
Abstract
Background
Controversy remains on the relationship between high-density lipoprotein cholesterol (HDL-C) and atherosclerotic cerebrovascular disease.
Methods
Over 5000 women living in the area of Naples, Southern Italy, were recruited for a prospective study on the etiology of cardiovascular disease in the female population (the ‘Progetto ATENA’ study). A sample of 310 participants underwent high-resolution B-mode ultrasound examination and the intima-media thickness and diameters of common carotid artery were measured. In addition to routine biochemical tests, these women also had oxidation markers determined.
Results
Women in the upper HDL-C quartile (HDL-C>1.89 mmol/L) had significantly lower body mass index and waist-to-hip ratio values, and triglycerides concentrations when compared with women in the first three quartiles. A linear negative association was found between HDL-C and carotid intima-media thickness (1.07 ± 0.16 mm for the IV quartile versus 1.10 ± 0.20 mm for the III quartile, 1.15 ± 0.26 mm for the II quartile and 1.19 ± 0.23 mm for the I quartile; P< 0.01 by ANOVA). No difference was found between groups with regard to carotid diameters and oxidation markers. After adjustment for other cardiovascular risk factors, women in the highest quartile of HDL-C had a decreased risk of carotid intima-media thickening (OR 0.42, 95%CI 0.23-0.94).
Conclusions
In asymptomatic middle-aged women, HDL-C levels were independently and negatively associated with preclinical atherosclerotic changes of the carotid artery wall.
Introduction
Epidemiological studies indicate that high-density lipoprotein cholesterol (HDL-C) protects against coronary heart disease [1,2]. Controversy however remains regarding the relationship between HDL-C levels and risk of atherosclerotic cerebrovascular disease. A few, but not all studies found a general trend towards a lower stroke risk with an increase in HDL-C in men, whereas in women participating in EUROSTROKE, elevated HDL-C levels were associated with a significant increased risk of cerebral infarction [3–6.
Over the last two decades, quantitative ultrasound determination of intima-media thickness (IMT) of the carotid wall has been performed to evaluate the presence of preclinical atherosclerosis in a large number of individuals with ‘traditional’ and ‘non traditional’ cardiovascular risk factors [7–10; has been shown to correlate with atherosclerotic lesions in other vascular territories [11,12], and has been used as outcome measures in clinical trials evaluating various treatment effects on the progression/regression of atherosclerosis [13–15. The aim of the present study was to evaluate the influence of a wide range of HDL-C levels on carotid artery wall geometry, characterized by both IMT and diameters, in a large sample of asymptomatic middle-aged women.
Methods
Study population
We studied a cohort of 310 middle-aged women living in the area of Naples (Southern Italy) and participating in the ‘Progetto ATENA’ study [16]. The general objective of this project is to investigate the causes of those chronic diseases that have a major impact on the female population. The total study cohort, enrolled within a 4-year period, consisted of 5062 women aged from 30–69 years. Less than 5% of the total cohort had ever used hormone replacement therapy. Potential participants with previous diagnosis of myocardial infarction, stroke and major cancers were excluded. Subjects with viral or bacterial acute diseases affecting the blood and urine biochemistry were asked to delay their participation. During a 6-month period, the older three of ten daily participants were invited to undergo an ultrasound examination of the carotid arteries, and additional biochemical tests. Of the 400 women invited, 310 (response rate 77%) accepted the additional investigations and constituted the present study sample. After age adjustment, there were no statistically significant differences between the sample of women who underwent carotid ultrasound evaluation and the remaining cohort of Progetto ATENA with regard to body mass index, systolic and diastolic blood pressure, the concentrations of cholesterol, triglycerides and the prevalence of current smokers. All women gave written informed consent and the ethical committees of the institutions involved approved the study.
Clinical and biochemical assessment
Anthropometric measurements were made with the subjects in indoor clothing, without shoes. Body mass index (BMI), used as a measure of general obesity, and was calculated as weight in Kg divided by height in m2. The waist-to-hip ratio was used as a measure of abdominal obesity. Blood pressure was measured twice in a sitting position after a resting period of at least 5 minutes using a random zero sphygmomanometer. Lifestyle questionnaires were based on the questionnaires used in major Italian population studies of cardiovascular disease.
Blood specimens were collected after a 12–14 hour fast, between 0800h and 0930h, to reduce the influence of circadian variation. Total cholesterol and triglyceride concentrations were measured using standard enzymatic methods [17,18]. High-density lipoprotein cholesterol was measured after precipitation of very low-density lipoprotein (VLDL) and low-density lipoprotein (LDL) cholesterol with phosphotungstic acid [19], and LDL cholesterol was calculated according to the Friedewald formula. Fasting glucose levels were enzymatically determined by the hexokinase method. Fasting insulin levels, used as a surrogate measure of insulin resistance [20], were determined by enzyme immunoassay (Boehringer Mannheim Immunodiagnostics on ES 300 instrument). Serum immunoglobulin G (IgG) antibody titre against oxidized-LDL was determined using an enzyme linked immunosorbent assay on micro-wells coated with copper oxidized-LDL (ELISA, Biomedica o-LAB, Biomedica Gruppe, Vienna, Austria). The error of the method was evaluated on both sera at low and high content of oxidized-LDL and was below 10%. The measurement of thiobarbituric acid reactive substances (TBARS) was used as a screening method for lipid peroxidation. A modified thiobarbituric acid (TBA) test was employed to minimize artefactual oxidative degradation of lipids during the assay. A description of the method has been published elsewhere [21]. The total radical-trapping activity potential of plasma (TRAP), which is indicative of plasma antioxidant potential, was measured using a spectrophotometric end-point method on a Cobas Fara centrifugal analyser (Roche, Switzerland). The error of the method was evaluated by analysing daily a plasma pool, and was lower than 5%. The method has been described elsewhere [21].
High-resolution carotid ultrasound
Carotid B-mode ultrasound examinations were performed by an expert sonographer, using a Biosound 2000 II SA equipped with an 8 MHz annular array mechanical transducer (Biosound Inc, Indianapolis, IN). This system provides high-resolution ultrasonic images with 0.3 mm axial resolutions.
The study protocol involved scanning the distal 1.0 cm of the near and far walls of the common carotid arteries. The crest at the origin of the bifurcation was used as an anatomical landmark to identify this segment. In each examination, the sonographer used different scanning angles (anterior, lateral and posterior) to identify the greatest IMT in each wall. Scans were recorded on super 1/2’ VHS videotape for offline analysis. At the Division of Vascular Ultrasound Research (Winston Salem, NC), certified ultrasound readers, blinded to the subjects’ clinical characteristics, reviewed the examinations and made quantitative IMT and diameter measurements, using a computerized system [22]. The thickest IMT (single max IMT) for the four carotid walls was used as the ultrasound end-point of the study. A single max IMT > 1.0mm was classified as increased IMT [23]. It was possible to obtain IMT measurements in all 310 subjects.
The common carotid internal diameter was measured as the distance between the trailing edge of the echo produced by the intima-lumen interface of the near wall and the leading edge of the echo produced by the lumen-intima interface of the far wall. The external diameter was defined as the distance between both media-adventitia interfaces.
Continuously monitored quality control data, derived from a large international multicenter trial being conducted during this time at the Division of Vascular Ultrasound Research show a coefficient of reliability for the common carotid IMT of 0.85. This figure includes instrument, subject, sonographer and reader variabilities [24]. For internal diameter, the coefficient of variation in replicate blind determination was 4.5% and 2.2% for the external diameter.
Statistical analyses
All statistical analyses were performed with SPSS for Windows, version 11.0. Continuous variables were described as mean and standard deviation, and categorical variables were reported as percentages. Variables that were not normally distributed, including triglycerides, fasting insulin and oxidation markers, were logarithmically transformed before analyses. Comparisons among subgroups of women classified on the basis of HDL values were performed using one-way ANOVA and Pearson χ2. Carotid IMT was treated as a continuous as well as categorical variable. Age-adjusted Pearson correlation coefficients were used to describe the association of carotid IMT with cardiovascular risk factors. Variables showing a significant relation (P < 0.05) to carotid IMT were included in multivariable analyses. Logistic regression was used to test the independent relation between HDL-C (independent variable) and increased IMT (dependent variable). Odds ratios and 95% confidence intervals were based on the comparison of quartile IV versus quartiles I–III.
Results
The clinical and biochemical characteristics of the study subjects are presented in Table 1. Women in the upper HDL-C quartile (HDL-C ≥ 1.89 mmol/L) had significantly lower BMI and waist-to-hip ratio (WHR) values, and triglycerides concentrations when compared with women in the first three quartiles.
A linear negative association was found between HDL-C and carotid IMT (1.07 ± 0.16mm for the IV quartile versus 1.10 ± 0.20mm for the III quartile, 1.15 ± 0.26mm for the II quartile and 1.19±0.23 mm for the I quartile; P < 0.01 by ANOVA) (Fig. 1). There was a trend toward lower diameters with increasing HDL-C concentrations, but ANOVA did not reach statistical significance (internal diameter: 5.77 ± 0.56 mm for the IV quartile versus 5.82 ± 0.63 mm for the III quartile, 5.78 ± 0.64mm for the II quartile and 5.83 ± 0.73 mm for the I quartile; external diameter: 7.29 ± 0.69 mm for the IV quartile versus 7.40 ± 0.79 mm for the III quartile, 7.34 ± 0.81mm for the II quartile and 7.44 ± 0.87mm for the I quartile).
Clinical and biochemical characteristics of the study sample stratified according to quartiles of HDL-C concentrations
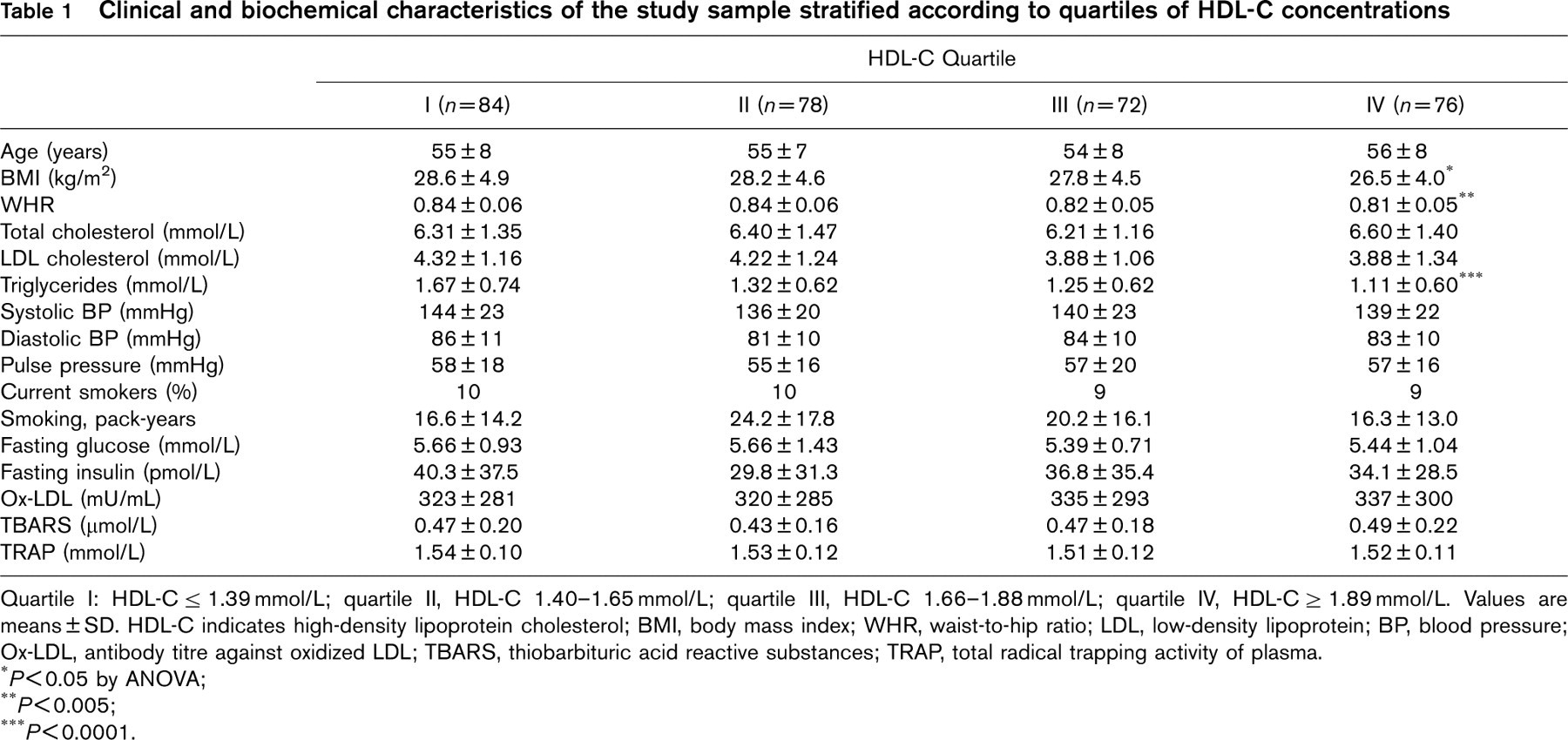
Quartile I: HDL-C ≥ 1.39 mmol/L; quartile II, HDL-C 1.40-1.65 mmol/L; quartile III, HDL-C 1.66-1.88 mmol/L; quartile IV, HDL-C ≥ 1.89 mmol/L. Values are means ± SD. HDL-C indicates high-density lipoprotein cholesterol; BMI, body mass index; WHR, waist-to-hip ratio; LDL, low-density lipoprotein; BP, blood pressure;
Ox-LDL, antibody titre against oxidized LDL; TBARS, thiobarbituric acid reactive substances; TRAP, total radical trapping activity of plasma.
∗ P<0.05 by ANOVA;
∗∗ P<0.005;
∗∗∗ P<0.0001.
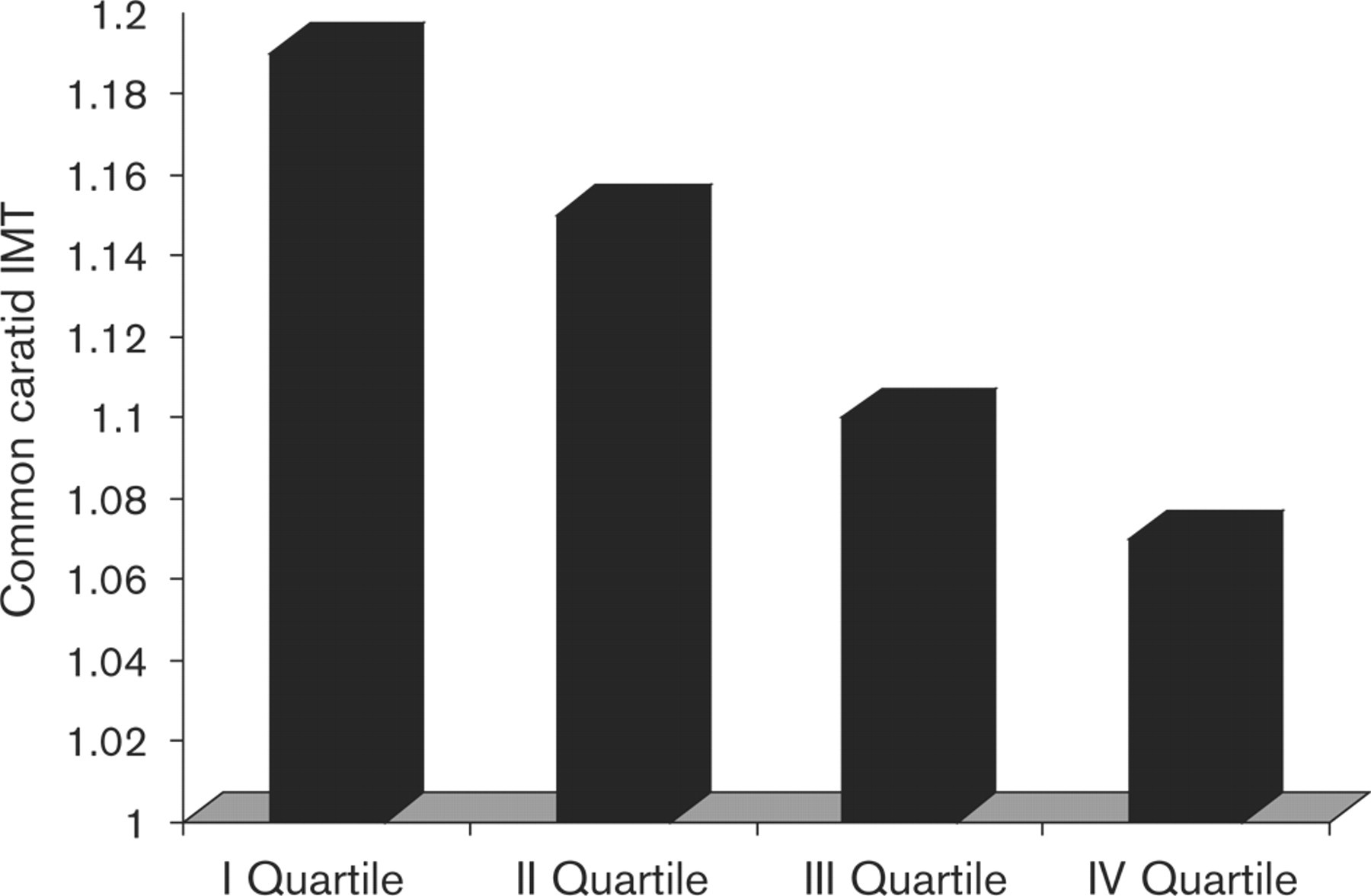
Common carotid single max IMT according to quartiles of HDL-C (P<0.01 by ANOVA).
Logistic regression analysis for increased carotid IMT (single max IMT≥1mm)
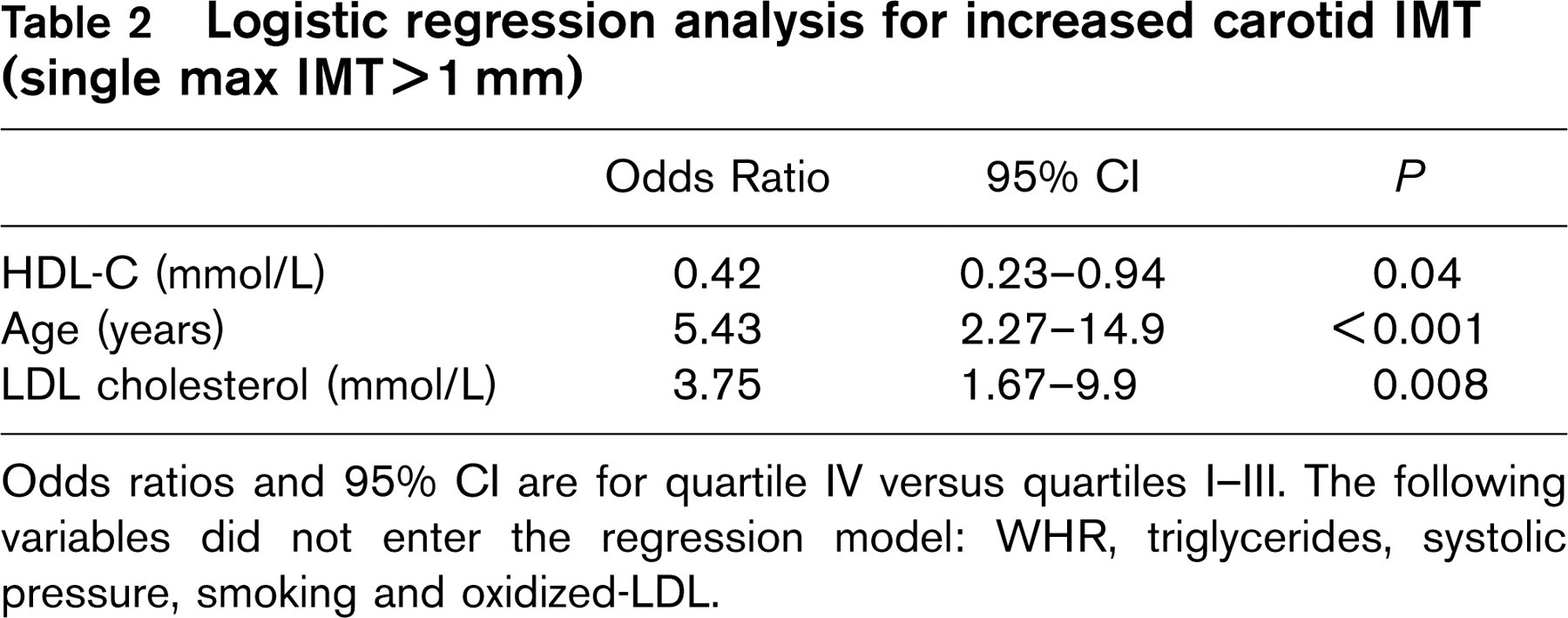
Odds ratios and 95% CI are for quartile IV versus quartiles I–III. The following variables did not enter the regression model: WHR, triglycerides, systolic pressure, smoking and oxidized-LDL.
In our study sample, 56 women had a HDL cholesterol value <1.3 mmol/L and fulfilled the Adult Treatment Panel III criteria for the metabolic syndrome. After controlling for relevant covariates (age and total cholesterol), such women had a greater common carotid IMT than women with normal metabolic status (1.20 ± 0.25mm versus 1.12 ± 0.21 mm, P = 0.01).
Carotid IMT was significantly correlated with body mass index (r = 0.15), WHR (r = 0.18), total and LDL-cholesterol (r = 0.12 and r = 0.17, respectively), triglycerides (r = 0.17), systolic and pulse pressure (r = 0.16 and r = 0.17, respectively), smoking (r = 0.15) and oxidized-LDL (r = 0.13).
In a multivariable logistic regression analysis, after adjustment for other cardiovascular risk factors, women in the highest quartile of HDL-C had a decreased risk of carotid intima-media thickening (OR 0.42, 95% CI 0.23–0.94) (Table 2).
Discussion
In the present study, we found a negative, independent association of HDL-C with carotid artery IMT–an indicator of preclinical atherosclerosis–in a Mediterranean female population. There have been few previous ultrasound investigations focused on women that evaluate the relationship between HDL-C and carotid atherosclerosis. Bonithon-Kopp et al., [25] reported in a sample of middle-aged French women, that HDL-C significantly decreased with the severity of carotid atherosclerosis. In a subgroup of 200 participants from the Healthy Women Study who had undergone high resolution B-mode ultrasound, HDL-C levels measured both before and after menopause were not independently associated with carotid IMT [26]. In a population of women with high atherosclerotic risk from Norway, increasing levels of HDL-C were associated with a decrease in mean IMT [27].
In our study, women in the lower HDL-C quartile had greater BMI and WHR values and triglyceride concentrations than women in the other quartiles. There is growing evidence that low HDL-C is one of the markers for insulin-resistance syndrome, a condition also characterized by abdominal obesity, hypertension, impaired glucose tolerance and the presence of an atherogenic lipoprotein phenotype–elevated trigyceride-rich lipoproteins and small, dense LDL particles [28]. However, when we performed the multivariable statistical analysis, HDL-C remained a negative predictor of carotid single max IMT, independent of LDL-cholesterol, triglycerides and other ‘traditional’ and ‘non-traditional’ risk factors.
High-density lipoprotein cholesterol > 1.55 mmol/L has been recognized as a ‘negative’ risk factor in the third report of the National Cholesterol Education Program (NCEP) expert panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults, i.e., its presence removes one risk factor from the total count [29]. The present data suggest that increasing HDL-C values are associated with a decreased risk of preclinical carotid atherosclerosis in middle-aged women, without a specific benefit cut-off level.
Although our knowledge of the complex processes involved in HDL-C metabolism has greatly improved over the last decade, the exact mechanism of the anti-atherogenic effect of HDL-C remains poorly understood. Experimental studies have shown that HDL-C may protect endothelial cells against the cytotoxic effects of LDL and may prevent oxidative modification of LDL particles [30–32. The present results show that elevated HDL-C levels were not associated with a decreased oxidative stress and indirectly support the theory that the protective effect of HDL-C is related to its role in reverse cholesterol transport, in which cholesterol that has been synthesized or deposited in peripheral tissue is returned to the liver.
In conclusion, our data suggest that elevated HDL-C levels are a protective factor against preclinical carotid atherosclerosis in a large sample of asymptomatic women.
Footnotes
Acknowledgements
The ‘Progetto ATENA’ was supported by funds from the Consiglio Nazionale delle Ricerche (Rome, Italy), ‘Progetto finalizzato Biotecnologie’ and ‘Progetto finalizzato FATMA'; the Ministero dell'Universitá e della Ricerca Scientifica e Tecnologica-MURST 1998, No. 9806174392-008 and the Fondazione Banco di Napoli.