
Abstract
Study objective
The aim of the study was to evaluate the impact of a long-term (6-month) correct breathing stereotype on minute ventilation, capillary blood gases and acid-base balance in post-myocardial infarction patients.
Methods
Fifty-five men (age 57.2 ± 12.5) were examined 2 months later after myocardial infarction. Spirometry and assessment of acid-base balance and capillary blood gases were performed at rest and repeated after 10 days and 6 months. Breathing correction was taught over 5 days. A session for the control and maintenance of the correct breathing skills was hosted once a month (during the 6-month period).
Results
Changes of minute ventilation, capillary blood gases and acid-base balance were revealed in 55% of patients 2 months later after myocardial infarction. Twenty patients (group I) were randomly selected for breathing correction while 10 patients made up the control group (group II). After breathing correction minute ventilation significantly decreased (18.5 ± 5.5 versus 9.8 ± 2.5 l/min), oxygen ventilatory equivalent decreased (39.8 ± 5.2 versus 22.5 ± 3.8), partial pressure of blood carbon dioxide increased (33.2 ± 1.7 versus 44.2 ± 2.5 mmHg), plasma bicarbonate concentration augmented (19.1 ± 2.2 versus 24.5 ± 1.8mmol/l), base excess normalized (−2.90 ± 2.5 versus +1.3 ± 2.1 mmol/l), and pH shifted to more alkaline value (7.36 ± 0.01 versus 7.43 ± 0.02).
Conclusions
A long-term correct breathing stereotype improved respiratory function and could be an additional measure in rehabilitation programmes for post-myocardial infarction patients.
Introduction
Most of the physiological functions of the human body are related to respiratory function; there are the controlling central and peripheral nervous systems, the detoxicative capacity of the liver, the acid–base regulation function of the kidney, and the transport ability of the respiratory gases by the blood. Dysfunction of these systems induces a slight hyperventilation (HV) and a long-term compensated metabolic acidosis or respiratory alkalosis [1–3]. When concomitant diseases are absent, HV most often occurs in cases of increased excitability of the autonomic nervous system or states of recurrent anxiety, which may play some role in the pathogenesis of the ischaemic heart disease. The mechanisms of the respiratory regulation are still not sufficiently clear [2, 4].
The opinion becoming more pronounced in recent years is a denial of the concept of hyperventilation syndrome as a complex of signs and symptoms—HV itself is evaluated as a non-specific sign (like tachycardia) of many acute and chronic clinical conditions that can be benign, of moderate severity or life-threatening [4–6].
In the 1970s and 1980s, a great many publications and monographs [2, 7] appeared reporting biochemical research results on carbonic acid metabolism. They revealed an important impact of carbonic acid on biosynthesis and metabolic regulation processes, oxygen supply and the speed of reactions in the tricarboxylic acid cycle. But there has been no clinical evaluation of these findings over the past 20 years. The opinion of researchers and clinicians up to this time has been different in evaluating the position of HV in the cause-consequence chain of mental and somatic disturbances.
In chronic HV, increased respiration is rarely clearly visible [8]. Slight increases in the volume of breath (for example, up to 750 ml), even under conditions of normal respiration rate (15–17 per min), should be considered HV (750≤17 = 12750 ml/min) [9]. It has also been emphasized [10] that over-breathing, established during situations of mental stress, or disturbances of the dietary regime, retains a low level of partial carbon dioxide tension, even when the increase in the over-breathing is slight or occasional.
After long-term breathing correction, the partial pressure of carbon dioxide in the blood and concentration of bicarbonates in plasma and tissues increases [2, 3, 11–13], oxygen consumption also becomes better [13, 14]. This improves bio-energetic processes and biosynthesis in the cells [2, 7]. Our data revealed that using long-term (6-month) breathing correction in combination with lifestyle modification improved respiratory function and induced positive alterations in peripheral circulation and cardiac morphometric data in post-myocardial infarction patients—significantly reducing the long axes of the left and right atria, improving left ventricular systolic function and significantly increasing ejection fraction and decreased wall motion score index [13]. There are no data regarding the breathing pattern in post-myocardial infarction patients, especially in the initial stages of heart failure, when dyspnea and hyperventilation are not yet evident. The acid-base misbalance and metabolic aspect of the hyperventilation problem in post-myocardial infarction patients is also underestimated. Possibilities to turn round the perverse cycle and to achieve improvement in haemodynamics and oxygen consumption are more favourable in the initial stages of heart failure [10, 13].
The aim of the study was to evaluate the impact of a long-term (6-month) correct breathing stereotype alone (without lifestyle correction) on minute ventilation, capillary blood gases and acid-base balance in postmyocardial infarction patients in the initial stages of heart failure.
Patients and methods
Contingent of patients
The study was performed on a sample of 55 men (age 57.2 ± 12.5) 2 months after myocardial infarction (MI) with congestive heart failure of I–II functional classes (The NYHA Classification). In cases of moderate and severe heart failure (NYHA class III–IV), dyspnea increases and hyperventilation occurs more frequently and is more marked, but because of worsening haemodynamic changes, ventilation–perfusion mismatching increases and breathing correction is not so effective.
Baseline characteristics of patients
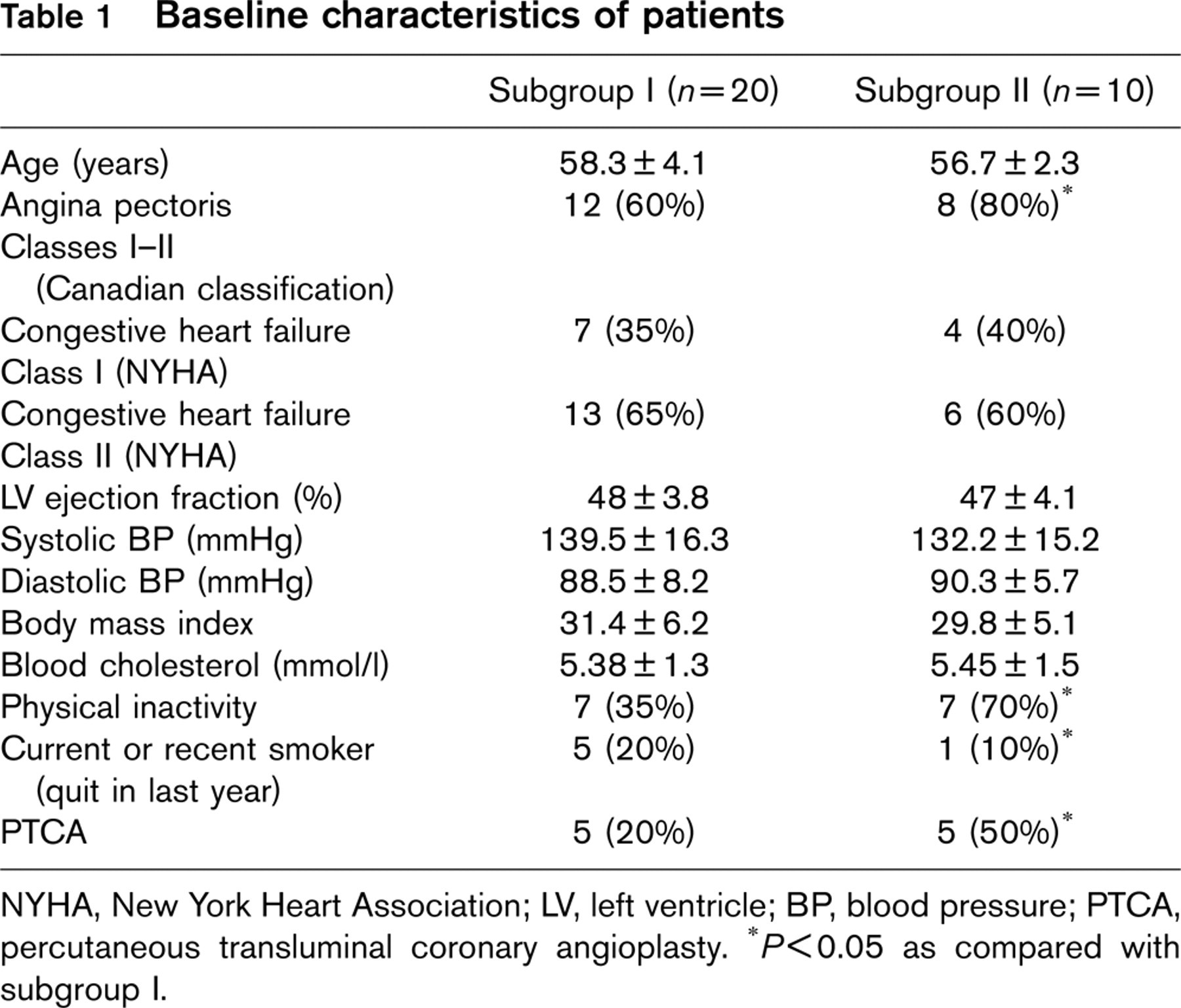
NYHA, New York Heart Association; LV, left ventricle; BP, blood pressure; PTCA, percutaneous transluminal coronary angioplasty. ∗ P < 0.05 as compared with subgroup I.
Medicamental therapies after myocardial infarction in subgroups I and II
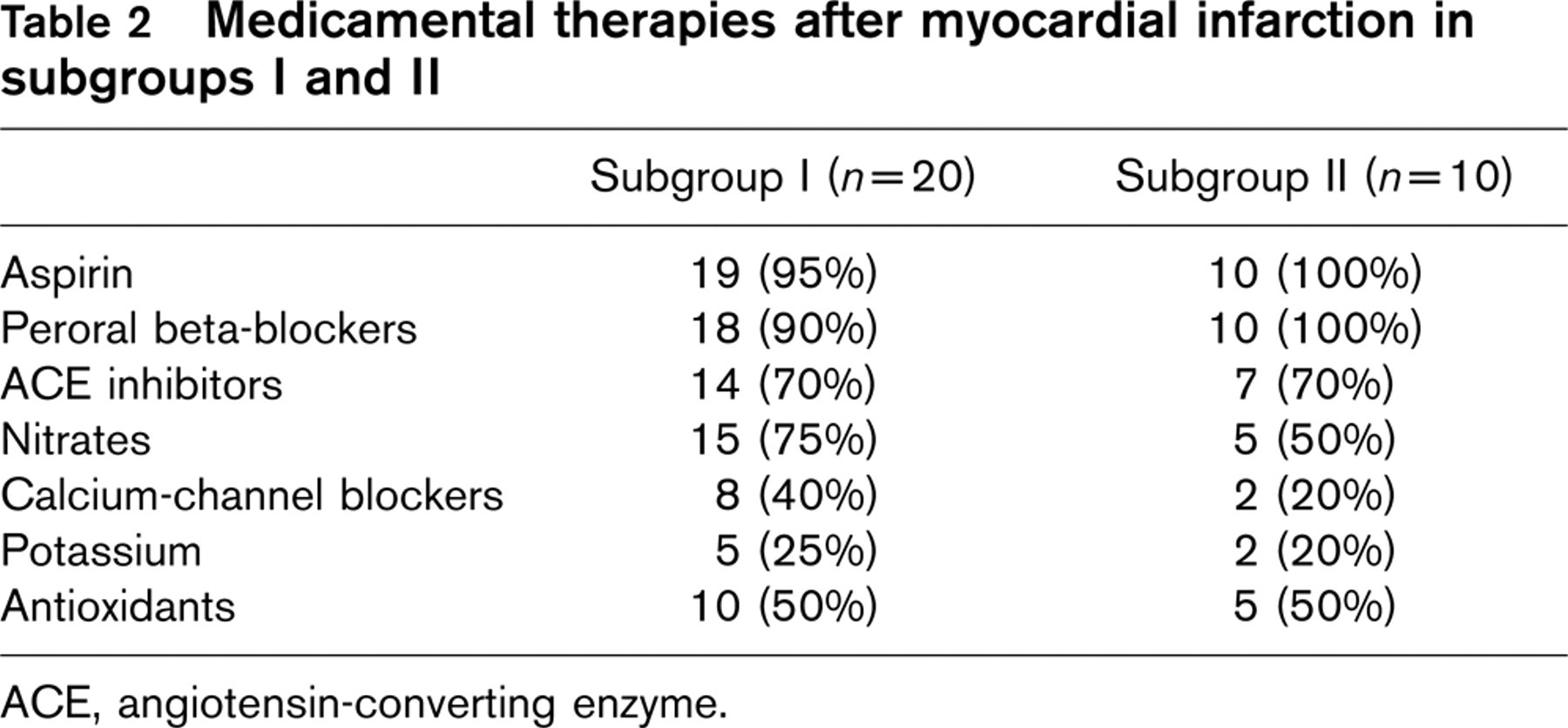
ACE, angiotensin-converting enzyme.
The state of one patient became worse, and he interrupted breathing practice. Baseline characteristics of patients are presented in Table 1. All the studied postmyocardial infarction patients received a standard drug treatment (Table 2).
The study did not include patients after coronary artery bypass surgery and cases with atrioventricular blockade, complicated rhythm disorders, unstable angina pectoris, stable angina pectoris (Canadian classification class III–IV), electrical pacing, congenital heart disease, bronchial asthma, obstructive pulmonary disease, diabetes mellitus, and other severe somatic or mental diseases.
Methods
Spirometry was performed at rest with a CS-200 Schiller spirometer. The breathing parameters of the stable interval were evaluated when mean values remained the same, and variation coefficient was 10%. For determination of hyperventilation, we used the following criteria:
Minute ventilation (MV) at rest ≤ 11 l/min.
Oxygen ventilatory equivalent (MV/VO2) ≤ 35.
Assessment of acid–base balance and capillary blood gases was performed with IL-System 1303 analyser. The tubes with blood specimens were washed up with heparin solution. The blood samples were kept in the ice thermostats and evaluated within a period of 1–2 h. For determination of hyperventilation, we used the following criteria:
Partial pressure of carbon dioxide (pCO2) in capillary blood <35mmHg.
Plasma bicarbonate concentration (HCO3 −) < 20mmol/l.
Spirometry, assessment of acid–base balance, and capillary blood gases were repeated after 10 days and 6 months.
Breathing correction
Breathing was corrected in accordance with the postulate that oxygen consumption at rest is better in case of slight hypoventilation, when pCO2 increases up to 60mmHg, pO2 decreases by not more than 60–70mmHg, minute ventilation decreases to 6–7 l/min [15]. Breathing retraining was taught in 5 days (six 15-min sessions per day). Once a month (during the 6-month period) a session was provided for control and maintenance of the correct breathing skills [13, 16]. Breathing correction by forming a correct breathing stereotype helps to prevent hyper-ventilation not only during breathing exercise but it also forms a long-term correct breathing pattern at rest. In this way, patients avoid time expenditure for breathing practice—they can breath correctly in their everyday life (TV watching, reading, writing, driving a car etc.), except in episodes of physical exertion.
Statistical analysis
Categorical data are presented as absolute values and percentages, whereas continuous data are summarized as mean value ± SD. Comparison of continuous variables was performed by means of Student's t-test. P values < 0.05 were considered statistically significant.
Results
Two months later after MI, assessment of spirometry, analysis of blood gases and acid–base balance were performed for the study patients. In 25 (45%) patients, respiratory function was normal; in 30 (55%) patients hyperventilation was established. Among the hyperventilated subgroup, 20 patients (subgroup I) were randomly selected for breathing correction, while the remaining 10 patients acted as controls (subgroup II).
Primary parameters of minute ventilation, capillary blood gases, acid–base balance, and their changes after 10 days and 6 months, compared with the initial parameters, are presented in Table 3.
In subgroup I (breathing correction) the average minute ventilation was 18.5 ± 5.5 l/min (14.3–25.4); and 20.3 ± 5.5 l/min (13.5–24.8) in the control subgroup (II). According to this parameter the groups did not differ significantly.
Compensated metabolic acidosis and compensated metabolic acidosis combined with compensated respiratory alkalosis were observed in the blood of 23 (75%) patients with over-breathing. In patients in subgroup I, oxygen ventilatory equivalent (MV/VO2) was elevated (35.2–48.3), partial pressure of blood carbon dioxide (pCO2) was reduced (28.2–35.2 mmHg), bicarbonate (HCO3 −) concentration was downgraded (17.1–20.4 mmol/l) and a lack of base (BE) (− 5.4 to + 0.5) was observed. Only in one patient was a positive (+) BE value established. The respiratory parameters of the controls did not differ significantly from the data of patients in subgroup I.
Parameters of minute ventilation, acid–base balance, capillary blood gases and their changes after 10 days and 6 months in patients from subgroups I and II
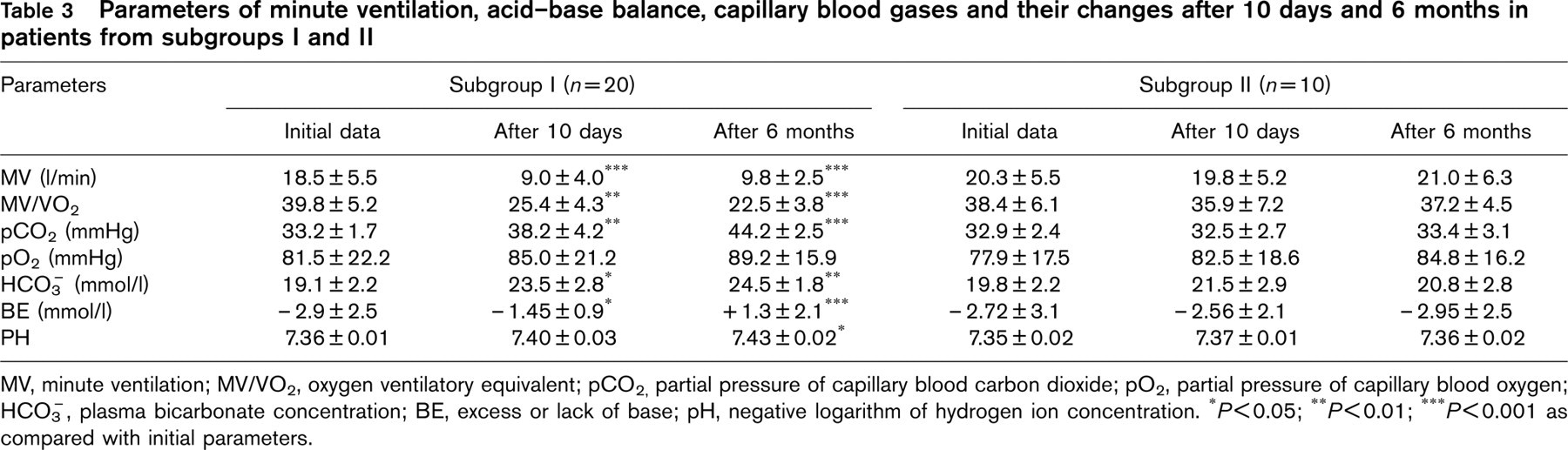
MV, minute ventilation; MV/VO2, oxygen ventilatory equivalent; pCO2, partial pressure of capillary blood carbon dioxide; pO2, partial pressure of capillary blood oxygen; HCO3, plasma bicarbonate concentration; BE, excess or lack of base; pH, negative logarithm of hydrogen ion concentration. ∗ P<0.05; ∗∗ P<0.01; ∗∗∗ P<0.001 as compared with initial parameters.
After 10 days' of breathing correction (Table 3), in the patients of subgroup I, MV decreased (7.2–12.9 l/min, P < 0.001), oxygen ventilatory equivalent (MV/VO2) decreased (18.2–35.4, P < 0.01), pCO2 increased (34.5–45.6 mmHg, P<0.01), HCO3 − augmented (20,8–25.9 mmol/l, P < 0.05), BE decreased (− 2.3 to + 1.2, P < 0.05]. Partial pressure of oxygen (pO2) in capillary blood did not differ significantly. Neither compensated metabolic acidosis nor respiratory alkalosis was established in any patient. Hypoventilation was also not observed.
After 6-month breathing correction, all differences of the above-mentioned respiratory parameters, compared with initial data, remained statistically significant. After 10 days and after 6 months, no statistically significant changes in minute ventilation and respiratory blood gases were noticed in the patients of the control subgroup (II).
Discussion
Some patient characteristics, which are presented in Table 1, differed between the groups. In our opinion, parameters that were not similar had no significant impact on the blood gases and acid–base balance. Inclusion and exclusion criteria are essential and define similar clinical conditions of the study contingent.
Being overweight did not differ significantly between the groups and there were no current smokers in either group (often after MI patients are scared enough to quit smoking, most when questioned had ‘quit in last year').
The impact of physical activity is under dispute, because physical exercise decreases hyperventilation and influences the acid–base balance. In both groups there was not a single patient who physically exercised. According to WHO recommendations (1999), physical inactivity is defined as physical activity equivalent to moderate walking of less 30 min per day. All patients admitted that their activity was only ‘daily physical activity'. Those, who were considered as physically active, stated, that although their daily life activity exceeded 30 min per day, they did not actually exercise. We supposed that such activity could not have any impact on the hyperventilation and acid–base balance.
Percutaneous transluminal coronary angioplasty (PTCA) could have an impact on the manifestation of angina pectoris, but in our study contingent we found more angina pectoris cases in the same group that was more often subjected to PTCA (subgroup II). It was not the aim of this study, but we found that due to the more effective breathing and better oxygen consumption (oxygen ventilatory equivalent decreased from 39.8 to 22.5), angina pectoris manifestation decreased from 60 to 30% in the subgroup I patients over the 6 months, while angina pectoris severity remained the same in 80% of the controls.
In post-myocardial infarction patients with heart failure, the spirometry and blood gas assessment have revealed deviation of respiratory function from normal parameters in 30 (55%) of our study population. In 23 (75%) of these patients, it manifested as compensated metabolic acidosis or compensated metabolic acidosis combined with compensated respiratory alkalosis. Carbon dioxide and bicarbonates change one into the other, rapidly and readily connecting or splitting-off the OH− group. The change of respiratory pattern rapidly changes concentration of carbon dioxide and bicarbonates in the body. As it is known, carbon dioxide and bicarbonates form the main buffer system regulating acid–base balance, whereas acid–base imbalance exerts important influence on the activity of many enzymes and the speed of biochemical reactions.
Theoretical premises [2, 7, 17] allow affirmation that, in cases of higher concentration of carbon dioxide and bicarbonates in the cells, carboxylation—addition of CO2 to an organic acceptor to yield a carboxyl (– COOH) group—is increased. Carboxylation reactions are essential in the synthesis of important metabolic products—the formation of albumin (synthesis of purine and pyrimidine bases, formation of adenosine triphosphate), biosynthesis of carbohydrates (pyruvate carboxylation and the formation of the dicarboxylic acids for the Krebs cycle) and fats (the initial state of synthesis of the fatty acids; acetyl coenzyme A carboxylation). If the concentration of carbon dioxide in the cells is adequate, reactions in the Krebs cycle accelerate, and cellular energy supply improves [2, 7]. Hypocapnia is an unfavourable factor in patient's rehabilitation and recovery as it impairs biosynthesis of cellular microstructures [2, 7], and worsens delivery of oxygen from microcirculation to mitochondria [14].
Our data did not reveal whether the compensated metabolic acidosis observed in post-myocardial infarction patients existed before MI. According to the literature [1, 2, 4, 18], slight metabolic acidosis is a quite frequent state in the human body. This was also confirmed by our investigation. Such metabolic acidosis can be easily corrected. Literature data show that in patients with heart disorders the impact of over-breathing is commonly investigated by short-term HV tests on coronary circulation, recording of electro- and echo-cardiograms, and performing Holter's monitoring [19–21, 24]. Hyperventilation induces spasm of coronary arteries, ventricular tachycardia [21, 22], mainly by activating the sympathetic nervous system [4, 23]. Low plasma bicarbonate concentration can predispose impairment of peripheral circulation [20, 22]. So, lack of carbon dioxide and plasma bicarbonates as well as increased activity of the sympathetic nervous system may cause spasms of the coronary arteries and complicate the course of ischaemic heart disease (IHD) [24]. During the workload testing, these patients had more increased double product and heart rate [24], and they presented more health complaints [4, 12]. Transcranial Doppler sonography and MR showed blood flow deterioration not only in coronary arteries, but also in the middle cerebral artery—during hyperventilation, blood flow decreased by 49.6% [10, 21].
A long-term breathing correction and formation of a correct breathing stereotype regulates acid–base balance and reduces or eliminates neurological and cardiological symptoms and signs [5, 11, 12, 20, 23]. Our data show that even after 10 days of breathing correction, minute ventilation and oxygen ventilatory equivalent decreased, partial pressure of carbon dioxide increased, lack of base normalized, and pH shifted to a more alkaline value. During the 5-day period patients were trained to correct their breathing by forming a new stereotype. Later we only observed whether their breathing remained correct, and whether the new stereotype worked. We found, that after 6 months the newly formed correct breathing stereotype remained unchanged, and that the altered breathing parameters still remained beneficial. Patients were encouraged to breathe correctly all the time and after the 6-month period. We believe, that only long-term breathing correction will produce a positive impact on the metabolism [4, 5, 7].
Conclusions
A long-term correct breathing stereotype improved the respiratory function and it could be an additional measure in rehabilitation programmes for post-myocardial infarction patients in the initial stages of heart failure. Five days' of retraining (with sessions once a month) are sufficient to acquire and maintain the correct breathing skills. Breathing correction, at relatively low cost, should therefore be taken into consideration while planning and arranging cardiac rehabilitation programmes.
Footnotes
Acknowledgements
This article forms part of an unpublished section of doctoral thesis (Impact of the correct breathing stereotype and changes of lifestyle on the cardiovascular system in patients after myocardial infarction) by Dr. Lina Jasiukevičienė, Kaunas, 2002. The work was done with the equipment of the Department of Cardiology, Kaunas University of Medicine Hospital.