
Abstract
Background
With the recognition that serum homocysteine may cause cardiovascular disease there is clinical interest in homocysteine measurement to guide treatment with folic acid. It is uncertain whether treatment is best directed at those with high homocysteine or those at high risk irrespective of initial homocysteine.
Design and methods
Dose-response plots of the associations between serum homocysteine and ischaemic heart disease and deep vein thrombosis were determined from retrospective (case-control) studies (a meta-analysis of 12 age-matched studies) prospective studies and studies of the C677T MTHFR polymorphism (a comparison of risk in three genotypes in a meta-analysis of 72 studies). The value of serum homocysteine as a screening test was assessed from distributions of serum homocysteine in men who did and did not die from ischaemic heart disease in a large prospective study.
Results
There were straight-line relationships between serum homocysteine and disease events in the three types of study; a given decrease in homocysteine would produce a similar proportional risk reduction from any pre-treatment level. There was substantial overlap between the distributions of serum homocysteine in men who did and did not die of ischaemic heart disease, indicating poor screening performance; there was no serum homocysteine cut-off that concentrated the majority of disease events into a small minority of the population.
Conclusion
Interventions to lower serum homocysteine, if judged to be worthwhile, should not be limited to people with a high homocysteine but should be offered to everyone at high risk, regardless of pre-treatment homocysteine.
Introduction
Three recently published meta-analyses have strengthened the evidence that the relationship between serum homocysteine and vascular disease is one of cause and effect [1–3]. There are statistically highly significant associations with ischaemic heart disease, deep vein thrombosis and pulmonary embolism. The associations are quantitatively similar in prospective observational studies and in studies of people with and without a common genetic variant that increases serum homocysteine levels (MTHFR). With the recognition that folic acid lowers serum homocysteine [4, 5], there is clinical interest in using it to prevent circulatory diseases, and the results of randomized trials are awaited to provide confirmatory evidence of this. Commentators have responded to this, however, by advocating that we measure serum homocysteine in patients, with a view to folic acid treatment only in those with relatively high homocysteine levels [6–10], and guidelines have recommended treating homocysteine levels if they are above but not below 12 μmol/l [11]. This view implies the presence of a threshold in the dose–response relationship between serum homocysteine and vascular disease–some point below which further homocysteine reduction produces little or no further reduction in risk.
For other cardiovascular risk factors (such as serum cholesterol and blood pressure) it has been shown that such thresholds do not apply – that the dose–response relationships are continuous and that most disease events occur in people with values of cholesterol and blood pressure close to the population average. This means that serum cholesterol and blood pressure should be lowered in all patients at high risk of disease events, irrespective of the initial levels of cholesterol or blood pressure [12–14]. We investigate whether this is also the case for serum homocysteine.
Methods
Dose–response plots of the association between serum homocysteine and ischaemic heart disease events and deep vein thrombosis were determined from meta-analyses of three types of study–prospective studies (in which the blood samples for the homocysteine measurements were taken in healthy people and subsequent disease events recorded), retrospective (or case–control) studies (in which the blood samples for homocysteine measurements were taken after the disease events, and so may potentially be affected by the disease event) and studies of persons with 0, 1 and 2 copies of the 677 C ← T mutation in the gene coding for the MTHFR enzyme (which produces a modest increase in serum homocysteine). We analysed data from two large prospective studies [15, 16], selected because they were large cohorts with relative risk estimates close to the median for all published prospective studies of homocysteine and ischaemic heart disease events from meta analyses [1, 2]. Dose–response plots were constructed from the published relative risk estimates, stratified according to subgroups (fourths) of serum homocysteine.
We conducted an original meta-analysis of retrospective (case–control) studies of serum homocysteine and ischaemic heart disease and deep vein thrombosis, identifying studies using Medline, Embase, CINHAL and Cochrane Library searches up to October 2001 (subject headings: homocysteine, homocystine, ischaemic heart disease, coronary artery disease, myocardial infarction, deep vein thrombosis or thromboembolic disease). Retrospective studies were selected in which individual serum homocysteine levels in age-matched cases and controls were published (generally in the form of individual data points in plots). Such data were obtained from 2429 cases for ischaemic heart disease (seven studies) [17–23] and 781 cases for deep vein thrombosis (five studies) [24–29]. Dose–response relationships were obtained by ranking the cases and separately the controls from all the study populations combined according to the homocysteine measurements, dividing the controls into four equal groups according to increasing serum homocysteine, and using the same homocysteine cut-off values that defined these four groups to divide the cases into four groups. Defining the odds in cases to controls of an ischaemic heart disease event and a deep vein thrombosis in the lowest homocysteine group as 1.0, the odds ratio in each of the three higher groups was determined.
For the MTHFR studies, we analysed data from a published meta-analysis [1]. A dose–response relationship was derived (albeit across a narrower range of homocysteine values) by plotting the relative odds of a disease event against serum homocysteine in persons with 0, 1 and 2 copies of the variant allele.
The value of serum homocysteine measurement as a screening test for ischaemic heart disease events was assessed by comparing the distributions of serum homocysteine concentration in people who did and did not die of ischaemic heart disease in a large cohort study of men aged 35–64 years at entry [16]. This is one of the largest of the cohort studies that examined the prospective association of serum homocysteine and ischaemic heart disease events and the strength of the association between homocysteine and ischaemic heart disease in this study was close to the median for all such cohort studies [1]. In general, wide separation between affected and unaffected distributions would indicate a good screening test, whilst substantial overlap would indicate a poor screening test.
Results
Figure 1 shows the summary dose–response relationships of cardiovascular disease events against serum homocysteine in subgroups of study populations with different average homocysteine levels. Plots are shown on ischaemic heart disease events from the two large prospective studies (314 events), the meta-analysis of retrospective (case–control) studies reported here (2429 events) and the published meta-analysis of the MTHFR studies (12,193 events). Plots are shown on deep venous thrombosis (with or without pulmonary embolism) from the meta-analysis of the retrospective studies reported here (781 events) and the published meta-analysis of the MTHFR studies (3439 events).
In Figure 1, the odds of a disease event relative to that in the lowest group, on the vertical axis, is plotted using a proportional or logarithmic scale, and when plotted in this way the plots yield reasonably straight lines. Examination of the risk estimates, and the associated 95% confidence intervals, make a threshold effect within the population range of values unlikely.
Figure 2 shows the distributions of serum homocysteine concentration in men who did and did not die of ischaemic heart disease in the large cohort study [16], as two overlapping Gaussian curves. There is substantial overlap between the two distributions. Using a cut-off serum homocysteine level of 18 μmol/l as an example, the detection rate for ischaemic heart disease deaths is 13% (that is, homocysteine was >18mmol/l in 13% of men who died of ischaemic heart disease) and the false-positive rate is 5% (that is, homocysteine was > 18 μmol/l in 5% of men who did not die of ischaemic heart disease). Whatever homocysteine cut-off is chosen to define a high risk category, the proportion of all men who died of heart disease who would be included in the category ‘high risk', is little greater than the proportion of men who did not die of ischaemic heart disease. Serum homocysteine, like the other risk factors, is a poor screening test.
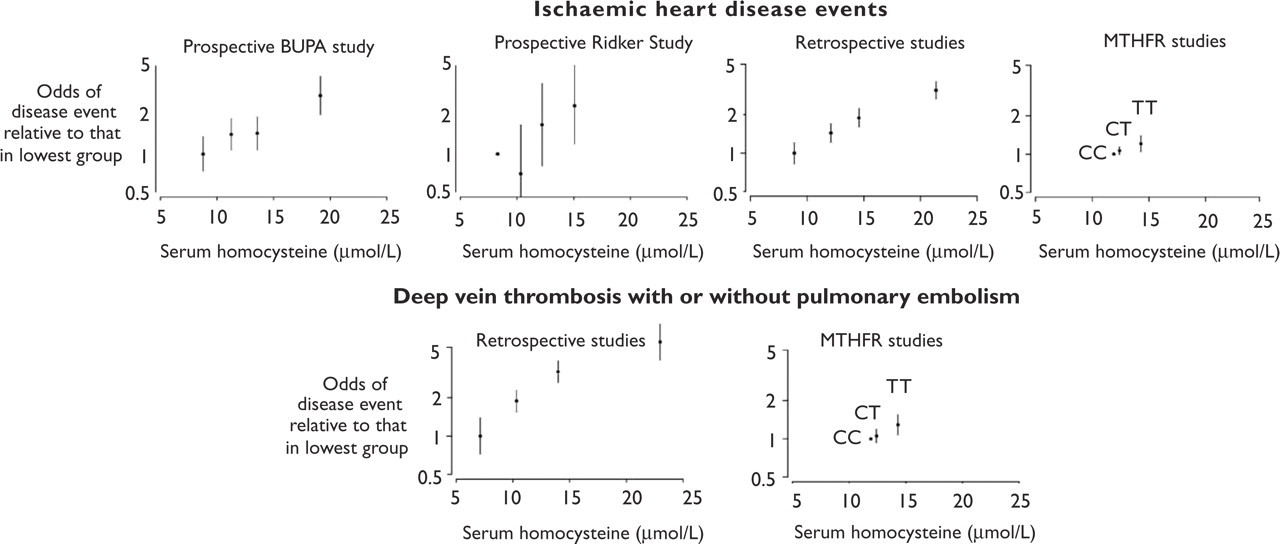
Dose–response relationships between serum homocysteine and risk of ischaemic heart disease event and of deep vein thrombosis (with or without pulmonary embolism), from two large prospective studies (relative risk estimates close to the median for all such published studies), and meta-analyses of retrospective studies and of studies of persons with 0 (CC), 1 (CT) and 2 (TT) copies of the 677 C ← T mutation of the gene coding for the MTHFR enzyme.
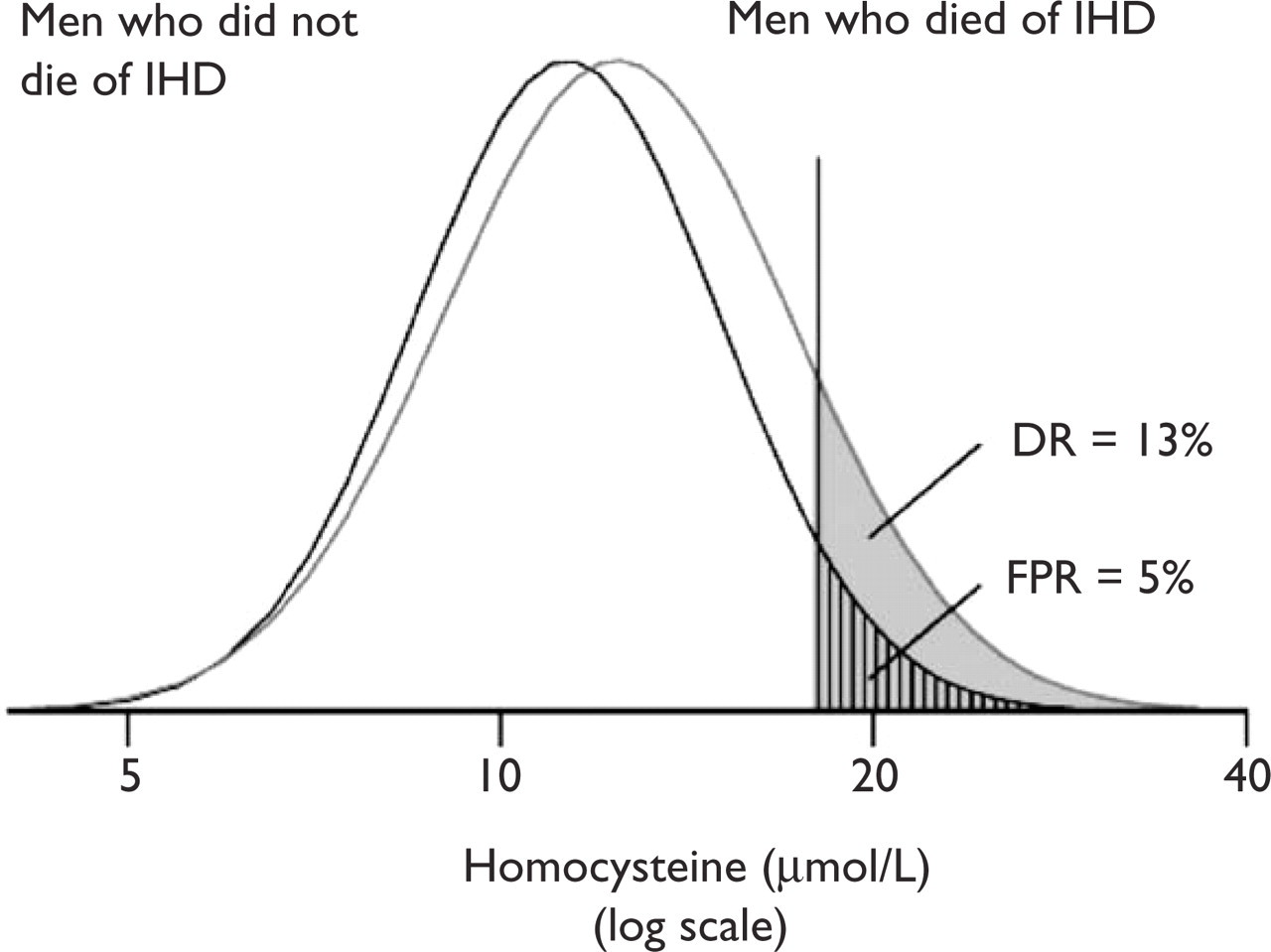
Overlapping distributions of serum homocysteine concentrations in men who did (mean serum homocysteine 12.4 μmol/l) and did not (mean serum homocysteine 11.3mmol/l) die from ischaemic heart disease in the BUPA study [16]. For a homocysteine cut-off level of 18 μmol/l as an example, the detection rate (DR: proportion of men who died with homocysteine above the cut-off) and false-positive rate (FPR: proportion of men who did not die with homocysteine above the cut-off) are shown.
Discussion
The value of the population based observational studies reviewed here is that, unlike randomized trials, they show the disease incidence across the entire range of values of a risk factor in the population. The straight line relationships in the plots indicate that, as for other cardiovascular risk factors [12], there are approximately constant proportional relationships between serum homocysteine, ischaemic heart disease and deep vein thrombosis and this is supported by the results of a recent meta-analysis of prospective studies on homocysteine and ischaemic heart disease [2]. Two other recently published meta-analyses have strengthened the evidence that the relationship between serum homocysteine and vascular disease is one of cause and effect [1, 3], although opinion on causality remains divided [30]. On the basis that the association is causal, it follows from the constant proportional relationships shown here, that a given decrease in serum homocysteine from any point on the distribution would be expected to produce a similar proportional decrease in risk. The absolute reduction in risk would be expected to be greatest in those at highest absolute risk of a cardiovascular disease event (not necessarily those with the highest homocysteine). A 25% reduction in serum homocysteine (achievable with folic acid) may be more important in a person with average homocysteine levels but at high risk (because of a previous myocardial infarction for example) than in a person with a high serum homocysteine but at low risk (young and without a past history of vascular disease for example).
For other cardiovascular disease risk factors, the continuous dose–response relationship across the range of risk factors in Western populations arises from the fact that today's average levels can be considered high in that they are not typical of values throughout human evolution [12]. Studies of isolated communities with a hunter–gatherer lifestyle typical of the Stone Age (where vascular diseases are uncommon) shows that most people in present Western populations have values above the prehistoric average [12], and that the increase in cholesterol, blood pressure and other risk factors with age that is characteristic of Western populations does not occur in the hunter–gatherer communities. The same applies to homocysteine (average serum concentrations were 13.4 μmol/l and 9.7 μmol/l in the two types of population [30]), supporting the observation (Figure 2) that a person's homocysteine level is a relatively poor predictor of an ischaemic heart disease event.
It follows that, as with the other cardiovascular risk factors [12], intervention to lower serum homocysteine should not be limited to people with a high serum homocysteine, but should be offered to everyone at high risk whatever the reason for the high risk.