
Abstract
Background
Randomised, controlled trials focusing on long-term psychological reactions to information about increased risk of coronary heart disease are scarce.
Design
A population-based randomised, controlled, 5-year follow-up trial was conducted in general practice.
Methods
In 1991, invitations were sent to 2,000 middle-aged people registered in the general practices in the district of Ebeltoft, Denmark. A total of 1,507 (75.4%) agreed to participate and were randomised into a control group and two intervention groups: one included health screening, a written feedback and an optional follow-up visit with the general practitioner; the other included health screening, written feedback and a planned 45-min follow-up visit with the general practitioner. The participants were informed at screening about their risk of developing coronary heart disease. Psychological distress was measured by the GHQ-12 before screening and at the 1 and the 5-year follow-up.
Results
Before the screening (0 year), 1 and 5 years after there were no significant differences in the GHQ-12 score between the control group and the two intervention groups. Nor were there any differences related to information about increased risk of coronary heart disease between scores obtained at the 1 and the 5-year follow-up.
Conclusion
Middle-aged persons had no long-term psychological reaction after information about increased risk of developing coronary heart disease following a health screening in general practice evaluated by the GHQ-12,1 year and 5 years after the examinations.
Keywords
Introduction
Health screening aims at identifying individuals at increased risk of developing coronary heart disease (CHD) to allow appropriate prophylactic measures to be taken. Health screening carries the expected but avoidable side effect that some people identified as belonging to the risk group, may react psychologically negatively to the information about an increased risk of CHD [1, 2]. This may be detrimental to their health but the information can also be used to raise adherence with the lifestyle advice given by their general practitioner (GP) [3]. Evaluation of health screening in general practice should therefore balance the positive effects of such information, like reduced morbidity and mortality, against the negative effects, for example, in the form of adverse psychological reactions. The earliest extensive study of psychological reactions using a screening program was performed by Haynes who showed an increase in absenteeism following the detection of hypertension in a group of steelworkers [4]. Present studies on psychological reactions to screening suffer from several weaknesses in their study design [1, 5, 6]. Even so, they indicate that GPs may communicate information about CHD risk factors without triggering a negative reaction that will affect well-being [7, 8]. However, the studies' weaknesses have allowed some expert and opinion makers to address only the potential harmful effects of screening in public [2, 8].
The aim of the present study was to investigate the long-term psychological reactions to information about increased CHD risks.
Methods
The study is a part of the Ebeltoft Health Promotion Project and the design and other parts of the study have been reported elsewhere [9, 10].
Study setting and inclusion of patients
The study took place between 1991 and 1997 in the district of Ebeltoft, Aarhus county, Denmark. All nine district GPs participated. A random sample of 2,000 (57.7%) of the 3,464 inhabitants aged 30–49 years (by 1 January 1991) who were registered with a local general practitioner were invited to participate in the study. The invitation included a one-page questionnaire.
Invitation
All study participants received an invitation to participate including a one-page questionnaire about general demographic and lifestyle related questions in September 1991. Those who agreed to participate received an extensive supplementary baseline questionnaire about their health, lifestyle, psychosocial conditions and life events.
Randomisation procedure to select control and intervention groups
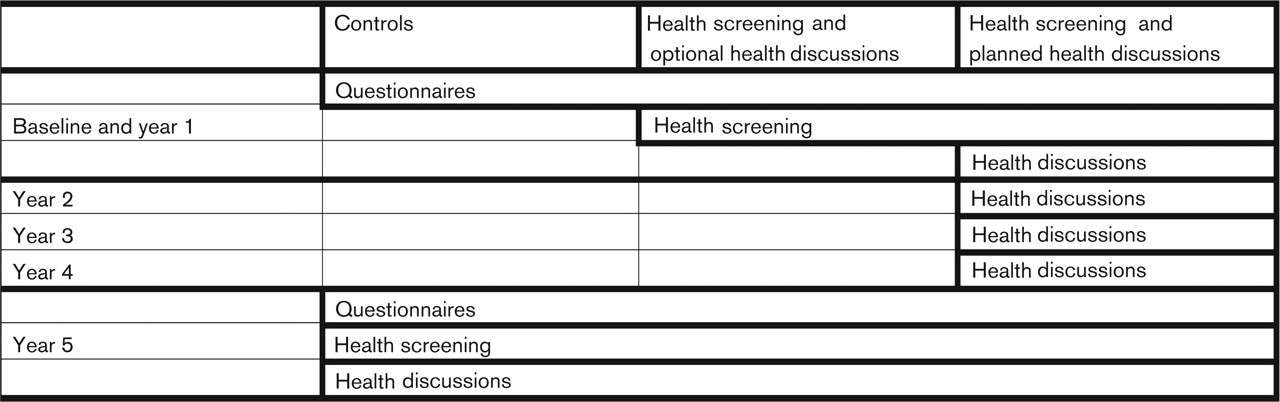
Participants were randomised into a control group and two intervention groups. Both intervention groups were offered a health screening with written feedback from their GP. One of the intervention groups had optional health discussions with their GP while the other group had a planned 45-min follow-up health discussion with their GP and were invited to have an annual health discussion. Participants in the health screening and planned health discussion group were invited to have an annual health discussion. Figure 1 presents the flowchart of the study.
The health screening
The health screening was multiphasic and performed in general practices by three laboratory assistants between December 1991 to June 1992. The risk for developing CHD was estimated by a simple arithmetic model based on the addition of risk factor for coronary heart disease (CRS) [10]. Based on the CRS, the risk was considered low, moderate, elevated, or high. A few weeks after the health screening, all tested participants received personal, written feedback from their GPs, explaining the test results in easily understandable terms. Those who had been informed of an elevated or high CRS were encouraged to see their GP, irrespective of their randomisation group.
The health discussions
Participants in the health screening had a planned 45-min health discussion. Participants with the optional discussion could ask for a normal consultation.
Follow-up
The participants were followed for 1 and 5 years after the baseline intervention as shown in Figure 1. The control group was offered a health screening and an optional health discussion at the end of the study period.
Outcome measure
Before the health screening and at the 1 and 5-year follow-up, psychological distress was measured by the GHQ-12. The GHQ is a self-administered questionnaire developed by Goldberg [6, 11] to measure four elements of distress concerning anxiety/insomnia, depression, social impairment/hypochondria (chiefly indicated by somatic symptoms) and social dysfunction. We used the 12-item ‘GHQ-12' version. A total GHQ-12 score according to the Likert-score method was calculated as the sum of Likert-scores for each item. A high score indicated psychological distress.
Data handling and statistics
Data were analysed with Stata SE 8.0 and SPSS 10.0. Chisquare tests were applied to dichotomous data and the two-sample t-test, Mann-Whitney test or Kruskal-Wallis test to continuous data. The randomised groups were compared at 1 and 5 years follow-up according to the intent-to-treat rule.
Results
Participation at baseline and at follow-up
In total 75% (1,507) of the 2,000 persons invited agreed to take part in the study. Of these, 502 persons were invited to receive a health screening plus an optional health discussion, and 449 did receive the health screening. Among the 504 participants who were offered a health screening with a planned health discussion, 456 received the screening, and 443 accepted the subsequent offer of a health discussion. We found no significant difference in acceptance between those participants who were facing a normal CRS and those who were facing an elevated CRS.
The follow-up rates of all randomised groups were, in relation to response on questionnaires, 84.1% at the 1-year follow-up, 79.2% at the 5-year follow-up, with no significant differences between the groups of randomisation.
We observed no significant differences between the groups in terms of distribution of socio-demographic and cardiovascular risk factors at baseline [9]. Of the 905 persons tested, 11.4% were informed of an elevated or high CRS at baseline.
Impact on outcome measures
Baseline data
The mean GHQ-12 before the health screening (year 0) in the three intervention groups: (a) control (b) health screening with optional health discussion and (c) health screening with planned health discussion was 23.48, 23.24 and 23.33 respectively (Kruskal-Wallis test P = 0.561). The mean GHQ-12 before the health screening (year 0) in the group which was informed about increased risk of CHD was 24.07 and 23.18 in the group which was informed about no increased risk of CHD (Mann-Whitney test P=0.371). There was no difference in the GHQ-12 score at the baseline examination between responders and non-responders (data not shown).
Follow-up data
No significant differences were noted in any of the analyses between the two intervention groups, therefore, data from the two groups are presented together in Tables 1 and 2. We observed no statistically significant change in GHQ-12 scores during the 1 and 5-year follow-up period in relation to information about the increased risk (Table 1). Data were analysed and stratified for randomisation group, smoking habits and self-reported body mass index (BMI). We observed no statistically significant change in GHQ-12 scores during the 1 and 5-year follow-up period in relation to randomisation groups, or when analysed according to participants with increased risk based on self-reported data from baseline (smokers and overweight participants) (Table 2). No significant differences were noted in any of the analyses between the two intervention groups.
Discussion
The result of this study does not support the concerns that information about increased risk for CHD would lead to a negative psychological reaction. There were no psychological reactions at the 1 and/or 5-year follow-up among patients informed about an increased CRS following a screening for CHD.
The psychological reactions were recorded as direct changes in psychological distress (emotional and cognitive), and not by a traditional indirect measure such as work absenteeism. We used the GHQ-12 whose value in recording psychological distress following screening examinations, drug treatment and social stress is well-established [6, 11, 12]. The GHQ-12 used here is particularly suitable for recording changes over time and it provides scores that are well-evaluated and accepted as standard outcome measures in other studies of psychological distress following screening examinations [1, 11, 12].
Change in GHQ-12 score 1 and 5 years after the first examination of participants in the follow-up study in relation to risk for CHD
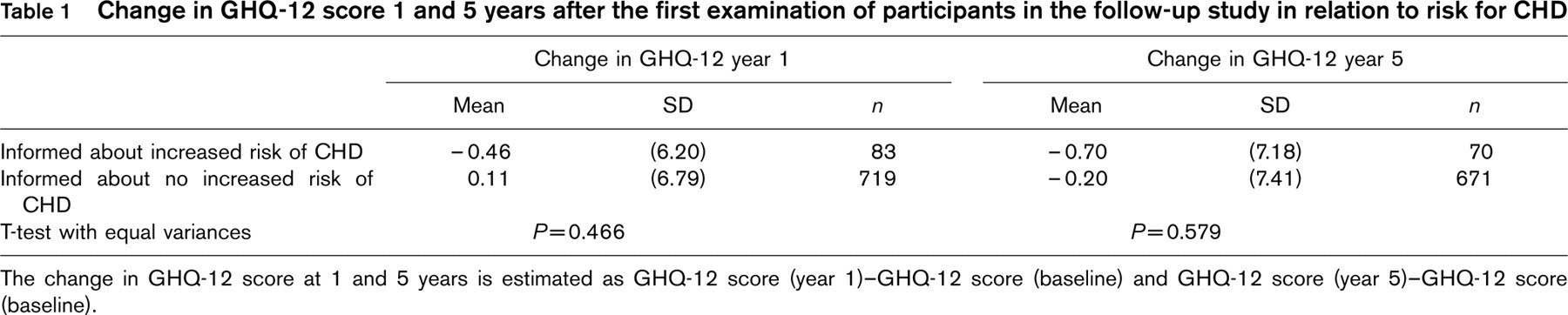
The change in GHQ-12 score at 1 and 5 years is estimated as GHQ-12 score (year 1)–GHQ-12 score (baseline) and GHQ-12 score (year 5)–GHQ-12 score (baseline).
Change in GHQ-12 score 1 and 5 years after the first examination of participants in the follow-up study in relation to randomisation and BMI and smoking habits
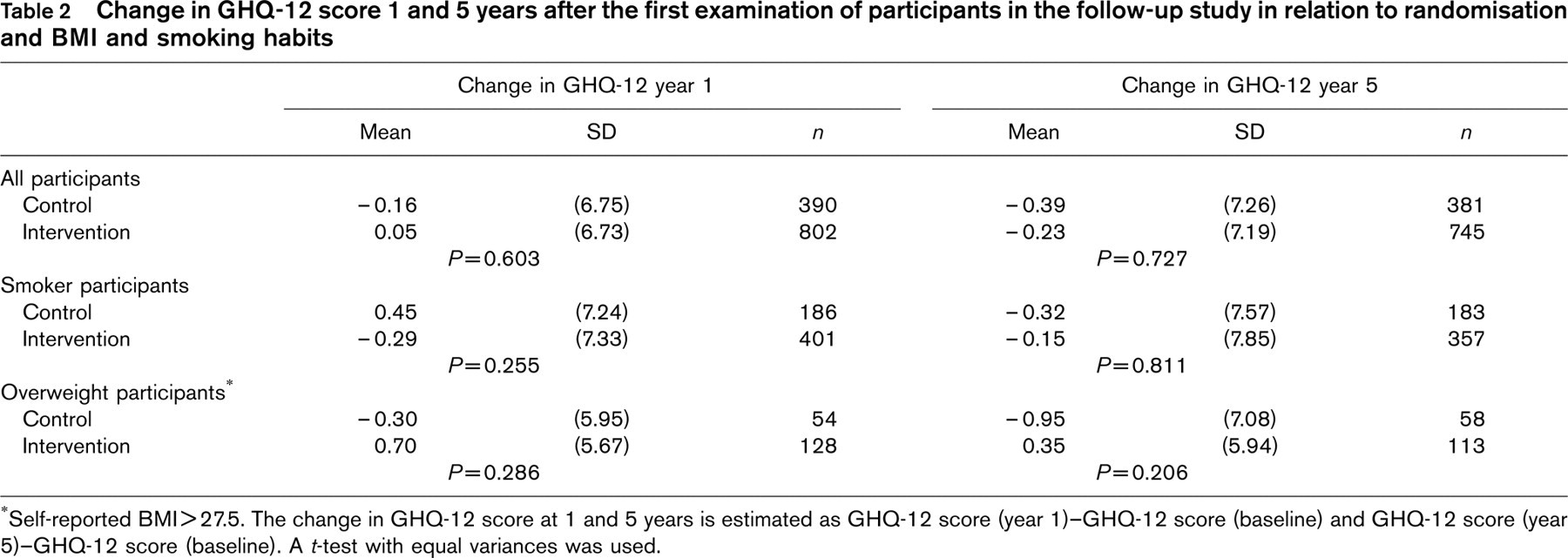
Self-reported BMI>27.5. The change in GHQ-12 score at 1 and 5 years is estimated as GHQ-12 score (year 1)–GHQ-12 score (baseline) and GHQ-12 score (year 5)–GHQ-12 score (baseline). A t-test with equal variances was used.
It could be stated that the relatively low response rate indicates high distress among the non-responders during the follow-up period, but there was no difference in the GHQ-12 score before the screening between these two groups and no change in the GHQ-12 score at the 1 and/ or 5-year follow-up between all participants in the control group and intervention group. Furthermore, we found no difference in change in the GHQ-12 score when we stratified for self-reported risk factors (smoking and overweight) and compared these data to the control group. In these analyses the follow-up rates were the same according to the self-reported risk factors, for instance, smokers compared with non-smokers.
The major strength of this study is that it is the first to offer a long-term perspective on the psychological reaction of health screening in a randomised controlled trail. A systematic review of the psychological impact of predicting individuals' risks of illness concludes that an adverse psychological effect is a common immediate consequence of a positive test [1]. A British study showed that unexpected labelling of increased risk for CHD given without a health discussion with the GP produced an immediate, negative psychological reaction [13]. A more distressing and especially a more long-lasting reaction to information about an increased risk for CHD may reduce the quality of life and reduce the recipient's ability to cognitively cope the information and make appropriate choices regarding future lifestyles and adherence to medical treatment [14]. We would expect persons who had an annual health discussion with the GP not to have any particular long-term psychological reactions, because the GPs long-standing knowledge of the patient could be used to maximum individual effect and to closely follow and counsel the patient in his/her worries throughout. But the study also showed that there was no difference in changes in GHQ-12 in the group where the health screenings were optional.
The study's principal weakness is rooted in ethical considerations. All participants who had been informed of an elevated or high CRS were encouraged to contact their GPs irrespective of their randomisation group. Thus, it is possible that the participants in the intervention group without the planned health discussion had a consultation about the risk for CHD. Yet, the study showed that this group did not experience a long-lasting psychological reaction either.
Previous studies have dealt with psychological distress and sick leave after identification of risk factors for CHD, usually high blood pressure. The results have been inconsistent [1, 5, 8, 11, 13] which is probably so due to various methodological discrepancies and shortcomings such as retrospective design, too few participants, different measures of effect (direct effect measure such as distress, indirect such as sick leave), or differences between the study populations; but also the conditions under which information was given have differed.
Negative psychological reactions to information about the results of screening cannot be entirely avoided, but various strategies may be adopted to counter them [15]. It was not possible to identify precisely what prevented the long-term negative reactions from occurring in this particular study, but it is important that future studies precisely describe the conditions under which the information about the increased risk is given to allow us to ascertain how negative psychological reactions may be prevented. In the present study successful prevention of long-term negative psychological reaction may be ascribed to the following factors: first, participants were invited by means of an invitation explaining the aim of the intervention, and in the invitations it was pointed out the voluntary nature of the study. Second, interpretation of results in the health discussion of the health screening and dissemination of information about an increased risk of CHD lay firmly and exclusively with the GP who enjoyed sole information ownership. Third, the health discussion was carried out by the patient's own GP who could hence use his/her often long-standing knowledge of the patient to gear information to maximum individual effect and to closely follow and counsel the patient in his/ her worries throughout the study period. Fourth, health screenings were based on patient-centred consultations including advice and information and without ‘blaming the victim'.
The study was initiated in 1991. We have no data supporting whether psychological reactions are more or less likely to occur now, but general practitioners are better educated in patient-centred consultations and are in general aware of the potential adverse reaction after health screening and information about risk for CHD.
Conclusion
Middle-aged persons had no long-term psychological reactions after information about increased risk of developing coronary heart disease following a health screening in general practice evaluated by the GHQ-12, 1 year and 5 years after the screening.
Footnotes
Acknowledgements
The following general practitioners participated in the study: A. Bøgedal, P. Grønbæk, L. Jørgensen, P.T Jørgensen, H. Lundberg, J.M. Nielsen, G.S. Pedersen, J.C. Rahbek, N. Bie. We thank Ineta Sokolowski for the statistics analysis and the staff at the GP's clinic in Ebeltoft for their extraordinary effort, including the extensive and brilliant administrative assistance given by A. Hilligsøe and E. Therkildsen.