
Abstract

Intervention strategies: 1. Predictors of awareness for hypertension and hypercholesterolaemia after medical screening in a sample of hypertensive/hypercholesterolaemic subjects
Françoise Leynena, Els Claysb, France Kittela, Guy De Backerb, Marcel Kornitzeraa
aDepartment of Epidemiology and Health Promotion, School of Public Health, Brussels Free University, bDepartment of Public Health, Ghent University, Brussels.
Background Previous analyses on the Belstress cohort have shown a positive association between awareness of hypertension (HT)/hyper-cholesterolaemia (HC) and sick-leave incidence, as an inverse measure of the quality of life. In the present analyses we want to investigate possible predictors for awareness, 5 years after a medical screening examination, in subjects, previously unaware of their condition, who were diagnosed as hypertensive or hypercholesterolaemic at baseline.
Methods From the 25 companies that participated in Belstress I, nine companies were selected for a second survey, resulting in a total Belstress II sample of 1950 males and 871 females. In order to examine the evolution of awareness of HT and HC between the first and the second survey, only hypertensive (∗systolic blood pressure ≤140mmHg or diastolic blood pressure of ≤ 90mmHg or being under treatment)/hypercholesterolaemic subjects (∗∗serum cholesterol level ≤ 200 mg% or being under treatment), unaware of there condition at time1 (Belstress I) where withheld for analyses. Awareness was defined as answering ‘yes' to the question ‘Did a physician ever inform you that your blood pressure/cholesterol level was too high?'.
Results From the 35.5% male and 26.1% female hypertensives, respectively 61.3/45.1% were unaware at time 1, resulting in a total sub-sample of 495 subjects eligible for analyses on awareness of HT. Parallel to this, from the 70.8% male and 66.7% female hypercholes-terolaemics, respectively 68.5/85.3% were unaware, resulting in a sub-sample of 1363 subjects.
I. For awareness of HT. In univariate analyses, a significant higher incidence of awareness at time 2 was observed in females and close to statistical significance in older subjects, in subjects with job strain, in French-speaking subjects, in obese subjects, in depressive subjects and in those with intermediate educational levels and with an intermediate job function. When all previous variables, plus systolic blood pressure (SBP) were introduced in a multivariate logistic regression model, gender, SBP and BMI remained independent predictors of awareness with OR's of 2.20 (1.28–3.78)∗∗, 1.03 (1.02–1.04)∗∗∗ and 1.70 (0.92–3.14), for female gender, increase in SBP of 1mmHg and BMI ≤ 25kg/m2 respectively.
II. For awareness of HC. In univariate analyses, significant higher levels of awareness at time 2 were observed in males, in older subjects and in Dutch-speaking subjects. Borderline significant higher levels were observed in subjects with job strain, in subjects with a higher educational level and a higher job level. In a logistic regression model, including all previous variables as well as baseline cholesterol level; age, language, occupation and cholesterol level remained independent predictors of awareness with OR's of 1.49 (1.13–1.96)∗∗, 0.61 (0.43–0.85)∗∗, 0.62 (0.44–0.86)∗∗ and 1.009 (1.005–1.013)∗∗∗ for older age, French speaking, intermediate job levels and increase in serum cholesterol of 0.026 mmol (1mg)% respectively.
Conclusion Awareness of hypertension does not seem to be predicted by the same variables as awareness of hypercholesterolaemia. Remarkable findings are the opposite associations observed for gender and socio-economic status. Awareness of hypertension is higher in females and in lower socio-economical levels, whereas for awareness of hypercholesterolaemia, the opposite is true. Further investigations in order to explain these differential findings could be useful in the context of health promotion.
Diet and physical activity: 2. Dietary fat and risk of coronary heart disease: possible effect modification by gender and age
Marianne Uhre Jakobsena,b, Kim Overvadc, Jøen Dyerbergd, Marianne Schrolla,b, Berit Heitmanna
aResearch Unit for Dietary Studies and Danish Epidemiology Science Centre at Institute of Preventive Medicine, Copenhagen University Hospital, bResearch Centre for Prevention and Health, Glostrup University Hospital, cDepartment of Clinical Epidemiology, Aalborg Hospital and Aarhus University Hospital, and Department of Epidemiology and Social Medicine, University of Aarhus, dDepartment of Human Nutrition, Royal Veterinary and Agricultural University, Denmark.
Background Results from studies of dietary fat and risk of coronary heart disease (CHD) are inconsistent, potentially due to effect modification by gender and age. We did a prospective cohort study in order to examine the association between energy intake of dietary fat and the risk of CHD while assessing the role of gender and age.
Methods As part of the Glostrup Population Studies, 3686 middle-aged men and women without previous CHD were enrolled between 1974–1993. Dietary intake was assessed at baseline using a 7-day weighed food record. Over 16 years of follow-up, 326 participants with fatal or non-fatal events of CHD were identified. In the models used, total energy and protein intake were fixed. Differences in intake of energy from fat thus reflected complementary differences in intake of energy from carbohydrates.
Results A 5% higher level of energy from saturated fat intake was associated with a 36% greater risk of CHD among women (multivariate adjusted HR = 1.36, 95% CI: 0.98–1.88). No overall association between saturated fat and CHD was found among men. However, age dependent analyses showed that saturated fat was positively associated with CHD among the younger men (multivariate adjusted HR=1.29, 95% CI: 0.87–1.91) and the younger women (multivariate adjusted HR=2.68, 95% CI: 1.40–5.12) but not among the older men and the older women. Polyunsaturated fat was inversely associated with CHD among women and men, but not significantly.
Conclusion The present study suggests that CHD risk relates both to the quantity and the quality of dietary fats.
Diet and physical activity: 3. Does autonomic function link social position and coronary risk? The Whitehall II study
Harry Hemingwaya, Martin Shipleya, Eric Brunnera, Annie Brittona, Marek Malikb, Michael Marmota
aInternational Centre for Health and Society, Department of Epidemiology and Public Health, University College London Medical School, London, bDepartment of Public Health Research, Westminster Primary Care Trust, London, cCardiological Sciences, The Medical School, St. George's Hospital, London, UK.
Background Laboratory studies of animals and humans suggest that the autonomic nervous system mediates the relation between low social position and high coronary risk. We sought to test this hypothesis in a population study.
Methods A total of 2197 male civil servants aged 45–68 years in the Whitehall II study undergoing standardised assessments of social position (employment grade), and the psychosocial, behavioural and metabolic risk factors for coronary disease, previously found to be associated with low social position. Five minute recordings of heart rate variability (HRV) were used to assess cardiac parasympathetic function (standard deviation of N–N intervals [SDNN] and high frequency power [HF, 0.15–0.40 Hz]) and the influence of sympathetic and parasympathetic function (low frequency power [LF, 0.04–0.15 Hz]).
Results Low employment grade was associated with low HRV (P for trend for each modality ≤ 0.02). Behavioural factors (smoking, exercise, and alcohol), psychosocial factors (job control) and components of the metabolic syndrome (waist:hip ratio, systolic blood pressure, High density lipoprotein cholesterol, triglycerides and 2 hour post-load glucose) each showed strong, linear associations with low HRV (P <0.01). The age adjusted prevalence of low job control was 21.8% in the bottom quartile of LF power, decreasing to 12.1% in the top quartile (P for linear trend 0.006). A total of 42% of the employment grade differences in LF power were explained by the metabolic syndrome and behavioural factors; adding job control to this model increased the explanation to 59%. Conversely, 23% of the employment grade differences in MS were explained by LF power.
Conclusion Chronically impaired cardiac autonomic function may link social position to different components of coronary risk in the general population.
New risk factors: 4. Do factors in the psychosocial work environment mediate the effect of socio-economic position on the risk of myocardial infarction?
Ingelise Andersena, Hermann Burrb, Tage S. Kristensenb, Michael Gamborga, Merete Oslerc, Eva Prescotta,d, Finn Diderichsenc
aCopenhagen Centre for Prospective Population Studies, Danish Epidemiology Science Centre, at the Institute of Preventive Medicine, H:S Kommunehospitalet, Copenhagen University Hospital, Copenhagen, bNational Institute of Occupational Health, Copenhagen, cCopenhagen Centre for Prospective Population Studies, at the Institute of Public Health, Copenhagen University, Copenhagen, dDepartment of Cardiology, Rigshospitalet, Copenhagen, Denmark.
Background Studies from a broad range of countries during the latest 40 years have consistently shown that the risk of coronary heart disease is lowest in positions with greatest social and economic advantage, and highest in the most disadvantaged groups. The effect of social position on myocardial infarction (MI) has been shown to be mediated by several known biological, behavioural and psychosocial risk factors. Most studies, however, have found that adjustment for a number of potentially mediating biological and behavioural risk factors reduces the excess risk among manual occupations to only 20–50%. If psychosocial exposures are included in the model, a similar proportion seems to be mediated by those causes. Several studies have found that the psychosocial conditions at the work place are particularly important. The aim of this study is to investigate whether the effect of socio-economic position on risk of MI is mediated by differential exposure or differential susceptibility to psychosocial work environment.
Methods We used data from three prospective population studies conducted in Copenhagen. A total of 16,214 employees, 44% women, aged 20–75 years, with initial examination between 1974 and 1992 were followed until 1996 for incident (hospital admission or death) MI. We used register-based information on job-categories. Psychosocial job exposures were measured indirectly by means of a job exposure matrix based on the 1990 Danish Work Environment Cohort Study. The association between risk factors and incidence of MI was analysed using Cox's proportional hazards regression models, with age as underlying time scale.
Results During follow-up, 731 subjects were diagnosed with an MI: 610 men, 121 women (35% fatal). The hazards by socio-economic position showed a graded effect with a hazard ratio (HR) of 1.57 (1.23–2.03) for unskilled workers as compared to executive managers. Despite a strong and graded association in risk of MI related to decision authority and skill discretion, only skill discretion mediated the effect of socio-economic position. The HR for unskilled workers was reduced to 1.47 (0.93–2.31) after adjustment for decision authority and other cardiovascular risk factors, and to 1.07 (0.72–1.60) after adjustment for skill discretion and cardiovascular risk factors. No sign of synergy was found.
Conclusion Decision authority and skill discretion were strongly related to socio-economic position; the effect on risk of MI was partially mediated by skill discretion. Improvements in psychosocial work environment, especially possibilities for skill discretion, might contribute to reducing the incidence of MI and social inequality in MI.
New risk factors: 5. The impact of depression and Type D personality on cardiac prognosis following percutaneous coronary intervention: Type D personality is more than just depression
S. S. Pedersena,b, P. A. Lemosa, P. R. van Voorena, R. A. M. Erdmana, P. C. Smitsa, P. W. Serruysa, R. T. van Domburga
aDepartment of Cardiology, Thorax Centre, Erasmus Medical Centre Rotterdam, Rotterdam, bDepartment of Psychology and Health, Tilburg University, The Netherlands.
Background Depression and the distressed personality type (Type D) have both been associated with adverse clinical outcome in patients with established heart disease. Whereas depression has gained risk factor status, Type D has been criticized for being nothing more than a variant of depression or ‘old wine in new bottles'. We investigated the relative impact of anxiety and depressive symptoms versus Type D personality on the occurrence of adverse events 9 months following percutaneous coronary intervention (PCI) with either sirolimus-eluting stents (SES) or bare stents.
Methods In a sub-study of the Rapamycin Eluting Stent Evaluated At Rotterdam Cardiology Hospital (RESEARCH) registry, 875 consecutive patients with ischaemic heart disease filled in the Hospital Anxiety and Depression Scale and the Type D Personality Scale 6 months following PCI. This time point was chosen in order not to burden patients at the time of intervention. The primary endpoint was a composite of death (all-cause) and non-fatal myocardial infarction (MI). Events occurring prior to administration of the questionnaires were excluded from analyses.
Results At 9 months following administration of the psychological questionnaires, there were nine deaths and 11 MIs. Anxiety, depressive symptoms, and Type D were all separately independent predictors of death or MI. Anxiety lost its significance in conjunction with depressive symptoms and Type D personality, respectively. The model that best predicted outcome contained depressive symptoms (HR = 2.14; P = 0.145) and Type D personality (HR = 4.02; P= 0.010) adjusting for all demographic and clinical factors. As indicated by the −2 log likelihood statistics, adding depressive symptoms to a model comprising demographic and clinical risk factors substantially increased the level of prediction of outcome (P= 0.005). The addition of Type D personality to this model further improved the level of prediction (P < 0.001).
Conclusion This is the first study to investigate the relative impact of anxiety and depressive symptoms versus Type D personality on clinical outcome in the drug-eluting stent era in patients following PCI. Our results showed that Type D personality is more than just anxiety and depressive symptoms and that it may be a risk factor on a par with depression.
New risk factors: 6. Circulating oxidized LDL and risk of myocardial infarction in well-functioning elders in the Health ABC cohort
Paul Holvoeta, Stephen B. Kritchevskyb, Russell P. Tracyc, Ann Mertensa, Susan M. Rubind, Javed Butlere, Bret Goodpasterf, Tamara B. Harrisg, for the Health ABC study
aCentre for Experimental Surgery and Anaesthesiology, Catholic University, Belgium, bSticht Centre on Aging, Wake Forest University School of Medicine, Winston-Salem, NC, cDepartments of Pathology and Biochemistry, University of Vermont, Burlington, VT, dUniversity of California, Prevention Sciences Group, San Francisco, CA, eVanderbilt University, Nashville, TN, fDepartment of Medicine, University of Pittsburgh, PA, gLaboratory of Epidemiology, Demography and Biometry, National Institute on Aging, NIH, Bethesda, USA.
Background We have shown in the Health ABC cohort, a relation between high-predicted coronary heart disease (CHD) risk prior to CHD events and high levels of circulating oxidized low-density lipoprotein (LDL) even after adjustment for LDL-cholesterol. High-predicted CHD risk was defined according to the Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATPIII) (Arterioscler Thromb Vasc Biol 2003, 23:1444–1448). Our objective was to establish the relation between oxidized LDL (oxLDL) and risk for myocardial infarction (MI) in this cohort.
Methods Baseline levels of oxLDL were measured in plasma from 3,033 participants in the Health ABC study (50% women, 42% Black, aged 70–79 years). Since enrolment (follow-up: March 1997 through to June 2002), 120 persons had an incident MI. The relative risk (RR) of MI according to oxLDL (continuous variable, log-transformed, or per quintile) was determined by logistic regression analysis adjusting for age, gender, race, smoking, and LDL-cholesterol.
Results Levels of oxLDL predicted MI risk (RR: 2.94; 95% CI: 1.25–6.96). The incidence of MI was 5.7% in the highest quintile of oxLDL compared to 2.6% (P <0.01) in the lowest quintile. The adjusted RR for participants in the highest quintile was 2.25 (95% CI: 1.22–4.15). After further adjustment for all metabolic syndrome components, defined according to ATPIII, RR for persons in the highest quintile of oxLDL was 1.87 (1.00–3.49). Whereas persons with the metabolic syndrome had significantly higher levels of oxLDL, there was no significant interaction between MS and oxLDL suggesting that the effect of oxLDL on MI was independent of MS.
Conclusion Oxidized LDL predicts risk of myocardial infarction in well-functioning elders even after adjustment for metabolic syndrome. Funding: N01-AG-6–2101; N01-AG-6–2103; N01-AG-6–2106; the Interuniversitaire Attractiepolen Programma of the Belgian Federal Government (P05/02).
High risk/traditional risk factors: 7. Overweight, body composition and cardiovascular responses
Hans W. Hensea, Angela Doeringb, Heribert Schunkertc
aInstitute of Epidemiology and Social Medicine, University Muenster, bInstitute of Epidemiology, GSF National Research Centre, Neuherberg, cClinic for Internal Medicine II, University Schleswig-Holstein, Campus Luebeck, Germany.
Background Obesity is a highly prevalent precursor of cardiovascular disease. However, the specific mechanisms underlying the cardiovascular sequelae of obesity are not fully understood. We hypothesised that the amount of adipose and fat-free mass may differentially determine cardiovascular responses.
Methods Men and women, age 25–74 years, were examined in a population-based survey of the MONICA Augsburg study in 1994/95. Two-dimensional echocardiography with optimal visualisation of the endocardium was used to determine ventricular volumes and cardiac output. High-quality recordings were available for 371 men and 467 women. Fat-free and adipose mass were assessed employing bioelectrical impedance analysis. Cardiac and blood pressure measurements were compared between groups using multivariate linear regression.
Results The age-sex-adjusted mean fat-free mass in normal, overweight and obese subjects was 48.3, 52.0, and 54.9 kg and the respective mean adipose mass was 15.6, 23.9, and 33.7 kg (P<0.001). Regression analysis confirmed the expected significant rises of systolic and diastolic blood pressure (P <0.001), of stroke volume (P=0.02) and of cardiac output (P <0.001) across the three BMI groups. Interestingly, additional adjustment for fat-free and adipose mass completely eliminated the differences in cardiac output and blood pressure. Of note, fat-free mass contributed significantly (P =0.002) to the attenuation of the differences in cardiac output whereas adipose mass contributed significantly (diastolic P =0.002; systolic P =0.015) to the elimination of the effect on blood pressure.
Conclusion The elevation of cardiac output in overweight and obesity was explained by raised fat-free mass, while, by contrast, only adipose mass accounted for the increase in blood pressure. Fat-free mass represents those compartments of the body that require most of the circulatory blood supply. Our data suggest that gains in body weight result in physiologically adequate increases of cardiac output due to raised fat-free mass indicating a relevant role of non-adipose tissue for the haemodynamics of obesity. The assessment of body composition may deserve a stronger focus in the management of obese patients.
High risk/traditional risk factors: 8. Predictors of one year sick-leave, an indicator of well-being, using a total cardiovascular risk estimate
M. Moreaua, D. De Bacquerb, E. Claeysb, F. Leynena, G. De Backerb, M. Kornitzera
aDepartment of Epidemiology and Health Promotion, School of Public Health, Université Libre de Bruxelles, bDepartment of Public Health, Ghent University, Ghent, Belgium.
Background Several epidemiological studies have shown positive association between coronary risk factors such as obesity or smoking habits and absenteeism whereas some other risk factors are not associated with sick-leave (total cholesterol, high-density lipoprotein [HDL]-cholesterol, hypertension). As risk factors interact to produce their total risk, it is more and more recommended to use a global risk. The purpose of this study is to test the predictability of a global cardiovascular risk score on absenteeism due to illness among workers independently from major confounding factors.
Methods Between 1994–1998, 16,335 male and 5084 female volunteers, aged 35–59 from 23 Belgian companies, completed a questionnaire and underwent a clinical screening at the beginning of the study. Percentile 75 (P 75) of the distribution of the total number of absent days (12 and 15 days for men and women respectively) was used as cut-off to classify the workers with a high or low sick leave incidence. The frequency of short sickness absence (≤ 7 days) (no spells versus one or more short spells), the frequency of long sickness absence (≤ 28 days) (no absence versus one or more absences of 28 days or more) as well as the frequency of medium spells (spells between 7 and 28 days) were also used as additional endpoints. A global cardiovascular risk score based on age, total cholesterol, smoking and systolic blood pressure was computed for males and females and categorised in quartiles. The coronary heart disease status was assessed by ECG using the Minnesota code. Multiple logistic regression was relied upon to select predictive factors of sick-leave using a backward procedure based on the likelihood ratio. The variables entered initially in the logistic regression equation were age, global cardiovascular risk, waist circumference, occupational and education level, presence of diabetes, physical activity, fibrinogen, HDL-cholesterol, coronary heart disease status and alcohol consumption.
Results After adjustment for variables selected with the backward procedure, we found significant odds ratios (OR) for medium and long spells in men and for high sick-leave incidence and medium spells in women. Thus compared to workers in the first quartile of the global score risk, workers in the highest quartile have an adjusted risk of having medium and long spells of 1.29 (P <0.0001) and 1.33 (P <0.009) in men respectively. Compared to workers in the first quartile of the global score risk, females workers in the highest quartile have an adjusted risk of having a high sick-leave incidence and medium spells of 1.75 (P <0.006) and 1.59 (P <0.0001) respectively.
Conclusion These findings indicate that a global cardiovascular risk score, besides predicting incidence of cardiovascular diseases, is an independent predictor of sick-leave, and a good marker of quality of life.
High risk in the Italian population: 9. Stroke risk in the Italian population
Simona Giampaolia, Luigi Palmieria, Marco Ferrariob, Salvatore Panicoc, Lorenza Pilottod, Diego Vanuzzod, Jeremiah Stamlere
aCentro di Epidemiologia, Sorveglianza e Promozione della Salute, Istituto Superiore di Sanità, Rome, bDipartimento di Scienze Cliniche e Biologiche, Università degli studi dell'Insubria, Varese, cUniversità degli studi Federico II, Napoli, dCentro per la Prevenzione Cardiovascolare, Azienda Socio-Sanitaria 4 Medio Friuli and Agenzia Regionale della Sanità, Udine, Italy, eFeinberg School of Medicine, North-western University, Chicago, USA.
Background For decades Italy has evoked research interests because of its lower coronary heart disease mortality rates, a phenomenon widely attributed to the ‘Mediterranean diet'. But throughout these years Italy has experienced higher stroke mortality rates, a neglected adverse public health finding. The purposes of this study are to estimate incidence of stroke in the Italian general population, to evaluate impact of multiple risk factors, and potential for stroke prevention.
Methods A 10-year prospective study of 10 cohorts (Progetto CUORE) 7,477 men and 7,989 women baseline ages 35–69, free of stroke at baseline, followed through to December 1998; standardized validation of suspected non-fatal and fatal strokes based on MONICA diagnostic criteria.
Results Age-adjusted incidence rates were 23 per 10,000 person-years in men, 14 in women. Age, gender, blood pressure, need for hypertension medication, smoking, fasting glycaemia, diabetes, total cholesterol/high-density lipoprotein cholesterol (HDL-C), personal history of myocardial infarction and family history of cardiovascular disease were independently related to stroke risk. No strokes occurred in persons with favourable levels of all risk factors and none occurred in persons with borderline elevation of one risk factor of four (systolic blood pressure 121–139 mmHg, diastolic 81–89 mmHg, total cholesterol 200–239 mg/dl, BMI 25–29kg/m2).
Conclusion The Progetto CUORE study, with the first data on stroke incidence in the Italian adult general population, showed that blood pressure, smoking, glycaemia, diabetes, serum lipids, all preventable and controllable, are significantly independent risk factors for stroke. Prevention in the general population should be implemented and directed especially to improving life styles.
Settings: 10. A randomised non-pharmacological intervention study for prevention of ischaemic heart disease—Inter99
Torben Jørgensena, Knut Borch-Johnsenb, Frølund Thomsen Troelsa, Charlotta Pisingera, Hans Ibsenc
aResearch Centre for Prevention and Health, bSteno Diabetes Centre, cMedical Department M, Glostrup University Hospital, Denmark.
Background There is limited knowledge on the effect of systematic long-term interventions in population-based screening and non-pharmacological intervention for prevention of ischaemic heart disease (IHD).
Methods The study population comprised 61,301 persons. A random sample of 13,016 persons were invited for a risk assessment for IHD by means of a computer program (PRECARD®). The remaining 48,285 served as reference population. According to predefined criteria participants were classified into a high risk and a low risk group. The 13,016 persons were a priori randomised to receive a low or a high intensity intervention. Intervention focused on smoking, physical activity and diet. Interventions were made in three waves (at baseline, after 1 year, and after 3 years). Spontaneous changes in lifestyle in the reference population were monitored by questionnaires. Effects were calculated as change in lifestyle habits, biological risk factors, and absolute risk of IHD.
Results One year follow-up is presented. Participation rate at baseline was 52% (n = 6,784). A total of 60% fulfilled the criteria for lifestyle intervention. In the high intensity intervention group nearly half accepted group-based intervention. A total of 62% of the high-risk population was re-examined after one year. Significantly more persons in the intervention groups stopped smoking compared to the reference population. Systolic blood pressure, low-density lipoprotein-cholesterol, and risk of IHD decreased significantly in the high compared to the low intensive intervention group (P<0.05). Changes in BMI, waist circumference, and total cholesterol all showed a non-significant trend in favour of the high intensity intervention group.
Conclusion The present study shows a positive effect of population-based screening and intervention after 1 year.
Closing the gap: 11. Attitudes of physicians towards the treatment of risk factors in patients with CHD: how do physicians comply with clinical guidelines? Results from the COSIMA study
Ulrich Keil, Jan Heidrich, Friederike Raspe, Edith Siebert, Thomas Behrens
Institute of Epidemiology and Social Medicine, University of Münster, Germany.
Background The EUROASPIRE I and II surveys have shown a persistent gap between evidence-based guidelines on secondary prevention of coronary heart disease (CHD) and their implementation in clinical practice. The aim of the COSIMA (Coronary secondary prevention in the Münster area) study is to identify factors explaining the observed gap in the EUROASPIRE region of Münster.
Methods To achieve its aim COSIMA applies a physician and patient survey. We report here on the results from the physician survey. In 2002, a postal questionnaire with questions on knowledge and attitudes towards guidelines on secondary prevention of CHD was sent to all general practitioners (GP) and internists working in private practice in the region of Münster (n = 1,023). The impact of socio-demographic factors, specialty, duration of medical practice and characteristics of private practice were assessed using multivariate logistic regression.
Results In total, 681 physicians participated in the survey with 58% of physicians claiming a good or very good knowledge of the guidelines of the German Society of Cardiology, whereas the respective ESC guidelines were much less known (15%). Generally, physicians rated the treatment of risk factors such as smoking (94%), hypertension (90%), diabetes (84%), hypercholesterolaemia (71%) and being overweight (69%) as very important. With regard to smoking cessation, however, the importance of behavioural therapy and nicotine replacement therapy (NRT) was acknowledged as very important by only 17% and 5% of physicians, respectively. A total of 36% of physicians reported starting anti-hypertensive drug treatment at a systolic blood pressure of > 150 mmHg and 38% of physicians stated starting drug treatment only at total cholesterol values of ≤ 250 mg/dl or low-density lipoprotein-cholesterol (LDL-C) values of ≤150 mg/dl. Internists were more likely to start drug treatment of hypercholesterolaemia at a LDL-C level ≤ 100 mg/dl (OR 1.39; 95% CI: 0.95–2.05) and drug treatment of hypertension at systolic blood pressure ≤ 140 mmHg (OR 1.42; 95% CI: 1.0–2.02) as compared to general practitioners.
Conclusion In general, physicians expressed positive attitudes towards the usefulness of guidelines. However, the need for vigorous treatment of risk factors, such as smoking, hypertension, and hypercholesterolaemia in patients with CHD was grossly underrated. Our findings provide physician-related explanations for the persisting gap between guidelines and treatment of risk factors in the Münster region. Stronger emphasis has to be put on information dissemination and the continuous medical education of physicians to ensure higher standards of knowledge on recent developments in evidence based medicine.
Closing the gap: 12. Comparison of three hospital-based rehabilitation programmes for patients with acute coronary syndrome
I. Willainga, A. Helms Andreasena, T. Jørgensena, J. Rokkedalb
aResearch Centre for Prevention and Health, Glostrup University Hospital, bGlostrup University Hospital Medical Department, Glostrup, Denmark.
Background The literature clearly documents the positive effects of rehabilitation following acute coronary heart disease. This study compares the effects and costs of three different well-established rehabilitation programmes for patients admitted with acute coronary syndrome in three cardiology departments in the Copenhagen area.
Methods Over 1 year (2001–2002) 998 patients (aged 31–99) were included consecutively. Patients were offered a follow-up consultation in the hospital after 1 year. Data on the disease and treatment were registered and patients answered questionnaires on lifestyle, co-morbidity, social status, health-related quality of life (HRQoL, SF 36), and hospital stay and rehabilitation programmes. Statistical methods include logistic and linear regression analysis. A cost-effectiveness analysis will be performed.
Results At baseline there were no significant differences between the three populations in relation to severity of disease, co-morbidity, lifestyle, and HRQoL. Sex and age differed significantly (P =0.0003 and P<0.0001). Patients were significantly more satisfied with the hospital stay at one of the hospitals. At follow-up there were significant differences in mortality in a crude analysis, but not after adjustment. Changes in systolic blood pressure, blood lipids, blood glucose, lifestyle, SF 36, and rate of re-admission did not differ significantly. Patient-reported data on rehabilitation programmes offered indicated very few significant differences.
Conclusion The three rehabilitation programmes apparently have relatively similar effects on health and quality of life. However, because of suspected selection bias at follow-up sensitivity analyses must be performed as well as comparison with data from central registers.
Diabetes: 13. A comparison of risk estimation systems and simple physical measurements in predicting the metabolic syndrome
T. Leonga, Y. Rahmanb, A. P. Fitzgeraldc, S. Storeya, L. Taylora, P. Gaffneyd, G. Borand, V. Mahera, J. Nolanb, I. M. Grahama
aDepartment of Cardiology, Adelaide and Meath Hospital, Dublin 24, bDepartment of Endocrinology, St. James's Hospital, Dublin 8, cThe Haughton Institute, Dublin 8, dDepartment of Clinical Chemistry, Adelaide and Meath Hospital, Dublin 24, Ireland.
Background The metabolic syndrome increases cardiovascular disease (CVD) risk through the combined effects of several risk factors. Current risk estimation systems do not consider the effect of the metabolic syndrome. The aims of this study are firstly, to compare the ability of a high risk score using the European Joint Task Force Systematic Coronary Risk Evaluation (SCORE) system and NCEP ATPIII risk estimation systems, and secondly, using simple physical measurements to detect the metabolic syndrome in an asymptomatic healthy population.
Methods The metabolic syndrome was defined using NCEP guidelines. The European Joint Task Force definition of high risk is a 10-year fatal CVD risk of ≤ 5% now, or projected to age 60. In contrast, using NCEP guidelines, high risk is defined as a Framingham 10-year risk of hard coronary end-points of >20%. The diagnostic performance of the risk estimation systems and simple physical measurements in identifying the metabolic syndrome in subjects was assessed by calculating their sensitivities, specificities, positive predictive values (PPV), negative predictive values (NPV) and the area under the receiver operator characteristic (ROC) curves.
Results Of the 584 healthy volunteers (mean age 42, male 24%) studied, the prevalence of the metabolic syndrome was 11% (n = 64). Of these 64, SCORE identified 19 (30%) as high risk while identifying 62 (12%) of those without the metabolic syndrome as high risk. Using the Framingham function, six (9%) out of the 64 with metabolic syndrome were predicted as high risk, while 10 (2%) of those without the metabolic syndrome were considered high risk. Table 1 shows the comparison of the diagnostic abilities of the various physical measurements and risk estimation systems in terms of sensitivities, specificities, PPV, NPV and area under the ROC curves.
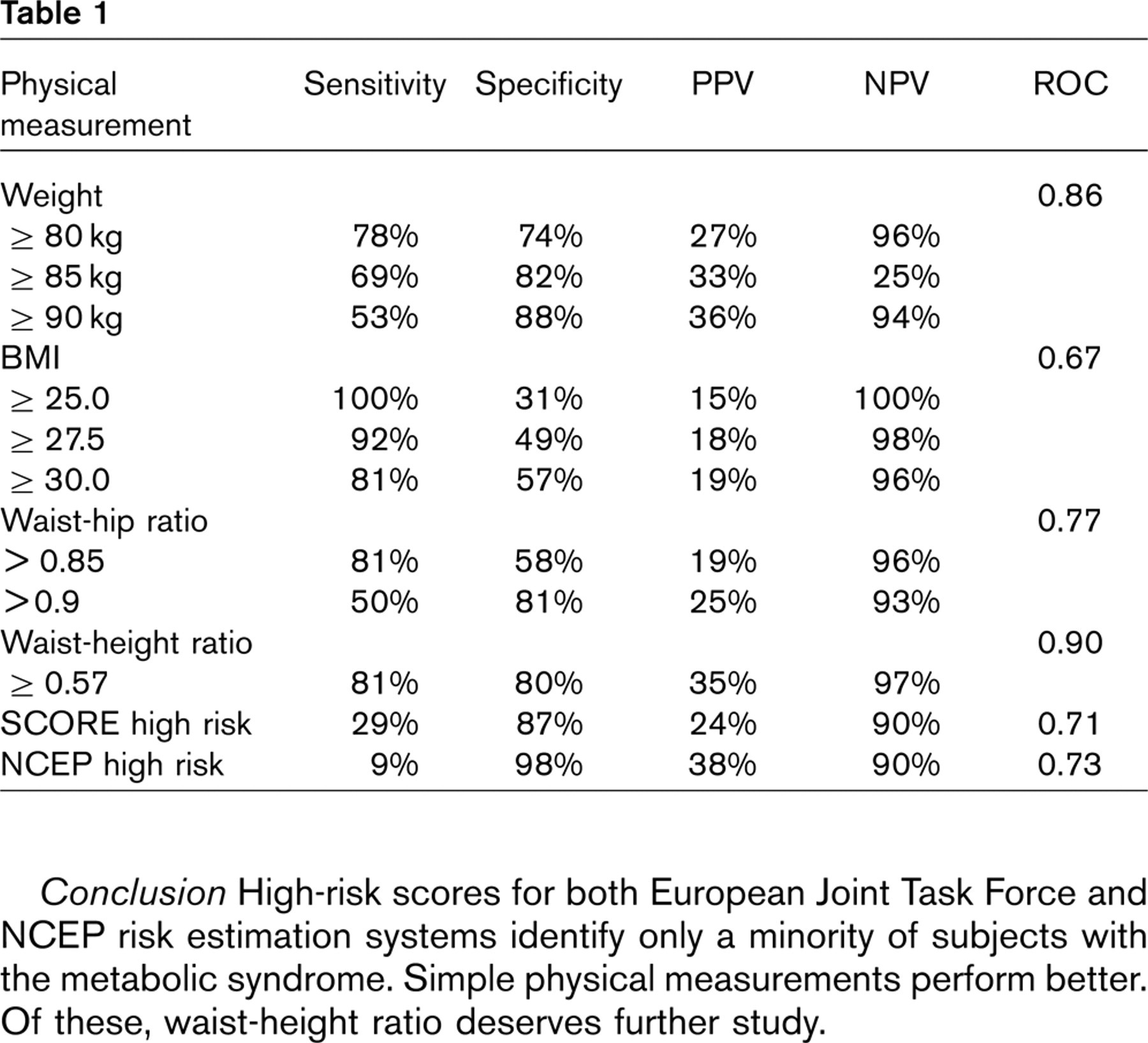
Conclusion High-risk scores for both European Joint Task Force and NCEP risk estimation systems identify only a minority of subjects with the metabolic syndrome. Simple physical measurements perform better. Of these, waist-height ratio deserves further study.
Diabetes: 14. The impact of diabetes and myocardial infarction at baseline and during follow-up on mortality from coronary heart disease
Gang Hua,b, Pekka Jousilahtia,b, Qing Qiaoa, Shuichi Katoha,c, Jaakko Tuomilehtoa,b
aDepartment of Epidemiology and Health Promotion, National Public Health Institute, Helsinki, bDepartment of Public Health, University of Helsinki, Helsinki, Finland, cDepartment of Internal Medicine, Jikei University School of Medicine, Tokyo, Japan.
Background Both myocardial infarction (MI) and diabetes are strong predictors of coronary heart disease (CHD) death. However, sex-specific data on the joint effect of diabetes and MI, and particularly on the effect of diabetes and MI during the follow-up, on CHD mortality are scarce.
Methods We prospectively followed 25,240 Finnish men and 26,546 women aged 25–74 years. Smoking status and the history of myocardial infarction, and type 2 diabetes were recorded, and height, weight, blood pressure and serum cholesterol level were measured at baseline. Additional data on the occurrence of diabetes and myocardial infarction were obtained from national hospital discharge and drug registers through computerized register linkage. Coronary heart disease mortality data were obtained from the national mortality register.
Results During a mean follow-up of 17.2 years, 3036 CHD deaths were recorded. The multivariate-adjusted hazard ratios (HRs) for CHD mortality were 1.90 (95% CI: 1.52–2.39) for men with baseline diabetes alone, 3.88 (95% CI: 3.42–4.40) for men with baseline MI alone, and 5.95 (95% CI: 4.31–8.23) for men with both baseline diabetes and MI compared with men without diabetes and MI. In women, the corresponding HRs were 4.78 (95% CI: 3.74–6.11), 2.59 (95% CI: 1.95–3.42), and 8.93 (95% CI: 5.43–14.7), respectively. When the diabetes and MI status during the follow-up was included in the analyses, the relative importance of diabetes markedly increased in women. When the analysis only included diabetes and MI at baseline, the multivariate-adjusted HRs for CHD mortality were low in men with diabetes alone (0.51, 95% CI: 0.40–0.66), but were high in women with diabetes alone (1.64, 95% CI: 1.12–2.39), in comparison with men and women with MI alone. This sex differential for CHD mortality was significant (χ2 = 28.01, 1df, P <0.001). When the analysis only included diabetes and MI during follow-up, the multivariate-adjusted HRs for CHD mortality were consistently low in men (0.46, 95% CI: 0.37–0.58) and in women (0.72, 95% CI: 0.56–0.93) with incident diabetes alone compared with men and women with incident MI alone (χ2= 5.87, 1df, P <0.025 between men and women).
Conclusion Diabetes and MI, both present at baseline and developing during the follow-up, increase the risk of CHD death markedly. The independent effect of diabetes, and the joint effect of diabetes and MI were larger in women than in men.
Diabetes: 15. Prediction of type 2 diabetes mellitus over 20 years among Danish women and men
Thomas Drivsholma, Michael Davidsenb, Hans Ibsenb, Hanne Hollnagelc, Knut Borch-Johnsend
aCopenhagen County Research Centre for Prevention and Health, University of Copenhagen, bMedical Department M of Medicine, Glostrup University Hospital, cResearch Unit and Department of General Practice, Copenhagen, University of Copenhagen, Copenhagen, dSteno Diabetes Centre, Gentofte, Denmark.
Background The development of type 2 diabetes mellitus (T2DM) is a life-long process. Most longitudinal studies of the development of T2DM have been carried out in populations with a high prevalence of T2DM, among men only, with a relative short follow-up time or with a limited number of risk factors under investigation.
Methods A population based age-specific birth cohort of Danish women and men were examined at age 40 (1976–1977) and re-examined at age 60 (1996–1997). A total of 662 (46.5% men) subjects free of T2DM and cardiovascular disease (CVD) at age 40 participated at the 20-year follow-up examination. At the baseline investigation T2DM was diagnosed by an individualised OGTT (1 g of glucose per kg body weight, max. 70 g), while a standardized 75g OGTT was used at age 60. Next to fasting plasma glucose (FPG) and 2h-OGTT-glucose the following risk factors for T2DM and CVD were recorded/measured by standardized methods at age 40: sex, fasting-insulin, BMI, cardio respiratory fitness (VO2-max estimated by a sub-maximal bicycle ergo meter test), diastolic and systolic blood pressure, triglyceride, high-density lipoprotein (HDL)-cholesterol and total cholesterol. In both investigations T2DM was defined as either known diabetes mellitus (DM) or T2DM according to WHO-criteria, for instance, a 2h-OGTT-glucose value 11.1 mmol/l and/or a fasting value ≤ 7.0 mmol/l.
Results A total of 54 individuals (57.4% men) had developed T2DM by age 60. All risk factors recorded/measured at age 40 predicted the development of T2DM in univariate, logistic regression analysis. In multivariate analysis using risk factors as independent variables, sex, 2h-OGTT-glucose, BMI and blood pressure (diastolic or systolic) predicted the development of DM. The final model is shown in the table below. Among individuals with combined 2h-OGTT-glucose, BMI and systolic blood pressure in the upper tertile of the study population at age 40, 56% (18/32) had developed T2DM by age 60. Among 45 individuals with combined 2h-OGTT-glucose, BMI and systolic blood pressure in the lower tertile of the study population at age 40, none had developed T2DM by age 60.
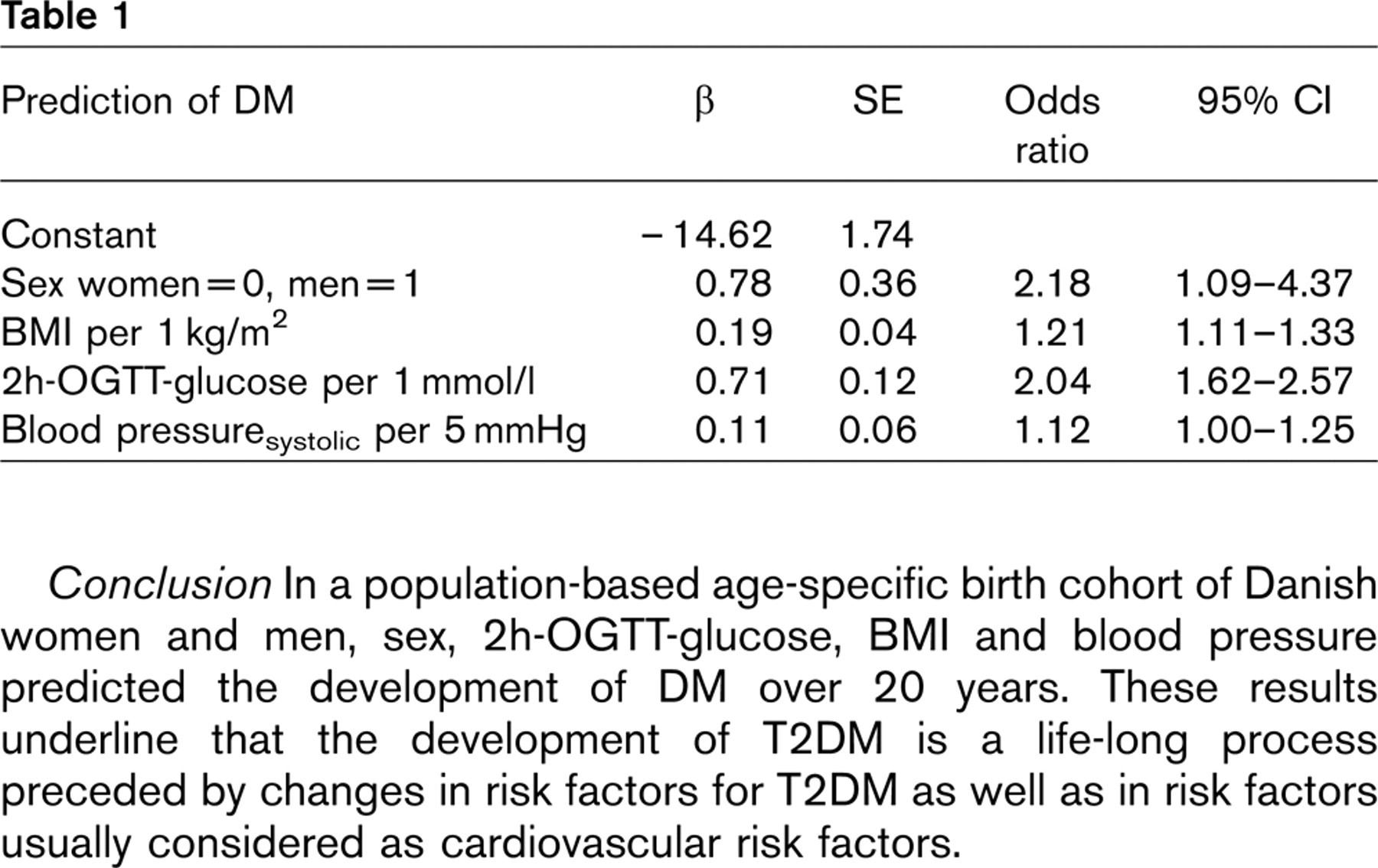
Conclusion In a population-based age-specific birth cohort of Danish women and men, sex, 2h-OGTT-glucose, BMI and blood pressure predicted the development of DM over 20 years. These results underline that the development of T2DM is a life-long process preceded by changes in risk factors for T2DM as well as in risk factors usually considered as cardiovascular risk factors.
Diabetes: 16. Metabolic syndrome, smoking and cardiovascular mortality
Hammar Niklasa,b, Johansson Sagab,c, Hu Gangd,e, Peltonen Markkud, Qiao Qingd,e, Tuomilehto Jaakkod,e, for the DECODE Study Group
aDepartment of Epidemiology, Institute of Environmental Medicine, Karolinska institutet, Stockholm, Sweden, bDepartment of Epidemiology, AstraZeneca Research & Development, Mölndal, Sweden, cCardiovascular Institute, Sahlgrenska University Hospital, Gothenburg, Sweden, dDepartment of Epidemiology and Health Promotion, National Public Health Institute, Helsinki, Finland, eDepartment of Public Health, University of Helsinki, Finland.
Background The metabolic syndrome (MetSyn) has been found to increase total and cardiovascular disease (CVD) mortality that are also associated with smoking. The aim of this study was to evaluate the impact of the joint exposure of MetSyn and smoking on total and CVD mortality.
Methods The study population consisted of six European cohorts in the DECODE study (n = 4452). The metabolic syndrome was defined primarily using a modified version of the WHO criteria but analyses were also performed for three other criteria (EGIR, NCEP, AACE). Mortality was followed for a median of 9 years. The relative risk of death for individual and joint exposure to MetSyn and smoking compared with absence of both exposures was estimated by proportional hazards regression adjusting for age, cohort and serum cholesterol. Synergy index was calculated to evaluate interaction. Additivity will give a synergy index equal to unity.
Results There were 701 deaths of which 244 from CVD. The MetSyn and smoking were both associated with increased CVD mortality independent of each other. Smokers with MetSyn had a relative risk of CVD mortality of 4.0 (95% CI: 2.5–6.3) in men and 6.6 (95% CI: 3.3–13.1) in women compared to non-smokers without MetSyn. This corresponded to a synergy index of 1.5 (95% CI: 0.8–3.5) and 1.8 (95% CI: 0.7–5.1) respectively. Somewhat lower estimates were recorded for all cause mortality. Other criteria for MetSyn gave rather similar findings.
Conclusion Smoking increases the risk of total and cardiovascular mortality associated with MetSyn by at least additivity.