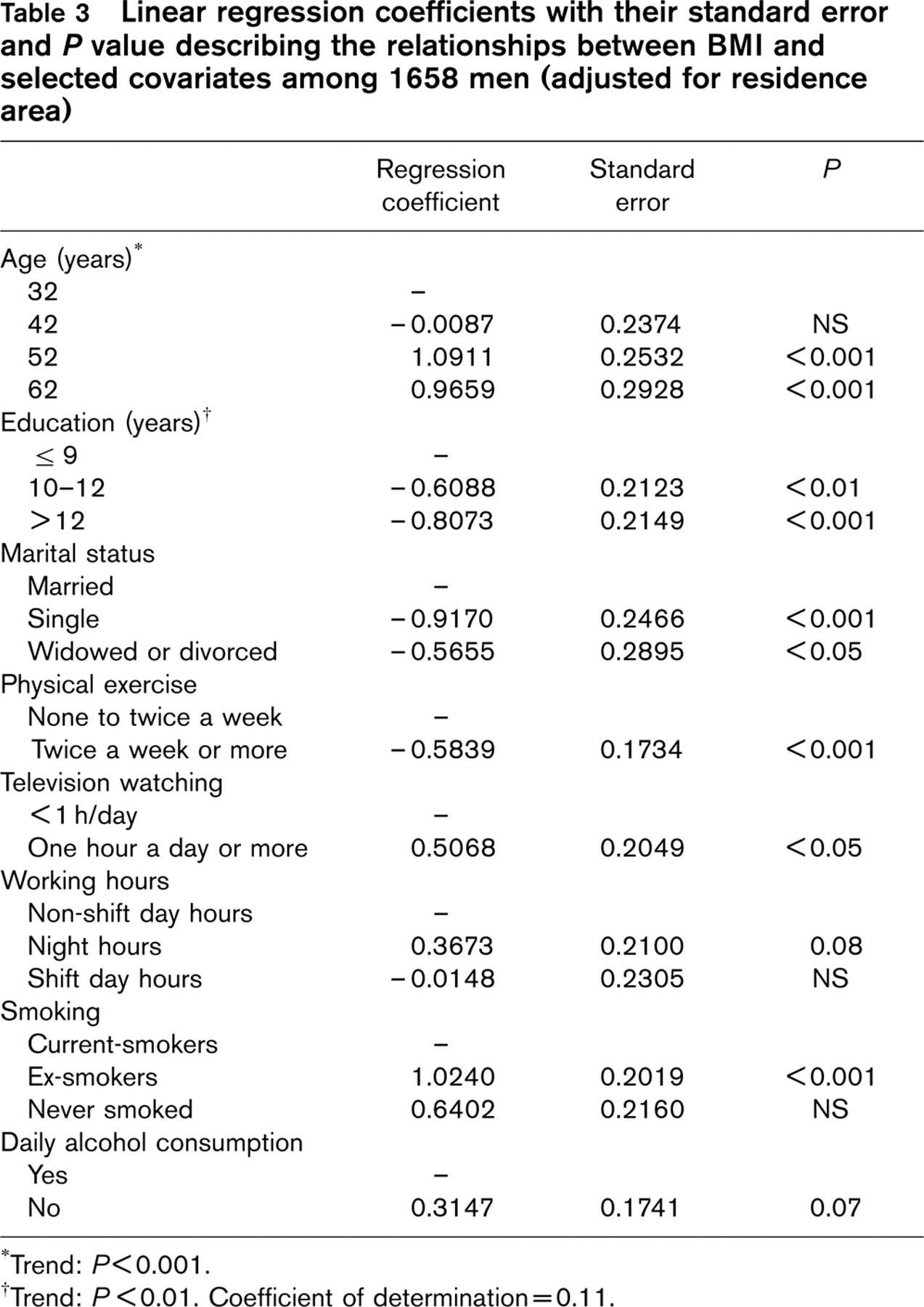
Trend: P< 0.001.
†Trend: P < 0.01. Coefficient of determination = 0.11.
In multivariate analyses (Tables 3 and 4), low educational level, television watching, low physical activities and ex-smoking habits, were positively and independently associated with BMI in both men and women. The BMI was higher for women with short night-sleeps. Women who reported no nap were thinner. The number of pregnancies or an early age at menarche was associated with a higher BMI, showing an increasing and statistically significant trend throughout regression coefficients. The use of oral contraceptives was significantly associated with a lower BMI. This association remained significant in the separate model performed for the 32-year old women after adjustment for educational level, smoking status and pregnancies, (β = 2.02 ± 0.77 for non-users versus current-users, P < 0.01).
Discussion
Even if the VISAT study was not a general population-based study, the overall distribution by socio-professional category was close to the distribution observed at the national level [27]. Moreover, in our sample obesity and overweight prevalence was either similar to or lower than the prevalence found in several European studies, including France [5, 18, 28–30]. However, unlike these studies, our sample did not include people older than 62 years and obesity prevalence usually increases with age, except for older subjects. A potential healthy-worker effect may account for this difference since non-working subjects under 62 years were not recruited. Still, this impact might be considered as minor since the results of a multi-centric study carried out among populations of the same age range and during the same period [31–33] showed that the BMI was lower in the south of France than in the two other studied countries geographically close (Spain and Italy).
Linear regression coefficients with their standard error and P value describing the relationships between BMI and selected covariates among 1469 women (adjusted for residence area)
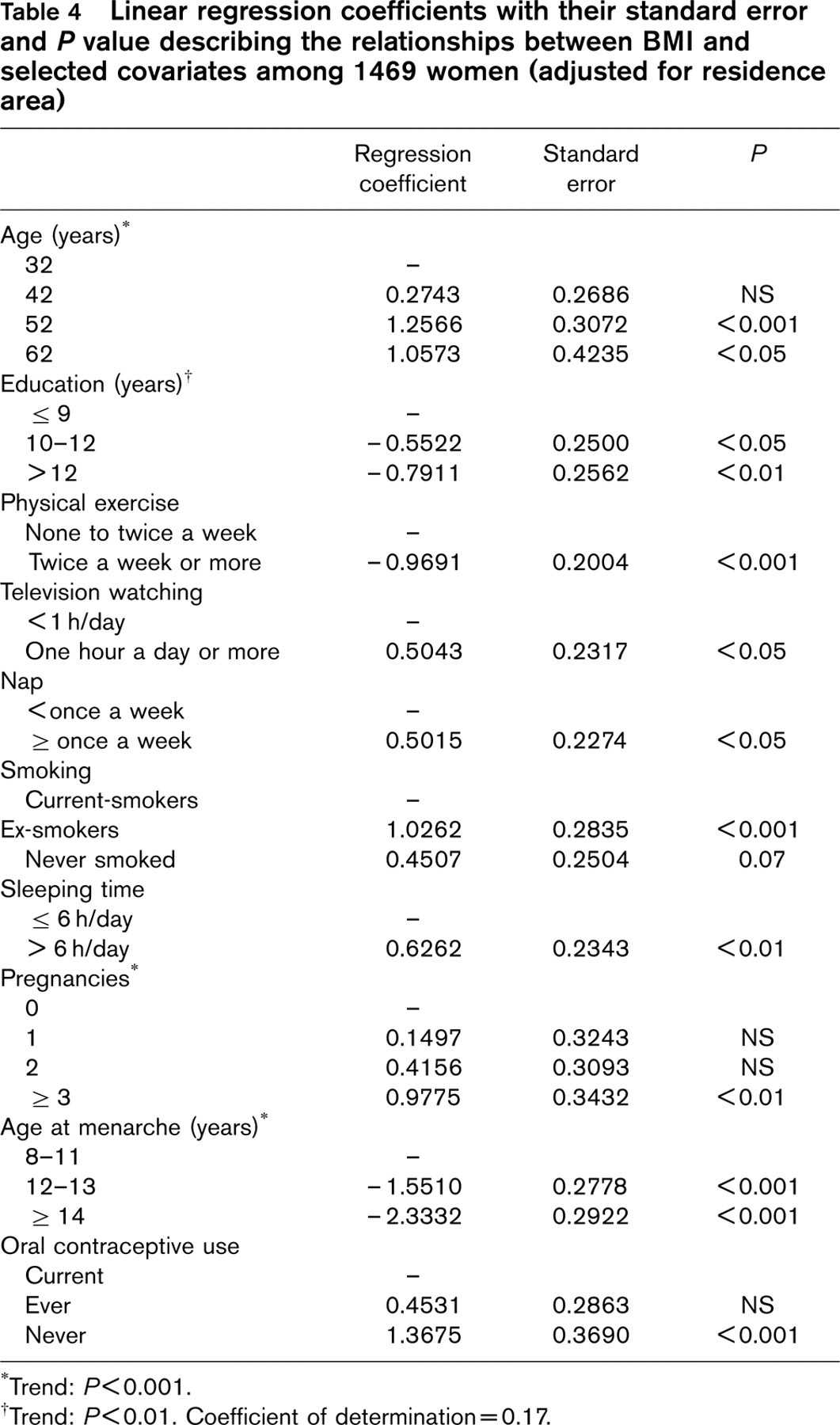
Trend: P < 0.001.
†Trend: P < 0.01. Coefficient of determination = 0.17.
The results of our study did confirm the complex relationships between environmental factors and BMI. Indeed, a great number of variables in multivariate analyses remained significantly and independently associated with the BMI. Some of these variables seemed to refer to very close meanings. But, the fact that both variables were independently associated with the BMI suggests that they might provide different information. For example, the time spent watching TV might provide information not only on energy expenditure but also on energy intake (‘snacking').
The relationship between age, education and BMI have been reported before [9–12, 34, 35]. Three lifestyle variables linked to behavioural changes were strongly and invariably associated in both men and women: physical activities, TV watching and smoking status. These behaviours, studied in previous studies [13–16, 18, 36, 37], could be modified in preventive actions.
An inverse relationship was found between sleep duration and BMI in women. This relationship had already been shown in French children [38] and in Spanish adults [18]. Three explanations have been put forward. First, sleeping disorder prevalence is high in obese subjects. They sleep less since their sleep is unsatisfactory. Second, obese subjects being less physically active need less sleep. Third, obese subjects spend more time watching TV and stay up late. This relationship remained significant after adjustment for physical activity, TV-watching duration and number of naps. Moreover, the test for statistical interaction between sleep duration and number of naps was non significant (P = 0.3). For a better understanding of the sleep-BMI relationship, a complementary analysis was performed for the number of sleepless hours spent in bed and the BMI. We assumed that the difference between the number of hours spent in bed and sleep duration would be an appropriate indicator of the sleepless hours spent in bed reading or watching TV for instance. Conversely to other relationships, a positive relationship between the number of sleepless hours spent in bed and the BMI was found in this context, remaining significant after adjustment for TV watching.
The reported positive relationship between TV watching and the BMI had already been described elsewhere [15, 16, 18, 36]. Time spent watching TV is often considered as an indicator of sedentary lifestyle, responsible for reduced physical activities and lower energy expenditure [39, 40]. But according to several authors, TV viewing is not an index of physical activity [41].
The existence of a direct causal relationship between the use of oral contraceptive and BMI is still debated [42–44]. In our study, the negative association between BMI and the use of oral contraceptive remained significant after adjustment for educational level. Our multivariate analysis included 416 post-menopausal women, unlikely to be current users of contraceptive pills. However, this association was observed only when the group of 32-year old women was analysed, even if this analysis could not exclude certain heterogeneity in the composition of the pills used by the same age range. However, educational level and the present occupation may not be relevant enough to characterize social parameters that may influence the BMI on the one hand and the use of oral contraceptives on the other hand, even though a causal relationship between these two variables was not clearly demonstrated. Another major point that should be underlined is the relative contra-indicated use of estrogen plus progesterone contraceptive in obesity. This contraindication may account for the negative relationship between oral contraceptive and the BMI. However, the part played by this bias is probably insignificant. Indeed, when we analysed the relationship between contraception and the BMI after excluding 133 women whose BMI was ≤ 30 kg/m2 and who might have been concerned by this contra-indication, the results showed that the contraceptive users remained significantly thinner whatever the age-group either in the univariate or multivariate analyses.
In our study, a very stable, strong and highly significant relationship was found between age at menarche and the BMI. When, in the same country, age at menarche was compared in several regions with dissimilar socioeconomical status, the secular decrease in age at menarche was attributed to a general improvement in nutrition [45, 46]. A relationship between age at menarche and the BMI was found whatever the age group. Many previous studies have already described the relationships between age at menarche, height, weight and adiposity in adults. It had been demonstrated that overweight prevalence was higher in early maturing teenagers [24], probably because of an excessive endogenous estrogen production in obesity. But it had been shown that a higher BMI during childhood, adolescence and young adulthood had a stronger effect on subsequent levels of obesity in adults [47–49]. Thus, early age at menarche may induce adult obesity, but obesity in young girls may induce early menarcheal age.
A great number of parameters like nutritional behaviour, genetic factors and other numerous environmental factors, not taken into account in this study, may account for the BMI. Our study used a cross-sectional design, thus allowing no causal relationship.
This study sheds light on numerous social, cultural and behavioural determinants influencing the imbalance between energy intake and energy expenditure responsible for the dramatic worldwide increase of obesity prevalence. Some of these determinants are linked to the southern Europe lifestyle (i.e., napping), but others are much more common and their association with BMI could be extrapolated to a larger population. Among these, three should be modifiable thanks to preventing actions: smoking, physical activity and TV viewing. A better understanding of interactions between these various factors is necessary for an appropriate prevention of the increase in obesity.
Footnotes
Acknowledgements
The authors thank the occupational physicians and VISAT researchers who participated in designing the present project and collected the data. This work was supported by grants from the Centre National de la Recherche Scientifique (CNRS), Conseil Régional Midi-Pyrénées, Ministère de l'Enseignement Supérieur et de la Recherche, Midi-Pyrénées Caisse Régionale de l'Assur-ance Maladie (CRAM), and Ministère du Travail. In the article all contributors decide on their own contributions, which are disclosed to the reader, and on their relative importance to the article, which drives the order in which their names appear in the contributors list and the byline. The editors decide how they wish to display both lists, and the indexing databases and journals set up the rules for how many contributors are cited. Research institutions and societies then use the descriptions of contribution in their assessments of candidates. Dr M. Cournot analysed the data and wrote the first draft of the paper. Dr J.C. Marquié was involved in the design and coordinated the project. Pr J. Ferrières was involved in the fieldwork and supervised the writing of the paper. Dr B. Baracat assisted with the interpretation of the currents results and commented the paper. Dr Y. Esquirol was involved in the analysis of the data and contributed to the interpretation on the current results. Dr J.B. Ruidavets proposed the topic and supervised data analysis and contributed to the writing of the paper.