
Abstract
Background
Patients with ischaemic heart disease have to perform exercise tests repeatedly. It is not clear if a small meal eaten before the test might influence it and if the meal's composition is important.
Design and method
We performed a double blind, randomised, crossover study on 20 volunteers with documented ischaemic heart disease known to have positive exercise tests. Each had three symptom limited exercise tests done one hour after a 200 ml meal, rich in either fat, carbohydrate or protein. Each postprandial test was compared to a fasting exercise test performed just before the meal.
Results
Postprandial blood pressure, time to angina and to peak exercise and double product at onset of ST-depression were not significantly altered by any of the meals. Heart rate was slightly increased only after the fat meal.
Conclusions
The nutritional composition of a small meal eaten an hour before an exercise test has no clinically important impact on the results of the test in patients with stable angina pectoris.
Introduction
It is customary to perform exercise tests (EXT) in the fasting state despite paucity of data regarding any severe adverse effect on the test of meals in general, and of specific macronutrients in particular. There have been a few reports on the impact of meal composition on EXT in patients with ischaemic heart disease (IHD) with regard to the ischaemic threshold and the extent of ischaemia [1–3, to haemodynamic alterations induced by meals of various compositions [4–7 and to the time interval between the meal and the EXT [8]. The effect of macronutrients composition of meals preceding exercise tests has been addressed in controls [9] and in endurance sports [10] and more recently the effects of fat and carbohydrate on EXT in IHD patients has been addressed [2, 8]. However, no double blind, randomised, crossover studies are available comparing the effects of all three macronutrients in patients with IHD. Furthermore, there have been no practical conclusions reached if EXT should be performed in the fasting state and, if meals are permitted, are there particular recommendations for the composition of pre-EXT meals.
We studied the effect of equivolumic meals containing predominantly fat, carbohydrate or protein on EXT and compared it to EXT in the fasting state in a double blind, randomised, crossover protocol in patients with ischaemic heart disease. The purpose of the study was to assess: (1) the effect of each meal type on the EXT; (2) to compare the effect of the meals to each other and (3) to reach practical recommendations with regard to the recommended composition of pre-EXT meals.
Materials and methods
Twenty men (age 61.9 ± 7.8, range 45–73) volunteered for the study, all had classical, stable, stress-induced angina (those with postprandial angina were not included) and angiographically documented significant coronary artery disease. They performed two exercise tests (EXT) on three separate days scheduled within about a week of each other. On each of the three days, a baseline EXT was performed after a 12 hour fast and was followed by a ‘test meal'. A second EXT was performed an hour after the meal. Anti-anginal medications, except for sublingual nitrates, were withdrawn 48 hours before the EXT.
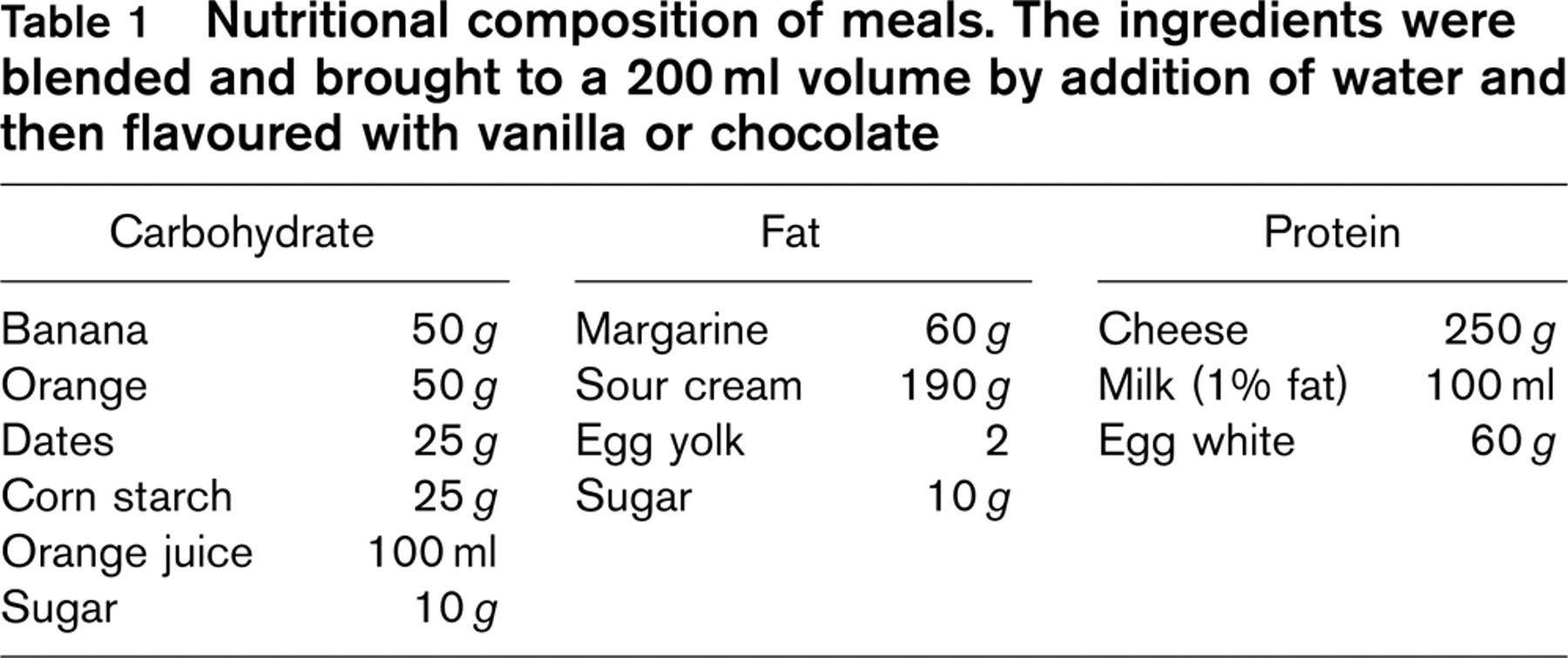
Three types of 200 ml ‘test meals’ were prepared consisting predominantly of fat (87% of 834 Kcal), of carbohydrate (91% of 331 Kcal) and of protein (81% of 258 Kcal). On each test day one of these meals was given in random order. The ingredients (Table 1) were blended and a technician added either vanilla or chocolate flavouring so that both the patient and physician were blinded to the composition of the meal.
Each symptom-limited treadmill exercise test was performed according to a standard Bruce protocol. Blood pressure (BP), heart rate (HR) and a 12-lead ECG were recorded at the start of the EXT and at 30-second intervals and also at onset of 1mm ST-depression, at onset of angina, at peak exercise, at resolution of angina and of ST-depression. The time to each of these events was recorded. Tests were terminated when predicted heart rate for age was reached, when angina became severe or when other standard indications for terminating the test were reached. During recovery, ECGs were recorded at 1-minute intervals until the ST segment returned to its pre-test configuration.
The ECGs from the six EXTs each volunteer had done were coded and interpreted by the same cardiologist, who was thus blinded to the relation between the ECGs and the meals. Blood samples were taken before the postprandial EXT and were analysed in the hospital biochemical laboratory by standard methods. Each patient signed an informed consent form approved by the Helsinki committee of this hospital.
Nutritional composition of meals. The ingredients were blended and brought to a 200ml volume by addition of water and then flavoured with vanilla or chocolate
Statistical analysis
Postprandial versus fasting heart rate (HR), systolic and diastolic blood pressure (SBP and DBP) at six events during the EXT (baseline, onset of ST-depression, onset of angina, peak exercise, resolution of angina and of ST-depression) were compared using repeated measures analysis of variance. The P values represent probability of falsely identifying interactions between meal (between subject) and time (within subject) effects. This analysis was also used to test for differences between the three meals in the magnitude of change in each parameter during the postprandial EXT compared to the corresponding fasting EXT values. In addition, the above analysis was repeated using the increase from resting (i.e., pre-test) values for each parameter. Comparison of time to occurrence of each of the six events (above) between each diet's postprandial EXT and its respective fasting EXT was done by the Wilcoxon rank-sum test (NPAR1-WAY procedure). The t-test for paired observations was also done to test the effect of the meals on the ischaemic threshold (i.e., the double product) at onset and resolution of angina and ST-depression. Thus the analysis tested: (1) the effect of each meal's postprandial EXT compared to its respective fasting EXT on the whole EXT (rather than comparing each of several points separately) and (2) the differences between the effects induced by the three meals.
Results
All patients completed the protocol and there were no adverse events during the study. The results are summarized with regard to the effect of each meal from two aspects: its effect on exercise parameters and on the ischaemic threshold (the double product which is directly related to myocardial O2 requirement) at onset of ischaemia as detected by angina and by ST-depression.
Changes induced by each meal-type compared to fasting EXT on heart rate (bpm), systolic and diastolic blood pressure (mmHg), double product (mmHg × bpm × 102) and EXT time (seconds)
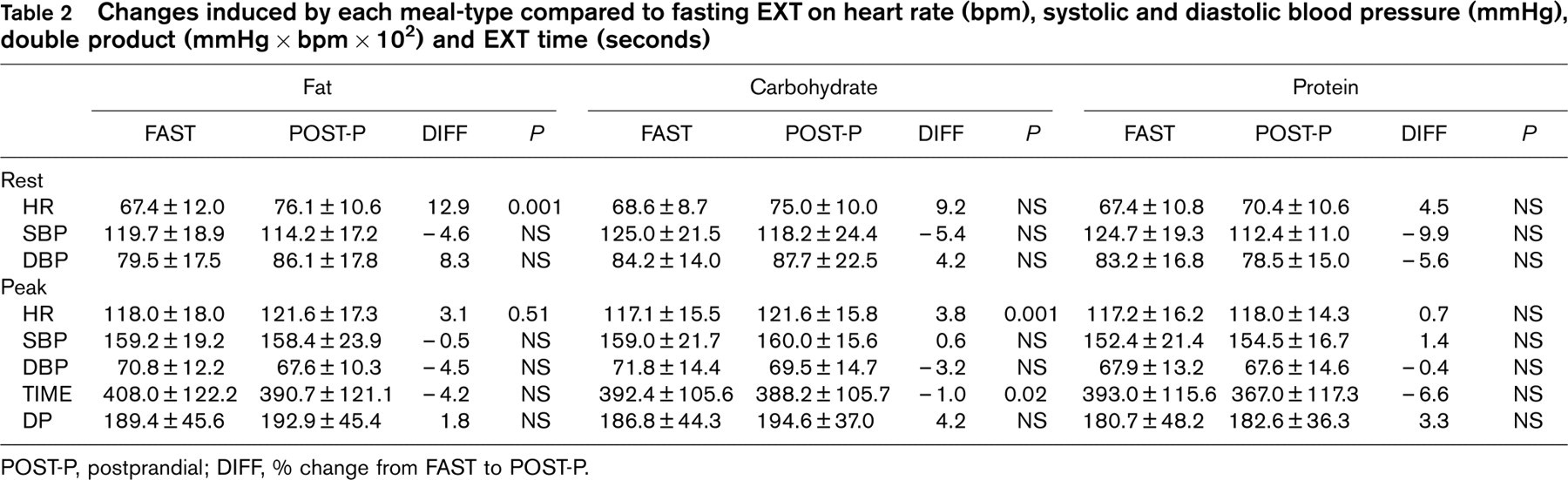
POST-P, postprandial; DIFF, % change from FAST to POST-P.
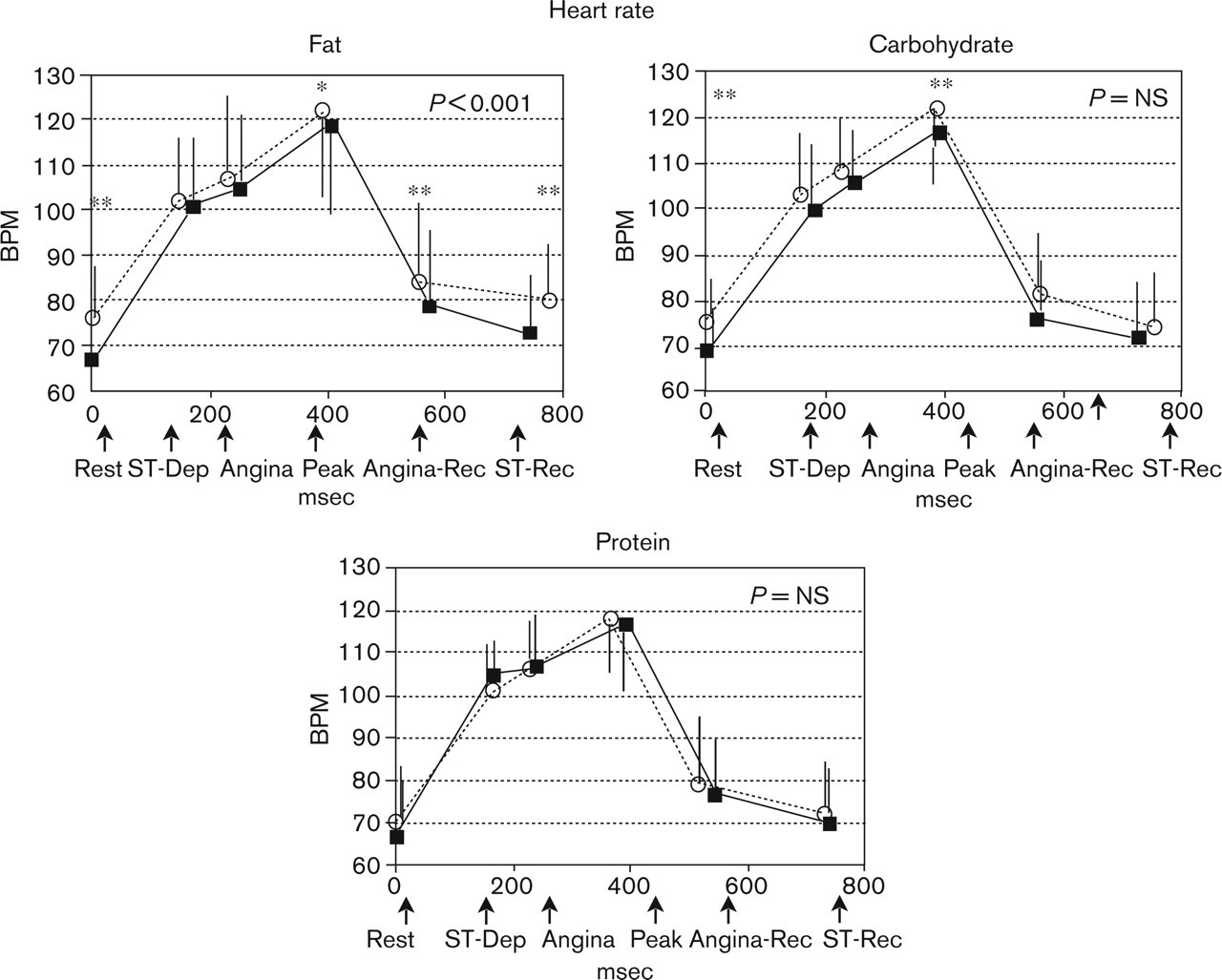
Effect of test meal versus fasting EXT on heart rate (bpm) and time (s) to appearance of main EXT events (baseline, onset of ST-depression, onset of angina, peak EXT, resolution of ST-depression, resolution of angina). Significant effects on HR during the whole EXT and differences at individual points during the EXT (by Student's paired t-test) are indicated. ANGINA, appearance of angina; ANGINA REC, recovery from angina; PEAK, peak exercise; REST, baseline; ST DEP, 1mm ST-depression; ST REC, return of ST segment to pre-test configuration. ∗P< 0.01, ∗∗P < 0.001 versus fasting EXT values by paired Student's t-test. ∗– – –∗ Fasting EXT, o—o postprandial EXT.
Effect on exercise (Table 2, Figs. 1 and 2)
In general
At rest, HR tended to increase and both SBP and DBP to decrease postprandially regardless of the meal composition. At peak exercise the magnitude of these differences was negligible.
Fat meal
Mean HR at baseline and throughout the EXT was an average of 3–9 bpm (range 3–13%) higher postprandially compared to the fasting EXT (P< 0.001). Both SBP and DBP tended to decrease by about 5% postprandially (P = NS). Patients’ maximal DP increased by 2% (353 ± 2973 mmHg × bpm, P = NS) whereas exercise time tended to decrease postprandially by 4% (17 ± 52 s, P = NS).
Carbohydrate meal
The HR tended to be higher throughout the test (4–9%) and both SBP and DBP to decrease (1–8%) postprandially. The maximal DP increased by 4% (784 ± 1784 mmHg × bpm, P = NS) and exercise time decreased marginally (by 4.2 ± 38 s, P = NS).
Protein meal
The meal did not induce significant changes in HR (1–4% increase). Although SBP and DBP were somewhat decreased at baseline postprandially (by 9–10%), it was not altered during the EXT. The maximal DP increased less than after the other meals (by 188 ± 2465 mmHg × bpm, P = NS) but time to peak exercise decreased the most and was almost half a minute shorter (26 ± 49s, 7%, P = NS) after this meal.
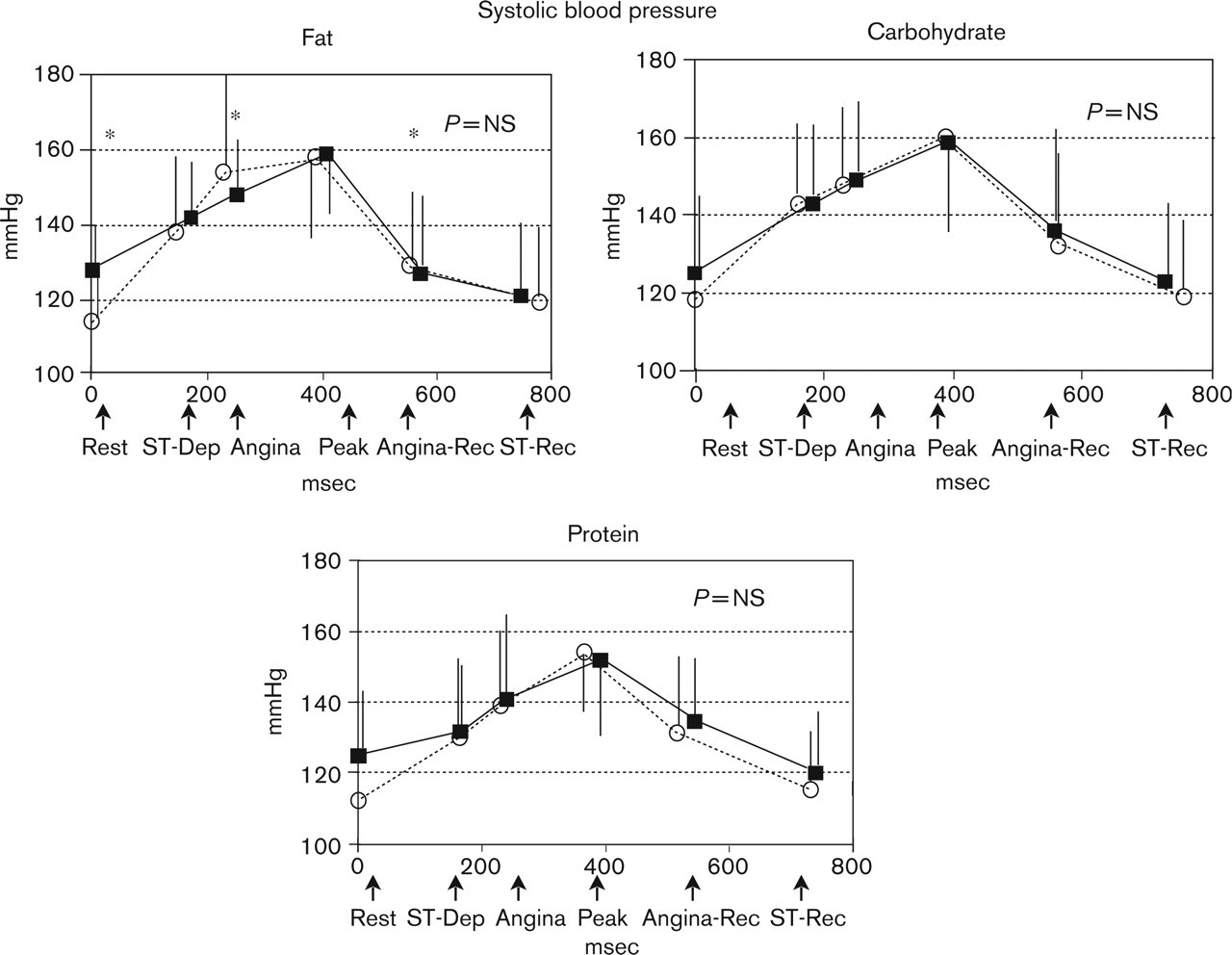
Effect of test meal versus fasting EXT on systolic blood pressure (mmHg) and time (s) to main events. ANGINA, appearance of angina; ANGINA REC, recovery from angina; PEAK, peak exercise; REST, baseline; ST DEP, 1mm ST-depression; ST REC, return of ST segment to pre-test configuration. ∗P< 0.01, ∗∗P< 0.001 versus fasting EXT values by paired Student's t-test. ∗– – –∗ Fasting EXT, o—o postprandial EXT.
Effect on ischaemia (Table 3, Fig. 3)
In general
There was a tendency for ischaemia (determined by ST-depression or angina) to appear sooner and resolve later postprandially. Thus, the ischaemic burden was slightly greater except after the protein meal, when it was marginally shorter. The double product at the appearance of ischaemia was not affected by the meals.
Fat meal
Ischaemia tended to appear earlier postprandially [ST depression by 26 ± 67s (15%) and angina by 20 ± 44s (8%) earlier], but to resolve later into recovery so that the duration of angina was 11 ± 96 s and of ST-depression 69 ± 146 s longer postprandially. The double product was insignificantly higher at onset and resolution of angina (7% and 10% respectively) and at return of ST to baseline (8%) than in the fasting EXT.
Carbohydrate meal
Postprandially ST-depression and angina occurred 23 ± 86s (12%) and 23 ± 71s (9%), respectively, sooner (P = NS) and tended to last longer into recovery (by 31 ± 87 s, and by 7 ± 50 s, respectively) than in the fasting state. However, the increased duration of angina (28 ± 88s) and ST-depression (51 ± 123s) were not statistically significant. At onset and resolution of ischaemia, the double product was similar to the corresponding fasting EXT.
Protein meal
Time to appearance of ischaemia was hardly affected by the meal (4% sooner to ST-depression, 1% to angina). Resolution of angina was unaffected and of ST-depression minimally prolonged (17 ± 92 s). Interestingly, this was the only meal after which the duration of both angina and ST-depression tended to be shorter (by 22 ± 86s and 9 ± 115 s, respectively). The double product was almost unaltered by the meal at onset and resolution of ischaemia.
Effect of each test-meal versus corresponding fasting state EXTs on appearance/resolution of ischaemia
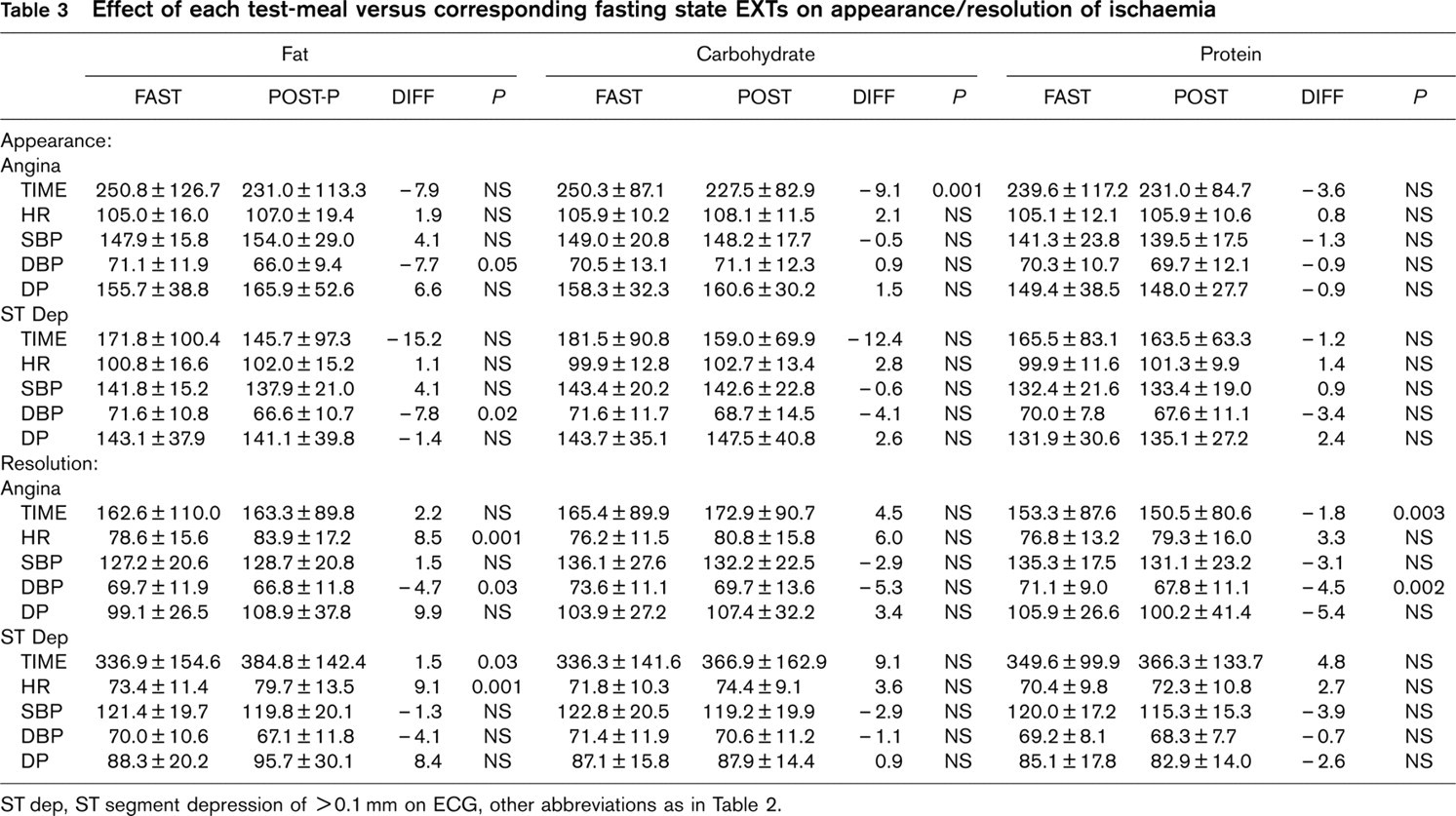
ST dep, ST segment depression of >0.1 mm on ECG, other abbreviations as in Table 2.
Between-meal differences
There were no clinically or statistically significant differences between changes induced by the three meals in either HR, SBP or DBP from their corresponding fasting EXT or from their rest (pre-test) values.
Effect of the meals on some biochemical parameters
After the carbohydrate meal plasma glucose was significantly higher than after the fat and protein meals (154.4 ± 83.1 mg/dl versus 102.8 ± 48.3 mg/dl and 110.3 ± 52.3 mg/dl, respectively, P < 0.001) and potassium was lower (4.1 ± 0.3 meq/l versus 4.3 ± 0.4 and 4.4 ± 0.3 meq/l respectively, P < 0.01). Postprandial blood levels of blood urea nitrogen, albumin and triglycerides were similar.
Discussion
It is customary to recommend that patients abstain from food at least 2–3 hours before an EXT. No references are given to support these recommendations. Also, there are no recommendations about the composition or size of the pre-test meal. Recent studies [1–3, 8] on postprandial EXT found that angina and ST-depression were induced sooner after a meal, especially after a carbohydrate-rich meal [3]. It was recommended that since some statistically significant postprandial alterations were found, meals should be avoided before EXT [1]. However, the main finding of the present study is that a small meal eaten an hour before a diagnostic EXT in patients with ischaemic heart disease, does not significantly alter exercise capacity, haemodynamic or ischaemic parameters, regardless of its main nutritional component: fat, carbohydrate or protein.
Many factors affect postprandial EXT and many parameters may be measured to quantify the magnitude of this effect. Among factors known to influence the EXT are meal size, composition, caloric value, time interval between meal and EXT and possibly psychological factors such as the smell and look of the meal. Thus, in order to reach practical recommendations, we used a double blind, randomised and crossover design to compare the effect that each of the three main nutrients had on EXT in volunteers with documented IHD (but not with spontaneous postprandial angina) who were challenged with equivolumic meals (200 ml), the size of a common breakfast/snack.
Not only must confounding factors be taken into account when comparing the results of various studies, but also the different study designs used. Thus, few previous studies were blinded, none were double blinded, some compared the effect of only one or two macro-nutrients on EXT to fasting EXTs or to placebo meals and different exercise protocols were used. In some studies two groups of patients were compared, rather than testing the same patients before and after a meal, some studies tested healthy volunteers, others studied patients with IHD, and in some the baseline fasting and the postprandial EXT were done on different days.
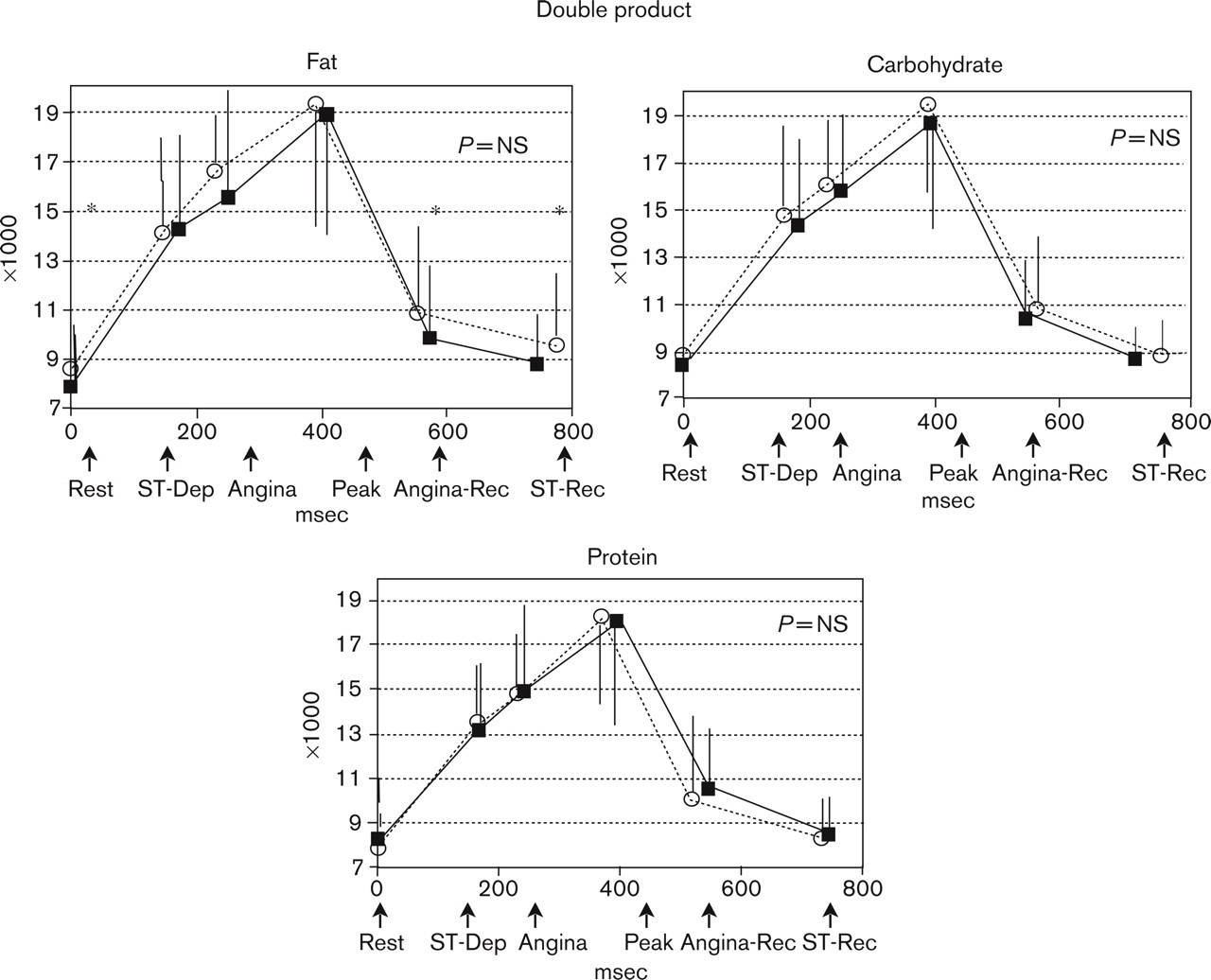
Effect of test meal versus fasting EXT on double product (mmHg × bpm × 103) and time (s) to main events. ANGINA, appearance of angina; ANGINA REC, recovery from angina; PEAK, peak exercise; REST, baseline; ST DEP, 1 mm ST-depression; ST REC, return of ST segment to pre-test configuration. ∗P<0.01, ∗∗P<0.001 versus fasting EXT values by paired Student's t-test. ∗– – –∗ Fasting EXT, o—o postprandial EXT.
With regard to healthy subjects at rest, following large meals there is a mild rise in HR with no substantial effect on SBP and a tendency toward a decrease in DBP [4, 5]. However, there are few studies in healthy people in which an attempt was made to differentiate between effects of individual nutrients. Dagenais [9] compared a 600 g meal rich in carbohydrate to a meal rich in protein. He studied 24 healthy subjects and the EXT was a limited 3.5 min bicycle test. Postprandially there were increases in HR and in SBP at rest and at peak exercise that were more pronounced after the protein meal. In general, his findings are similar to ours in patients with IHD, in which there was a trend toward a rise in HR, although we noted a trend toward a decrease in SBP and the changes we found were not accentuated after the protein meal. Recently the effect of meal-composition on endurance training was reported and it was concluded that meal composition had no clear effect on sprinting or 50 km cycling performance [10].
Results of studies on postprandial EXT that compared meals of varying compositions in patients with IHD vary in their findings. Lam [2] found no significant effect of either carbohydrate or fat meals on HR or BP. In contrast, other studies [3, 8] reported an increase in HR during a postprandial EXT that was more pronounced following a carbohydrate than a fat meal in patients with IHD. In our study the effect of both these meal types was of similar magnitude, with statistically significant changes in HR induced only by the fat meal. The delayed effect of fat on haemodynamics compared to carbohydrates may partly explain this difference because our EXT was done one hour after the meals, at a time the peak effect of carbohydrates may have already passed (although some effect still occurred as evidenced by the plasma glucose levels which were still elevated at the time of the postprandial EXT).
Induction of postprandial ischaemia in our study (both angina and ST-depression) tended to occur earlier after all the meals. This is in accord with other studies in patients with IHD [1–3, 7, 8] and has been related to the increased postprandial HR which results in the ischaemic threshold being reached sooner mostly after carbohydrate-rich meals, possibly as an expression of increased sympathetic nervous activity [3] and of increased mesenteric blood-flow and cardiac output [11], but not due to endothelial dysfunction [12]. Colles [1] showed that a mixed 1000 cal meal induced a rise in heart rate and an earlier appearance of angina and ST-depression but was not associated with more extensive ischaemia as determined by Thallium redistribution tests.
In addition to the earlier appearance of ischaemia, there was a trend towards a postprandial prolongation of the time from the beginning of recovery to complete resolution of both ST-depression and of angina, resulting in a trend toward a longer duration of ischaemia. It should be noted, however, that we measured the time to complete return of the ST segment to the pre-test pattern (not only to <1mm ST-depression) since we felt that it would be a more reliable (‘harder') endpoint for estimating time to complete resolution of electrocardiographic ischaemia. Also, we did not notice any difference in the magnitude of ST-depression or of subjective chest pain postprandially (these parameters were not quantified in our study), in accord with other studies, which demonstrated that such postprandial changes are negligible [13, 14] although others noted a greater ST-depression after a high-fat than a low-fat meal [12].
The clinically insignificant effect the small meals we studied had on diagnostic EXTs allows us to doubt the need for recommending that such tests should be done in the fasting state. Interestingly, the latest AHA scientific statement on this subject simply recommends that patients should not eat or smoke for three hours before the test (water may be taken as needed at any time) but no references are given [15]. Other guidelines recommend that patients be allowed to have a ‘light breakfast’ [16] or ‘a light meal’ [17] before the test and then to abstain from food at least 2–3 hours before an EXT and again, no references are given to support these recommendations and there are no recommendations at all regarding the composition or size of the pre-test meal. For clinical purposes, we found no reason to restrict patients from having a small meal an hour or more before an EXT, regardless of its nutritional composition. Besides, such a meal may offer the medical staff performing the EXT a possible bonus by marginally shortening the test. However, we agree with Colles’ conclusion [1] that when EXTs are done for research purposes, when even sub-clinical alterations in EXT parameters must be avoided, they should be done in the fasting state.
Limitations of the study
First, only male volunteers were studied but we see no theoretical reason for a different postprandial EXT response in females. Second, the meals were equivolumic but differed in their caloric content (see Table 1 for meal constituents). We felt that it would be more practical to reach recommendations regarding the composition and size of meals that are easier for patients to follow than regarding a given caloric value. Third, there are few studies on the effect of various meal volumes on diagnostic EXTs [18]. The relatively small meal volume we used (200 ml) may have contributed to the lack of significant effects on the EXT and thus our conclusions are limited to this meal size. Fourth, we did not study the effect of a mixed meal but since the three macronutrients had similar effects, mixing them would probably make the meal more palatable and would not alter our conclusions. Fifth, although each patient performed six EXTs, we tried to avoid the ‘learning effect’ by limiting the number of tests to two a day and spacing the test-days by at least a week. Finally, the statistical analysis was designed to determine the significance of changes induced by each of the test-meals throughout an EXT compared to a fasting EXT and then to compare these changes induced by the three types of test-meals to each other. Thus, although some statistically significant differences were found at individual points of the EXT (as noted in the figures but not used for drawing conclusions), the overall effect of each of the meals on the parameters studied was not significant except for an increase in HR induced by the fat meal.
We conclude that a 200ml meal an hour before a diagnostic EXT in patients with IHD does not have a clinically significant impact on the postprandial EXT regardless of its nutritional composition. It tends to hasten the onset on ischaemia (detected by both the appearance of angina and ST-depression) without affecting the ischaemic threshold, to marginally increase the ischaemic burden and to shorten the duration of the EXT. Thus, such meals may be recommended when EXT is performed for clinical purposes but should probably be avoided when performing EXT for research purposes.