
Abstract
Objective
Although many epidemiological studies have suggested that increased serum uric acid levels are a risk factor for mortality, this relationship remains uncertain. This cohort study examined the effects of serum uric acid level on death from cancer, atherosclerotic cardiovascular disease (ASCVD) or all causes in men.
Method
A 9-year, prospective cohort study was carried out with 22 698 Korean men, aged 30 to 77 years, who received health insurance from the National Health Insurance Corporation and who underwent biennial, secondary medical evaluations in 1992–1996. The main outcome measures were death from cancer, ASCVD or all causes, compared by quintiles of serum uric acid level. At baseline, the mean (SD) level of serum uric acid was 354.4 (98.1) μmol/l.
Results
During 199 746 person-years of follow-up, there were 387 cancer deaths, 323 ASCVD (99 ischaemic heart disease, 192 stroke) deaths and 1625 all-cause deaths. In multivariate Cox proportional hazards models, having controlled for age, current smoking, diabetes, hypertension and hypercholesterolaemia, uric acid levels were not associated with mortality from cancer, ASCVD or all causes. However, for those with diabetes, uric acid levels were associated with mortality from all causes even after full adjustment of the covariates. When the interaction term was included in the multivariate model, there was significant interactive effect of uric acid with diabetes (RR = 1.26, 95% confidence interval 1.02–1.55) on the risk of all cause of death, whereas the effects of uric acid itself did not attain significance.
Conclusion
These findings indicate that uric acid level is not an independent risk factor for death from cancer, ASCVD or all causes.
Introduction
Results of some prospective cohort studies have suggested a modest direct association between serum uric acid levels and an overall risk of death from atherosclerotic cardiovascular disease (ASCVD) [1–4] and cancer [5]. Some investigators, however, have argued that these results are probably due to the association of uric acid level with other risk factors [6–8]. While the dominant aetiologic role of uric acid in death is well recognized [9, 10], uric acid has not been established as a causal risk factor for cardiovascular disease. Rather, the precise relationship between uric acid level and death remains unclear, and the assertion of such a relationship is controversial because, (a) uric acid seems inextricably linked to hypertension, dyslipidaemia and disordered glucose metabolism, which all play a causal role in the pathogenesis of cardiovascular disease [8, 11] and (b) the relevant studies have been limited by small sample sizes and short follow-up periods [7, 12].
In this large prospective study of 22 698 Korean men, therefore, we have specifically examined the relationship between serum uric acid level and death from cancer, ASCVD, or all causes.
Materials and Methods
Study participants
In Korea, employees of the government and teachers in private schools participate in the Korea Medical Insurance Corporation (KMIC), now a part of the National Health Insurance Corporation (NHIC). Of the entire Korean population (approximately 43 million in 1992), 4 603 361 (11%) were insured by the KMIC, including 1 213 594 workers and their 3 389 767 dependents. All insured workers are required to participate in biennial medical examinations [13, 14]. In 1992, 94% completed the biennial primary examinations for insured persons. Subsequently, the biennial primary examinations for insured were completed in 1994 (95% participation) and 1996 (94%). Those whose primary medical examination showed values outside the normal range results for total cholesterol, blood pressure, fasting blood glucose or urinary protein, about 10% of the total group, were required to undergo a secondary medical examination, which included special tests for uric acid, creatinine, blood urea nitrate and other laboratory evaluation. Nevertheless, most of the participants of the secondary examination were healthy and had values within the normal range (Table 1). We have now used these secondary examinees as the study population for a prospective cohort study of serum uric acid and death.
The cohort, with a follow-up of up to 9 years (average 6.5 year, SD 1.9 year), includes the 22 825 Korean men from 30 to 77 years of age who received health insurance from the NHIC and who completed secondary medical evaluations from 1992 to 1996. Forty-three subjects (0.2%) with incomplete data on the uric acid were excluded, as were 50 (0.2%) who reported a history of any form of cancer or ASCVD, and 34 (0.1%) who died before the date of follow-up, leaving a final sample size of 22 698. Of the study participants, 6995 (30.8) were enrolled in 1992, 5227 (23.0%) in 1994 and 10476 (46.2%) in 1996.
Data collection
The NHIC biennial examinations are conducted in a standardized fashion by medical staff at local hospitals or places of employment. In the 1992, 1994, and 1996 questionnaires, participants were asked to describe their smoking habits, including the number of cigarettes smoked per day and the duration of cigarette smoking in years, along with other health habits including alcohol consumption. The completed questionnaires were reviewed and edited by trained staff and then entered into an electronic database. The data were further edited in creating analysis files.
The primary medical examinations included measurements of weight, height, blood pressure, serum total cholesterol and fasting serum glucose. In addition, secondary medical examinations included serum uric acid, creatinine and blood urea nitrate. Blood pressure was measured in the seated position by a registered nurse or blood pressure technician using a standard mercury sphygmomanometer or automatic manometer. A fasting serum specimen was drawn and analysed for total cholesterol, glucose, uric acid, creatinine and blood urea nitrate. Each hospital participating in the examination had internal and external quality control procedures directed by the Korean Association of Laboratory Quality Control.
Using data collected in the examination, the participants were classified as ‘current' smokers if they reported smoking currently for at least 1 year, ‘never-smokers' if they had never smoked, or ‘ex-smokers' if they had smoked but had quit for at least 1 month by the time of interview. Current smokers were further classified according to the average number of cigarettes smoked per day (1–9, 10–19 or 20 or more cigarettes per day) and duration of smoking (1–10, 10–19, 20–29 or 30 or more years).
Baseline clinical characteristics according to quintile of serum uric acid level (μmol/l)
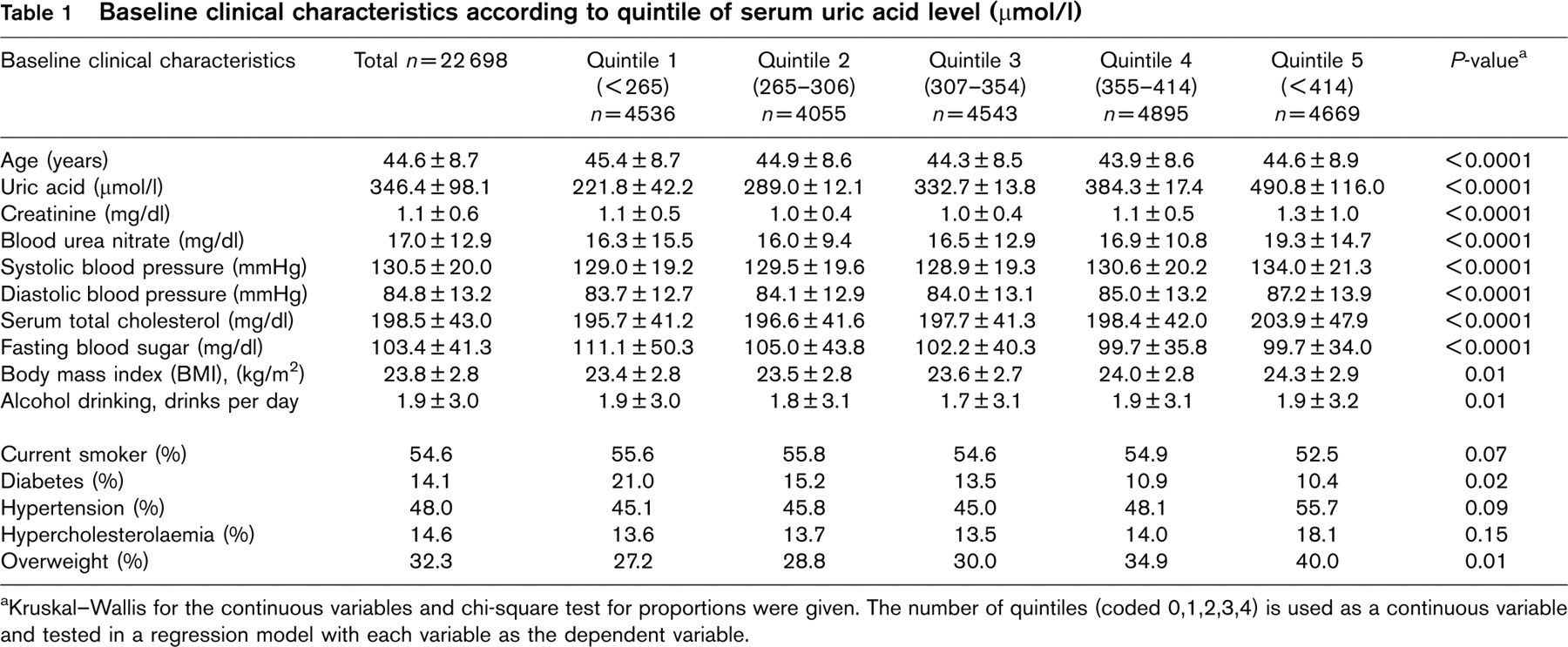
Kruskal–Wallis for the continuous variables and chi-square test for proportions were given. The number of quintiles (coded 0,1,2,3,4) is used as a continuous variable and tested in a regression model with each variable as the dependent variable.
Body mass index was calculated as weight in kilograms divided by height in metres squared. Hypertension was defined as a systolic blood pressure of at least 140 mmHg or a diastolic blood pressure of at least 90 mmHg. Using National Cholesterol Education Program guidelines [15], serum total cholesterol was classified as desirable (serum cholesterol level, < 200 mg/dl), borderline-high (serum cholesterol level, 200–239 mg/dl), or high (serum cholesterol level, ≤ 240 mg/dl). Using diagnostic criteria from the National Diabetes Data Group [16], diabetes was defined as a fasting serum glucose level of 126 mg/dl or higher.
The follow-up period was up to 9 years, from 1 January 1993 to 31 December 2001. The exact dates of completion of the survey form were not recorded. Consequently, follow-up accrual began on 1 January of the calendar year following the year in which the survey form was completed. Persons who completed a survey but died within the calendar year of the survey were excluded.
Outcomes
The principal outcome variables were death from cancer, ASCVD, or all causes, based on both national cancer registry data and hospitalization records. While Korea has a national cancer registry, reporting is incomplete and does not capture all incident cases. Consequently, hospital admission files were used to identify a first admission event for cancer. In Korea, professionally trained and certified medical chart recorders abstract charts and assign discharge diagnoses and codes in a standardized fashion. An incident cancer or ASCVD case was coded as occurring based on either a positive report from the national cancer registry or a hospital admission for a cancer or ASCVD. Follow-up was initiated based on the time of the earliest event. Outcomes for mortality were ascertained from the causes of death on the death certificates. A computerized search of death certificate data from the National Statistical Office in Korea was performed using the unique identification number assigned to all Koreans at birth. Causes of death are assigned at the hospital by a trained abstractor.
All cancers were classified according to the 9th and 10th revisions of the International Classification of Disease. In a random sample (n = 100) of lung cancers that occurred among the KMIC enrollees, we confirmed with a medical chart review that 95.7% of lung cancer diagnoses were valid [17].
Statistical analysis
Bivariate analyses provided information about the relationship between uric acid quintile levels and related factors such as creatinine, blood urea nitrate, blood pressure, serum total cholesterol, fasting blood sugar, body mass index, alcohol consumption and smoking status. All participants were divided according to uric acid level quintiles. In order to assess the independent effects of uric acid on cancer and ASCVD events, Cox proportional hazard models were used. In each model, age, smoking, body mass index, serum cholesterol, alcohol drinking, exercise and diabetes were controlled to delineate the independent effects of uric acid level. An interaction term of diabetes (yes/no) and uric acid level (high/low) was added to the model to examine their interaction.
Results
Participant characteristics
Table 1 shows the baseline clinical characteristics according to the quintile value of serum uric acid level at baseline for the whole study population. The mean uric acid level was 345.4 μmol/l (range, 6 to 978 μmol/l). The uric acid level was increased with age. Those with higher uric acid levels were more hypertensive, hypercholesterolaemic and obese; however, they also had lower levels of fasting blood sugar (P < 0.001). The effect of fasting serum glucose on uric acid level is illustrated in Figure 1.
Uric acid level and outcome events
During the 199 746 person-years of follow-up, there were 387 cancer deaths, 323 ASCVD (99 ischaemic heart disease [IHD], 192 stroke) deaths and 1625 all-cause deaths. As a continuous variable, baseline uric acid level was not associated with increased risk for cancer death, ASCVD death or all-cause death. The baseline quintile of serum uric acid level was also not associated with increased risk for any outcome measure (Table 2) or for IHD or stroke (Table 3). Although quintiles 3, 4 and 5 exhibited increased risks of total stroke mortality when compared with quintile 1 as the reference category, they were not significant in either the unadjusted or adjusted model.
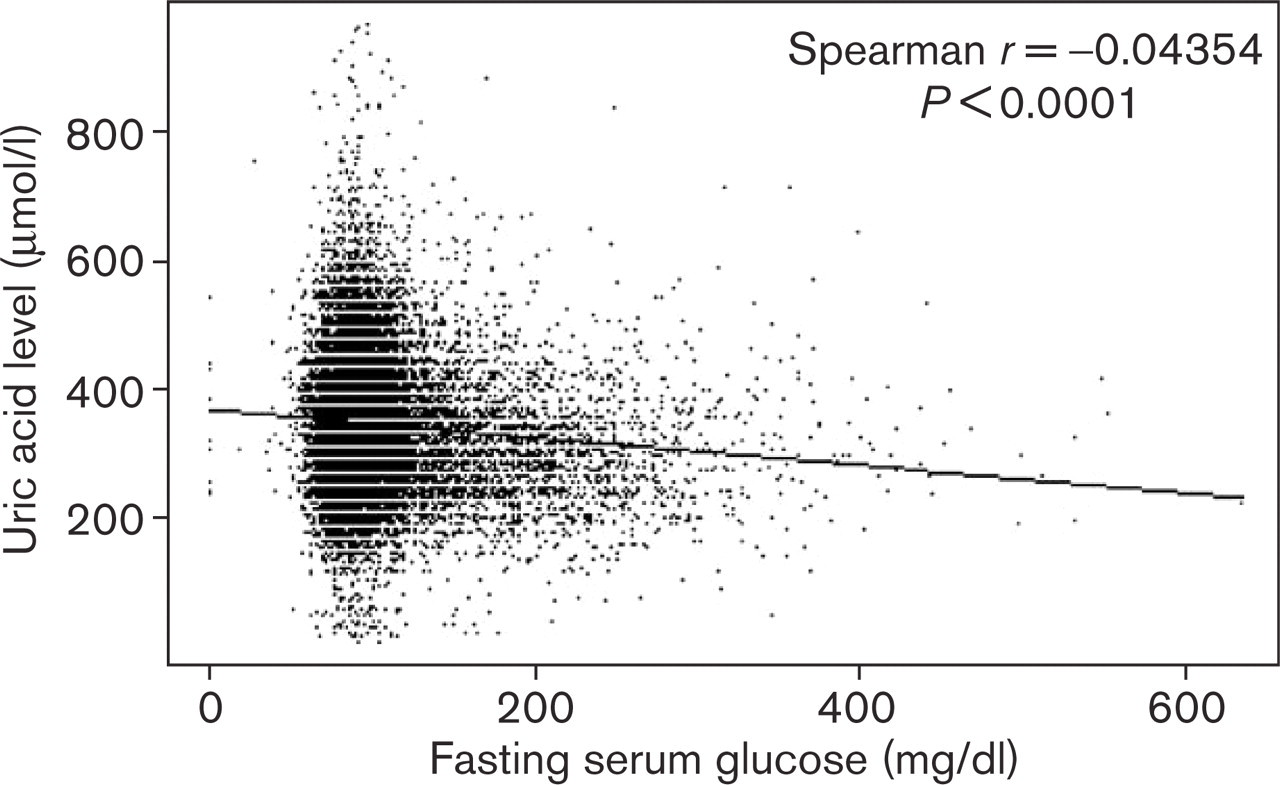
Mean serum uric acid level according to the fasting serum glucose level in men.
In those with diabetes, however, serum uric acid level was associated with increased risk of all-cause death in all three different models (Table 4). In the unadjusted Cox model with quintile 1 as the reference category, the risk significantly increased at uric acid quintiles 4 and 5 for all cause death (P < 0.0523 for trend). The significance of this trend increased after adjustment for age and other covariates. In the fully adjusted Cox models, baseline uric acid level in diabetics was significantly correlated with increased risk for all-cause death (P = 0.0399 for trend). However, among those without diabetes, serum uric acid level was not associated with all-cause death. When an interaction term was added to the model, the statistical significance for the interaction term of diabetes and uric acid was significant (P = 0.0194) (Table 5).
Discussion
The results of this prospective, observational study of a large sample of Korean men suggest that serum uric acid level is not an independent risk factor for all-cause death.
Several prospective epidemiological studies have investigated serum uric acid level as a significant risk factor for death from ASCVD [1–4] or cancer [5], but with inconsistent results. Some have reported no association [6–8, 18], whereas others have reported an increased CVD [1–3, 19, 20]. Although most previous studies have shown a positive association between serum uric acid level and mortality in general, reliable information about subgroup analysis is scarce. Even in the case of studies that have reported a positive association between uric acid level and a particular group, such as patients with angiographically proven coronary artery disease [12], patients with non-insulin-dependent diabetes mellitus [21], or stroke survivors [22], the results have been criticized because of small sample sizes and short periods of observation.
Relations of serum uric acid level to death from cancer, cardiovascular disease and all-causes
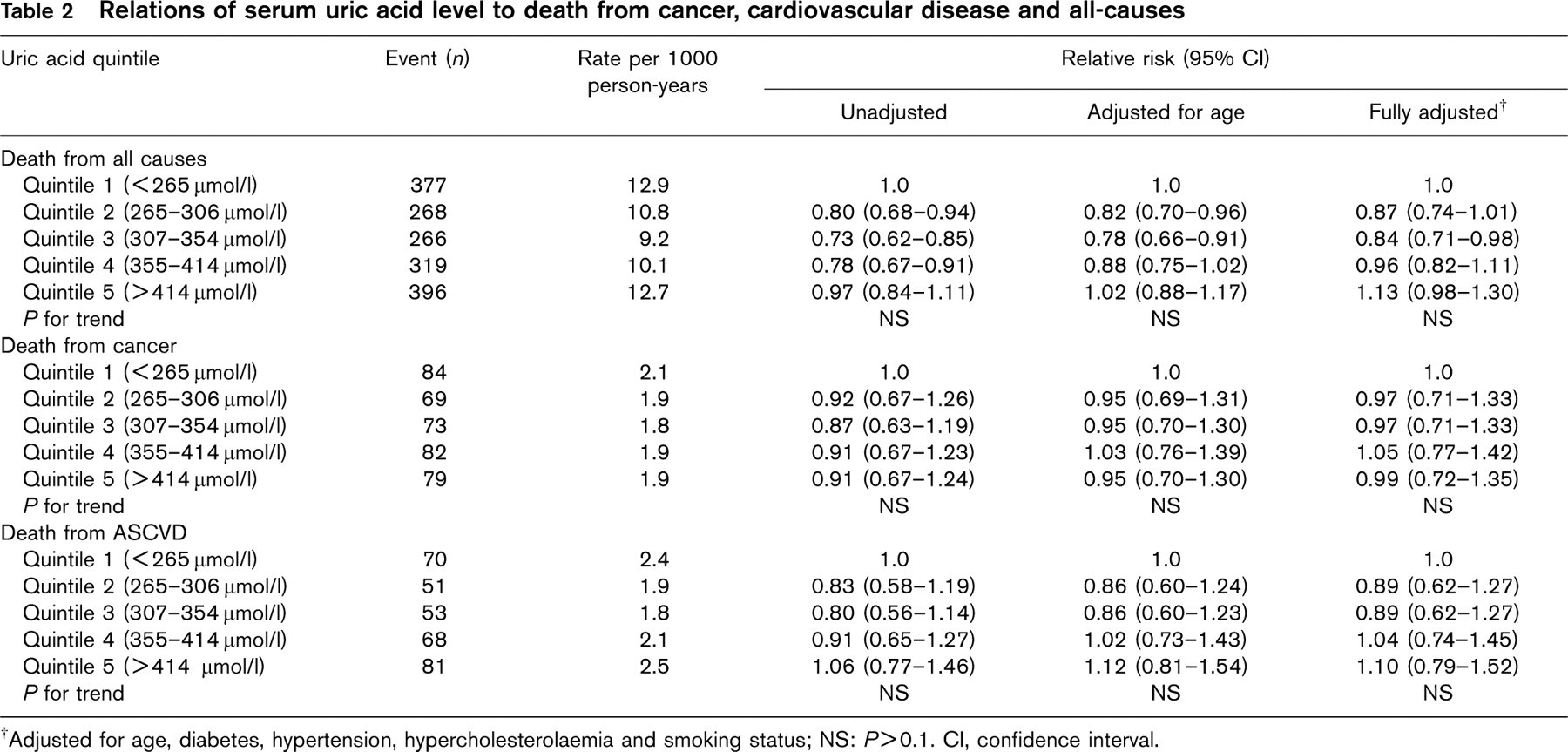
Adjusted for age, diabetes, hypertension, hypercholesterolaemia and smoking status; NS: P > 0.1. CI, confidence interval.
Relations of serum uric acid level to death from ischaemic heart disease and total stroke
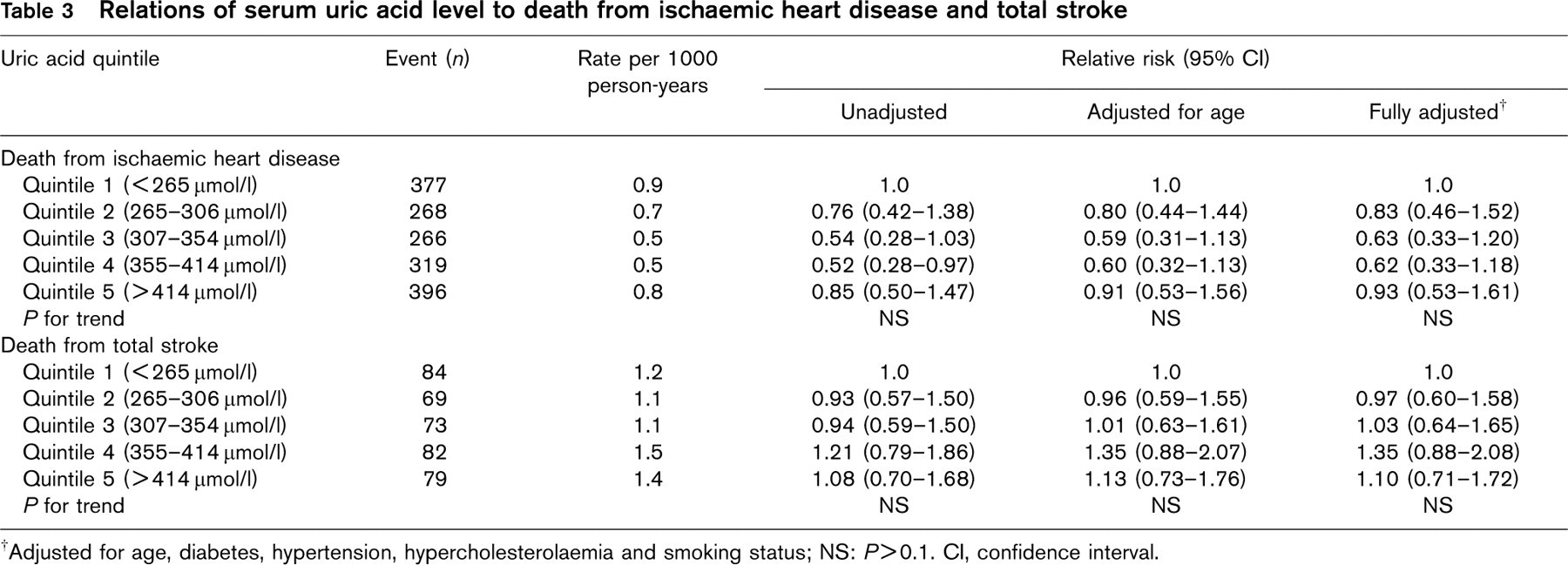
Adjusted for age, diabetes, hypertension, hypercholesterolaemia and smoking status; NS: P > 0.1. CI, confidence interval.
Relations of serum uric acid level to death from all causes according to diabetes and non-diabetes
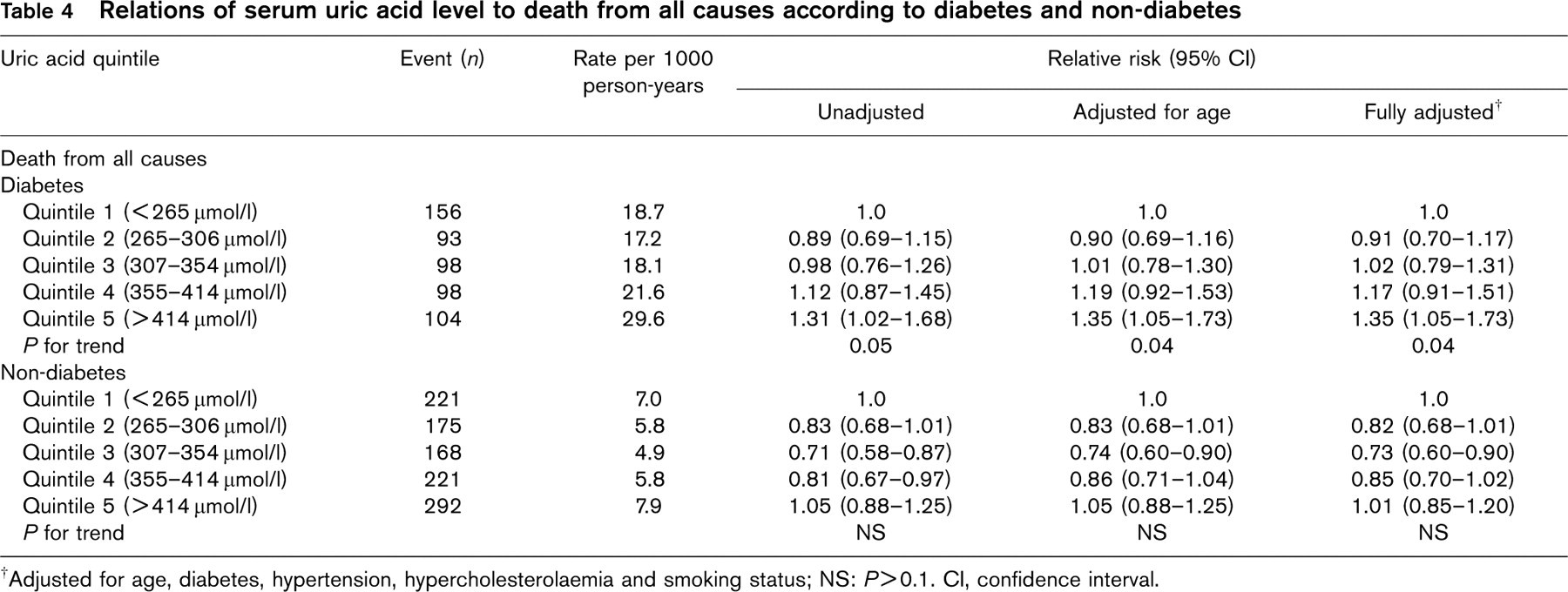
Adjusted for age, diabetes, hypertension, hypercholesterolaemia and smoking status; NS: P > 0.1. CI, confidence interval.
Relative risk of uric acid quintile with interaction term of diabetes and uric acid quintile in multivariate model
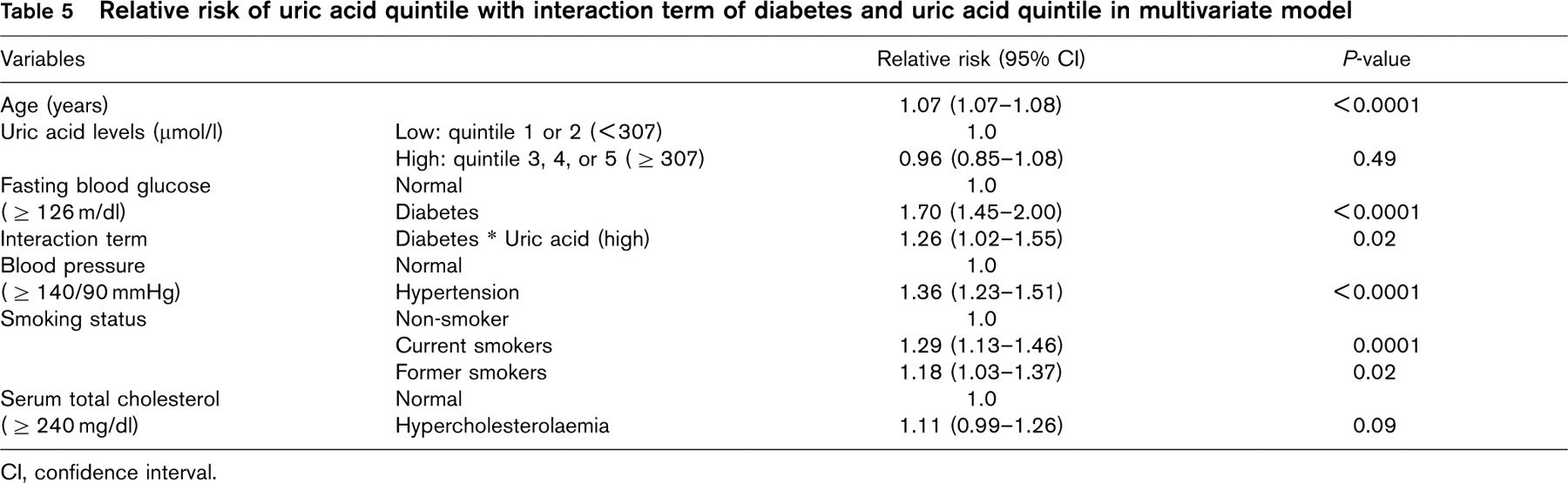
CI, confidence interval.
The Framingham [8] and NHANES I [1] epidemiologic follow-up studies have reported that serum uric acid levels are not associated with cardiovascular disease or death from all causes. The present findings support the results of these studies. Both of these studies, as well as our own, comprised basically healthy subjects, and this similarity in approach may explain, in part, the similar results obtained.
To assess the potential relationship between serum uric acid and mortality without some of the limitations that were identified in previous studies, we took the following approach. First, the sample size of our study, more than 22 000, was large, about 200 000 person-years of follow-up, and a total of 1625 deaths from all causes. This large sample size provided sufficient power to allow us to assess the effect of serum uric acid level on death from all causes, while controlling for other potential confounding factors. Secondly, in our analyses we specifically focused on partitioning the effect of uric acid level on death according to diabetes status, since diabetes is a well-known cause of death. After stratification by diabetes status, uric acid level was found to increase the mortality risk from all causes for the diabetes group alone. These results suggest that the coexistence of diabetes and a high uric acid level increases the risk of death from all causes. To examine this possibility, we then tested the interaction term of diabetes and uric acid level using a Cox proportional hazard model. When an interaction term was added to the model, the statistical significance for the interaction term of diabetes and uric acid level was significant (P = 0.0194). However, fasting blood sugar and uric acid were used as continuous variables; the authors found that interaction terms of them were marginally significant at a = 0.01 (P = 0.0671) and we left it as inconclusive at this point. This finding suggests that uric acid increases the mortality risk from all causes among diabetics.
In general, diabetes, impaired renal function, and diuretics increase the serum uric acid level [11]. Those with higher serum uric acid level often have an association with a history of diabetes [12]. Furthermore, the question has been also raised as to whether uric acid is associated with insulin resistance [23, 24]. However, we have now shown that fasting blood glucose is negatively associated with serum uric acid level (Fig. 1). Similar results have also been reported in a study by Lehto (1998) [21], in which men with high uric acid levels (≤ 295 μmol/l) had lower levels of plasma glucose than did those with low uric acid levels (< 295 μmol/l). Therefore, further investigation into the association between diabetes and uric acid level is needed.
A potential limitation of our study was the relatively brief duration of follow-up and our reliance on death certificates. We believe, however, that the large size of the cohort (> 20 000 participants) provided sufficient statistical power to overcome the first limitation. Reliance on diagnoses from death certificates may introduce both random and systematic errors. Random error would tend to diminish the study's power to detect associations, while systematic error could alter the distribution of events and perhaps the risk factor–disease relationships if the errors were related to exposure status. However, the consistency of our findings, that is, the significant relationships between current smoking and death (Table 5), tend to suggest that major systematic errors related to the coding of death from either cancer or ASCVD events were unlikely. The conclusion of the study is only limited to the special population who met the selection criterion such as those who received secondary health examination due to abnormality found in the first examination. Thus, the conclusion and result is likely to be overestimated.
In sum, this prospective study provides strong evidence that uric acid level is not an independent risk factor for death from all causes, but that diabetes interacts with uric acid to influence the risk of all-cause mortality. Future studies should focus not only on cross-validation of the findings of this study but also on finding a plausible physiological mechanism for this phenomenon.
Footnotes
Acknowledgements
The authors would thank the staff of the Korean National Health Insurance Corporation. This study was supported by a grant of the Korean Health 21 R&D Project, Ministry of Health & Welfare, Republic of Korea (HWP-00-GN-01–0001).