
Abstract
Background
The monocyte receptor CD14 is an important mediator of the inflammatory response to bacterial endotoxin. Recently, a functional polymorphism in the promoter of the CD14 gene (CD14-260C>T) was found to be associated with coronary heart disease. We examined if this polymorphism was associated with sub-clinical carotid atherosclerosis in a community population.
Design and methods
A randomly selected community population (557 men and 553 women; aged 27–77 years) underwent conventional risk factor assessment and ultrasound evaluation of the common carotid intima-medial wall thickness (IMT) and carotid plaque formation. CD14-260C>T genotypes were examined by restriction fragment length polymorphism analysis. Chlamydia pneumoniae-specific immunoglobulin G (IgG) and immunoglobulin A (IgA) antibody titres were determined by micro-immunofluorescence.
Results
The carrier frequency of the T allele and TT genotype was 0.48 and 0.22 respectively. Genotype frequencies met Hardy-Weinberg expectation. There was no significant association of −260C>T genotypes with traditional risk factors. On multivariate analysis, there was no independent association of genotypes with common carotid IMT in men and women or with prevalence of carotid plaque in women. Contrary to expectation, men who were TT homozygotes relative to CC wild-type had a lower adjusted risk of carotid plaque formation (odds ratio 0.34, 95% confidence interval 0.17–0.69; P = 0.003). There was no evidence that smoking or C. pneumoniae infection modified the association of genotypes with carotid IMT or plaque formation.
Conclusion
The CD14-260C>T gene polymorphism was not associated with an increased risk of sub-clinical carotid atherosclerosis in a community population.
Introduction
A chronic response to inflammatory stimuli, including to infectious agents, has been implicated in the genesis of atherosclerosis and its complications [1]. Cellular response to infection with gram-negative bacteria is mediated by bacterial lipopolysaccharide (LPS, endotoxin), which activates monocytes to express pro-inflammatory cytokines and pro-coagulatory factors via the endotoxin receptor CD14 [2, 3].
An Sp1 transcription factor binding site has been identified in the promotor region of the gene for CD14 receptor and is critical for CD14 expression [4]. Recently, a common C ← T nucleotide substitution polymorphism in the promoter (position −260) of the gene encoding CD14 has been reported [5, 6]. In children and adults, TT homozygotes were found to have higher circulating levels of soluble CD14 (sCD14) than CC or CT genotype carriers [5, 7]. Likewise, in a sample of healthy male volunteers, the TT homozygotes were reported to have a higher density of CD14 receptors on blood monocytes than carriers of the other genotypes [8].
It has therefore been postulated that the CD14–260C > T polymorphism might be involved in inflammatory processes linking bacterial endotoxins to atherogenesis [9]. Indeed, the initial epidemiological studies [6, 8, 10] indicated a positive association of the TT genotype with risk of myocardial infarction (MI) and coronary heart disease (CHD), although this was not confirmed by subsequent investigations [7, 11, 12]. Since the effect of the polymorphism on atherogenesis remains uncertain, we examined for an association between the TT genotype and sub-clinical carotid atherosclerosis in a randomly selected cross-sectional community population [13, 14]. Chlamydia pneumoniae (C. pneumoniae) infection and smoking [15] may be associated with increased circulating endotoxin levels. We therefore tested if C. pneumoniae infection and smoking could interact with the CD14–260C>T polymorphism to increase the risk of carotid atherosclerosis in a general population.
Methods
Subjects
The characteristics of the population have been previously described [13, 14]. Subjects were original participants in the 1989 Australian National Heart Foundation Perth Risk Factor Prevalence Survey [16]. This was a random electoral roll survey of 2000 people from the metropolitan area of Perth, Western Australia. Of these subjects 1111 (61% of those eligible), aged between 27–77 years, and an equal number of males and females in each age decile, agreed to take part in the study described here. Subjects who had previous carotid artery surgery were excluded. The population is predominantly Caucasian. Written informed consent was obtained from all study participants. The study protocol was approved by the Institutional Ethics Committee of the University of Western Australia.
A self administered questionnaire was used to record a history of physician-diagnosed hypertension, hyperlipidaemia, diabetes, angina pectoris, myocardial infarction (MI), stroke, angina hospitalization, or a family history of premature-onset coronary heart disease (CHD) by age 55 years in first-degree relatives [16]. Smoking lifetime exposure by pack-years was calculated. Anthropomorphic measurements and the lower of two resting blood pressures, measured with a mercury column manometer, were recorded by a trained research nurse.
Laboratory measurements
A fasting venous blood sample from each subject was obtained. Total cholesterol, high-density lipoprotein (HDL) cholesterol and triglyceride levels were determined enzymatically with a Hitachi 747 auto-analyser. Low-density lipoprotein (LDL) cholesterol was calculated using a method by Friedwald et al. [17]. Sufficient quantities of sera were available in 1034 subjects for testing of C. pneumoniae antibodies. Titres of C. pneumoniae-specific immunoglobulin G (IgG) and immunoglobulin A (IgA) antibodies were determined by micro-immunofluorescence according to manufacturer's instructions (Labsystems, Helsinki, Finland). Seropositivity was defined as an IgG titer of ≤ 1: 32 or an IgA titer of ≤ 1:8 [18].
Genetic analysis
DNA was available for 1100 subjects. A salt/phenol/chloroform method was used to isolate genomic DNA from leukocytes. Polymerase chain reaction (PCR) was performed in a total volume of 15 ml containing 20ng DNA, 1.7 mmol/l MgCl2, 200 nmol of each dNTP, 1U AmpliTaq gold polymerase (Applied Biosystems) and 5 pmol of each primer F (5'-ATCATCCTTTTCCCA-CACC-3') and R (5'-AACTCTTCGGCTGCCTCT-3'), on a 96-well plate PTC100 thermocycler (MJ Research). The PCR conditions were: an initial denaturation of 10 min at 94°C; followed by 39 cycles of denaturation at 94°C for 1 min, annealing at 55°C for 1 min, and extension at 72°C for 1 min; then a final extension step of 3 min at 72°C. The PCR product (295 bp) was digested with 2 U Hae III restriction enzyme (Promega, Madison, Wisconsin, USA) at 37°C for 3 h. Two bands at 140 and 155 bp identified the C allele; the T allele by a single band at 295 bp after electrophoresis on a 3% agarose gel stained with ethidium bromide. Two examples of each genotype were sequenced to check for the correct genotyping.
Carotid ultrasound
Bilateral carotid B-mode ultrasound was performed by two trained sonographers using a 7.5 MHz annular phased-array transducer on an Interspec (Apogee) CX 200 ultrasound machine as previously described [13]. The intima–medial wall thickness (IMT) was defined as the distance between the characteristic echoes from the lumen–intima and media–adventitia interfaces on the far wall of the distal common carotid artery measured over a 1 cm segment length. A thorough search of the distal common carotid, carotid bulb, and internal and external carotid arteries was also made to determine the presence of focal plaque. Plaque was defined as a clearly identified area of focal increased thickness (≤ 1 mm) of the intima–media layer. Three end-diastolic images were analysed from the right and left distal common arteries at a site free of any discrete plaque and measurements averaged to give the mean IMT. Repeat measurements of randomly selected scans revealed no significant variation in the IMT measurements. Quality control measures included repeat scans on a subset of 30 subjects on two separate occasions 7–10 days apart. The intra-observer coefficient of variability was 2.9% for sonographer I, and 4.8% for sonographer II. The inter-observer coefficient of variability was 5.9%.
Statistical analysis
Outcome variables of the association analyses were mean IMT and the presence of one or more carotid plaques. The principal explanatory variables were the genotyped polymorphisms. The bi-allelic polymorphisms were coded into three classes (e.g., CC = 0, CT = 1, TT = 2) and analysed categorically as two binary (1, 0) dummy variables relative to the most common homozygous genotype for each polymorphism. Sex, the presence of carotid plaques, physician-diagnosed diabetes, hypertension, myocardial infarction (MI), or stroke and family history of CHD were analysed as binary variables. All other variables were analysed as continuous. Cigarette smoking status was analysed both as a binary variable (smoking ever) and as a continuous variable (pack years of smoking). Body mass index (BMI), triglycerides, HDL were not normally distributed and therefore logarithmically transformed prior to analysis. Analysis of variance (ANOVA) was used to contrast mean IMT across the genotypes and χ2 tests on contingency tables for categorical variables. Consistency of genotype frequencies with Hardy–Weinberg equilibrium was tested using a χ2 goodness-of-fit test on a contingency table of observed versus predicted genotype frequencies. Generalized linear regression (GLM) and logistic regression models [19] were used to model the effects of multiple covariates on the continuous and dichotomous outcomes. Possible explanatory covariates, apart from genotype, included age, sex, systolic blood pressure, BMI, waist-hip ratio, total plasma cholesterol, HDL, LDL and triglyceride levels, smoking, physician-diagnosed diabetes, hypertension or MI, and past history of vascular disease (MI, stroke, or angina hospitalization). Each genotype was assessed with the use of dominant, recessive, and additive genetic models. Both forwards and backwards stepwise modelling procedures were used to select a useful subset of independent predictors of an outcome of interest. Checks of goodness of fit [20] included an investigation of the need for interaction terms to look for gene–environment interaction. The GLMs were also used to estimate genotype-specific means and standard deviations. Data were analysed using SPSS (version 10.1; SPSS Inc., Chicago, Illinois, USA). Statistical significance was defined at the standard 5% level.
Results
The mean age of the population was 53.3 years [standard deviation (SD) = 12.7 years]. The sex ratio was balanced; 557 male (50.3%) and 553 female (49.7%) subjects were studied. Approximately 25.6% of the subjects had one or more detectable carotid plaque and 7.8% had a previous history of myocardial infarction, stroke or angina hospitalization.
The carrier frequencies of the CD14–260C> T polymorphism genotypes in the whole sample were 25.9, 52.0 and 22.1% for CC, CT and TT respectively. The allele frequencies [T allele: 48.1%, 95% confidence interval (CI) 45.9–50.1%] were consistent with Hardy–Weinberg equilibrium (χ2 = 0.95, P = 0.62). The genotype distributions and allele frequencies were not significantly different between males and females.
When the whole sample was analysed according to −260C > T genotype, it was found that subjects carrying the CT or TT genotypes were significantly older (Table 1). All other clinical risk variables were similar between genotypes including smoking history (ever) and IgG and IgA seroprevalence to C. pneumoniae.
CD14 gene polymorphism and common carotid mean IMT
Univariate analysis showed that there was an association between the −260C>T polymorphism and mean IMT (P = 0.006) in the whole population (Table 1) and in females (P = 0.004) but not males (P = 0.14). However, the relationship between CD14 genotype and IMT was largely confounded by age (Table 1). After multivariate analysis adjusting for age and standard risk factors, there was no residual association of the genotypes with mean IMT in the whole sample or in males and females separately (Table 2). Multivariate analysis found no evidence of an interaction with standard risk factors, including smoking history (P for interaction = 0.60), or with C. pneumoniae IgG or IgA seropositivity (both P for interaction > 0.60). No association of genotype with carotid IMT was found when analysis was confined to subgroups defined by ever smoking or C. pneumoniae seropositivity (results not shown).
CD14 gene polymorphism and carotid plaque
Univariate analysis showed that the polymorphism was not associated with the presence of carotid plaques in the whole population sample (P = 0.76) (Table 1), nor in men (P = 0.17) or women (P = 0.22). Multivariate modelling also indicated no significant association of the T allele with the likelihood of carotid plaque in the whole population after adjusting for age and standard risk factors (Table 3). Exploratory analysis suggested a significant interaction between TT genotype and gender (P for interaction = 0.02). When the population was stratified by sex, no association was found in women, but male TT homozygotes was found to have a lower likelihood of carotid plaque compared to their CC counterparts (OR 0.34, 95% CI, 0.17–0.69; P = 0.003) (Table 3). There was no evidence of a significant interaction between genotype and other standard risk factors, including smoking history (P for interaction = 0.20) and C. pneumoniae IgG or IgA seropositivity (both P for interaction > 0.45).
Demographics of whole population by CD14–260C>T genotypes
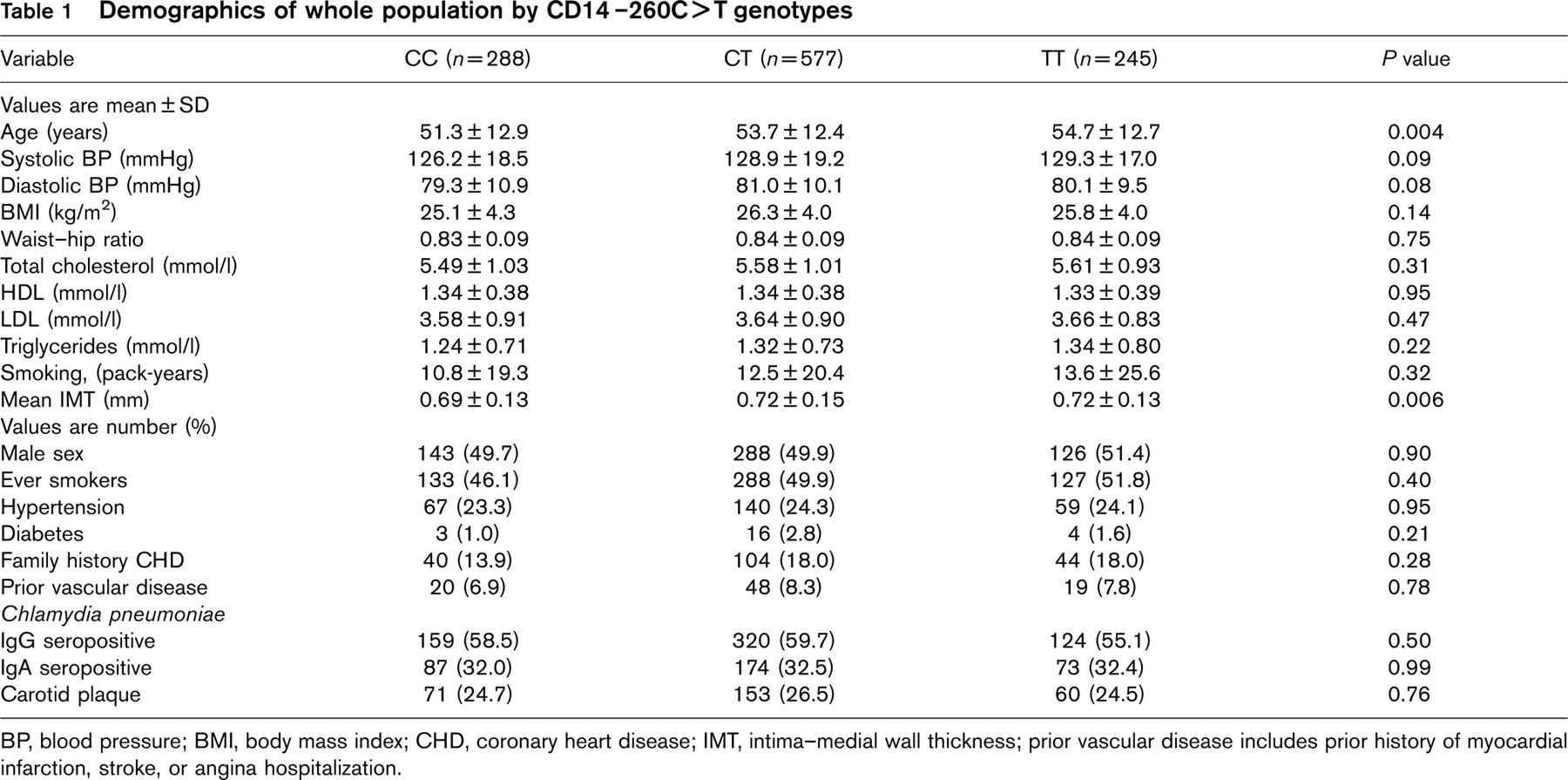
BP, blood pressure; BMI, body mass index; CHD, coronary heart disease; IMT, intima–medial wall thickness; prior vascular disease includes prior history of myocardial infarction, stroke, or angina hospitalization.
Multivariate adjusted carotid mean IMT for CD14 −260C>T genotypes in the whole population and when stratified by gender

Genotype-specific means from GLM model adjusted for age, systolic blood pressure, low-density and high-density HDL-cholesterol, waist-hip ratio and cigarette smoking (pack years). IMT, intima–medial wall thickness.
Adjusted odds ratio for carotid plaque with CD14–260C>T polymorphism in the whole population and when stratified by gender

Genotype-specific odds ratios (GR) and 95% confidence intervals (CI) from logistic regression model adjusted for age, low-density lipoprotein cholesterol, smoking (pack-years), hypertension, diabetes and previous history of vascular disease.
Discussion
Our study does not generally support an independent association between the CD14–260C>T polymorphism and carotid IMT or prevalence of carotid plaque in a healthy community population. The frequencies of the CD14 genotypes in our population sample were similar to those described in other predominantly Caucasian populations [6, 8, 11, 12]. Contrary to expectation, subgroup analysis confined to males only indicated that those who were homozygous TT compared to CC wild type had a significantly lower adjusted odds ratio for carotid plaque formation. There was no evidence that smoking or seropositivity for C. pneumoniae modified the relationship between CD14 genotypes and carotid IMT or plaque formation.
Our results add to the growing body of conflicting evidence regarding the role of the CD14 promoter polymorphism in inflammation and atherosclerosis. The initial retrospective studies suggested the CD14–260C>T polymorphism to be associated with an increased risk of MI and CHD [6, 8, 10]. These studies along with those that provide a possible mechanism through increased CD14 expression [5, 7, 8] suggested that the CD14–260C> T gene polymorphism might indeed be a risk factor for atherothrombotic vascular disease.
However, in the initial report by Hubacek et al. [8] containing 178 Czech men with MI and 135 controls, it is apparent that the observed positive association could well have arisen from an over-estimation of allele frequency based on an inadequate number of control subjects. Unkelbach et al. [6] reported a null finding in a study of 2228 men with suspected CHD, and the observed association with MI was found only in a subgroup analysis of 76 subjects who were non-smokers, normotensive and aged > 62 years. Another positive study [10] was reported in a small Japanese population (128 CHD patients and 83 controls), and a positive association was seen only in those with a recent MI and not those with stable CHD. Subsequent larger case–control studies [7, 12] and the prospective Physicians' Health Study [11, 21] found no evidence of an association of the CD14 promoter polymorphism with CHD, MI or stroke.
The present study addressed the question of whether a functional CD14 polymorphism might be associated with sub-clinical carotid atherosclerosis in a large cross-sectional community population with equal numbers of randomly selected males and females in each age decile. Measurement of an increased common carotid IMT has previously been used as a measure of sub-clinical atherosclerosis in a general population [22]. Prospective studies have also shown that increased IMT predicts future cardiovascular events, including risk of MI and stroke [23, 24]. The major finding of the present study was that there were no differences in mean IMT across CD14 genotypes after adjustment for age and other standard risk factors (Table 2).
To our knowledge, Risley et al. [25] are the only other investigators to have reported the association of the CD14 gene polymorphism with carotid IMT. They found in a German healthcare population (n = 992), aged 50–65 years, that the CC genotype was independently associated with thickened (> 75th percentile) common carotid IMT although the association was limited only to current and ex-smokers. In the latter subgroup (n = 503), they found that the CC compared to TT genotype was associated with an increased adjusted odds ratio of thickened IMT (2.02; 95% CI, 1.23–3.34; P = 0.006). They were unable to test for the association between genotype and plaque because of the relatively low prevalence of plaque in their population.
Risley et al. [25] explained the association of the CC genotype with increased carotid IMT on the basis that smokers are known to have increased endotoxin exposure [15, 26], that carriage of the C allele has been associated with lower levels of circulating sCD14 [5] and that this may result in a reduced capacity to neutralize the endotoxin [27, 28]. Their results appear to contradict the earlier case–control studies that suggested the T allele to be associated with an increased risk of MI and CHD [6, 8, 10]. However, Riseley et al. [25] speculated that the relationship of the CD14 gene polymorphism to inflammation and atherosclerosis might be complex. They suggested that carriage of the T allele which upregulates CD14 receptor expression might heighten acute inflammatory response to endotoxin, but conversely, higher levels of circulating sCD14 associated with the T allele may reduce chronic inflammation by better clearance of the ligand.
Our results do not support their findings with the CD14 gene polymorphism and smoking. We found no evidence of a gene–smoking interaction effect on carotid IMT in the whole population or in subgroups stratified by previous history of smoking. We also found no evidence of an independent association between genotypes and prevalence of carotid plaque in the whole population or evidence of a gene–smoking interaction. Unexpectedly, exploratory analysis suggested a gender–gene interaction on carotid plaque, and subgroup analysis confined to males only found that TT compared to CC homozygotes had a significantly lower adjusted odds ratio for carotid plaque (Table 3). A gender-specific effect of the gene cannot be excluded but we believe that a chance finding was also possible given that it was derived from subgroup analysis, it was not consistent with carotid IMT results, and the same effect was not seen among females.
Recent studies have suggested a causal relationship between chronic infection, inflammation and atherosclerosis [1, 29]. Chlamydia pneumoniae is a gram-negative bacteria possessing lipopolysaccharide (LPS, endotoxin) and has been the infectious agent most commonly implicated in atherosclerosis [30]. However, Coles et al. [18] found no association between seropositivity for C. pneumoniae and carotid IMT or plaque in our general population. Other population studies have also examined the association of C. pneumoniae infection with early carotid atherosclerosis with conflicting results [31, 32]. In the present study, we looked for a possible interaction between C. pneumoniae infection and CD14 genotypes on carotid IMT and plaque formation. We found no evidence that the CD14 genotype modified the association between C. pneumoniae infection and early carotid atherosclerosis. However, we cannot exclude the possibility that other infectious agents or the total bacterial burden may be more important in atherogenesis.
Overall, we found no clear evidence of an independent association between the CD14 −260C >T polymorphism and sub-clinical carotid atherosclerosis in a large randomly selected cross-sectional community population. We also found no evidence for a gene–environment effect in smokers or those with previous C. pneumoniae infection. Further studies are necessary to more clearly elucidate the potential relationship between CD14 gene polymorphism, endotoxin-mediated inflammatory responses and atherosclerosis.
Footnotes
Acknowledgements
The study was supported by grant-in-aids from NHMRC (211980), Ray Florence Shaw Foundation (to B. McQ.) and HeartSearch WA (to C.C. and J.B.).