
Abstract
Background
Benefits of cardiac rehabilitation with exercise therapy are well-established, although individual reactions are heterogeneous. The identification of determinants of training effects is useful from a prognostic point of view, but data regarding this are scarce. Furthermore, limited data exist on the determinants of complications during exercise in cardiac patients. This study aimed to investigate the determinants (1) of training effects in cardiac rehabilitation and (2) of complications requiring resuscitation during exercise activities at the hospital and during continued exercise at a sports club for cardiac patients.
Design
Clinical association study.
Methods
Determinants of changes in peak oxygen uptake (VO2) after 3 months of cardiac rehabilitation were determined by multiple regression analysis (n = 1909). Determinants of events requiring resuscitation (n = 21) were assessed by logistic regression analysis.
Results
Improvements in peak VO2 and exercise duration averaged 26%. Eighteen per cent of the variance in absolute improvements of peak VO2 was explained, with age and training characteristics as the strongest determinants. Twenty-one per cent of the variation in relative improvements was explained, with baseline exercise performance and training characteristics being the strongest determinants. The intake of anti-arrhythmics (odds ratio = 5.5; P<0.001) and the presence of ST-segment depression (> 1 mm) at baseline exercise testing (odds ratio = 1.6; P< 0.001) were predictive for serious complications. The occurrence of events requiring resuscitation was higher at the sports club (1/16 533 versus 1/29 214 patient-hours).
Conclusions
Age, baseline exercise performance and training characteristics were predictive for training effects in cardiac rehabilitation. Anti-arrhythmics and ST-segment depression at baseline exercise testing were predictive for complications.
Introduction
Cardiovascular diseases are currently a major health problem with a large burden of chronic disease, impairment and handicap. Although a decline in cardiovascular mortality has been observed over the last three decades in Western Europe, it remains extremely high in the eastern part [1]. In nearly all European countries, cardiovascular mortality represents around 40% of all-cause mortality before the age of 74 years [1]. Important advances in the treatment of acute coronary heart disease, such as coronary artery surgery, pharmacotherapy, thrombolytic treatment, heart transplantation and early percutaneous transluminal coronary angioplasty, have increased survival rates by about 50% [2]. This has led to an increased number of survivors and candidates for cardiac rehabilitation.
Beneficial effects of cardiac rehabilitation on secondary prevention and on physiological and psychosocial functioning are by now well-established [3, 4]. However, the individual variability in the response to a cardiac rehabilitation programme involving exercise therapy is high: according to the American College of Sports Medicine [5], the improvements in exercise performance after 3 months of training range from 10 to 60%. Because peak exercise capacity and training-induced changes in peak exercise capacity yield prognostic information [6–8], the identification of patients who are likely to benefit most from exercise therapy, would be of interest. A number of groups [9–15] addressed this question in sub-populations of cardiac patients, but it remains unclear which factors determine the changes in physical exercise performance. Up to now, the predictors for the responsiveness to cardiac rehabilitation have not yet been identified on a general cardiac rehabilitation population.
Limited data exist on complications requiring resuscitation during exercise activities in cardiac rehabilitation programmes and in coronary clubs. Three studies [16–18] described the incidence of cardiovascular complications during exercise in cardiac rehabilitation, and obtained divergent results. Also, the factors that can predict which cardiac patients are likely to suffer serious complications requiring resuscitation during exercise have not yet been investigated.
The first aim of this study was to identify determinants of the training effects in cardiac rehabilitation. The second aim was to investigate the determinants for complications requiring resuscitation in cardiac rehabilitation. Furthermore, the incidence of complications from exercise activities at the hospital and at a sports club for cardiac patients was compared.
Methods
Patients
Training effects
From the cardiac patients who were referred to the cardiac rehabilitation programme of the University Hospital of Leuven between 1979 and 2000, all patients who fulfilled the criteria mentioned below were selected for the present analysis. The inclusion criteria were (1) performance of a maximal exercise test before and after 3 months of physical training; (2) patients with a history of angina pectoris during exertion were accepted in the analysis when angina did not limit the exercise tests; (3) unchanged pharmacological treatment during the training period.
From a database of 2668 patients, 1909 patients met the inclusion criteria. Patients' characteristics, medical history and treatment are presented in Table 1. From the 789 patients that did not meet the inclusion criteria, 642 patients had dropped out of the rehabilitation programme. The baseline exercise test was not maximal in 65 patients, the second exercise test at 3 months was not maximal in 22 patients and 14 patients did not perform a maximal exercise test on both occasions.
Patient characteristics
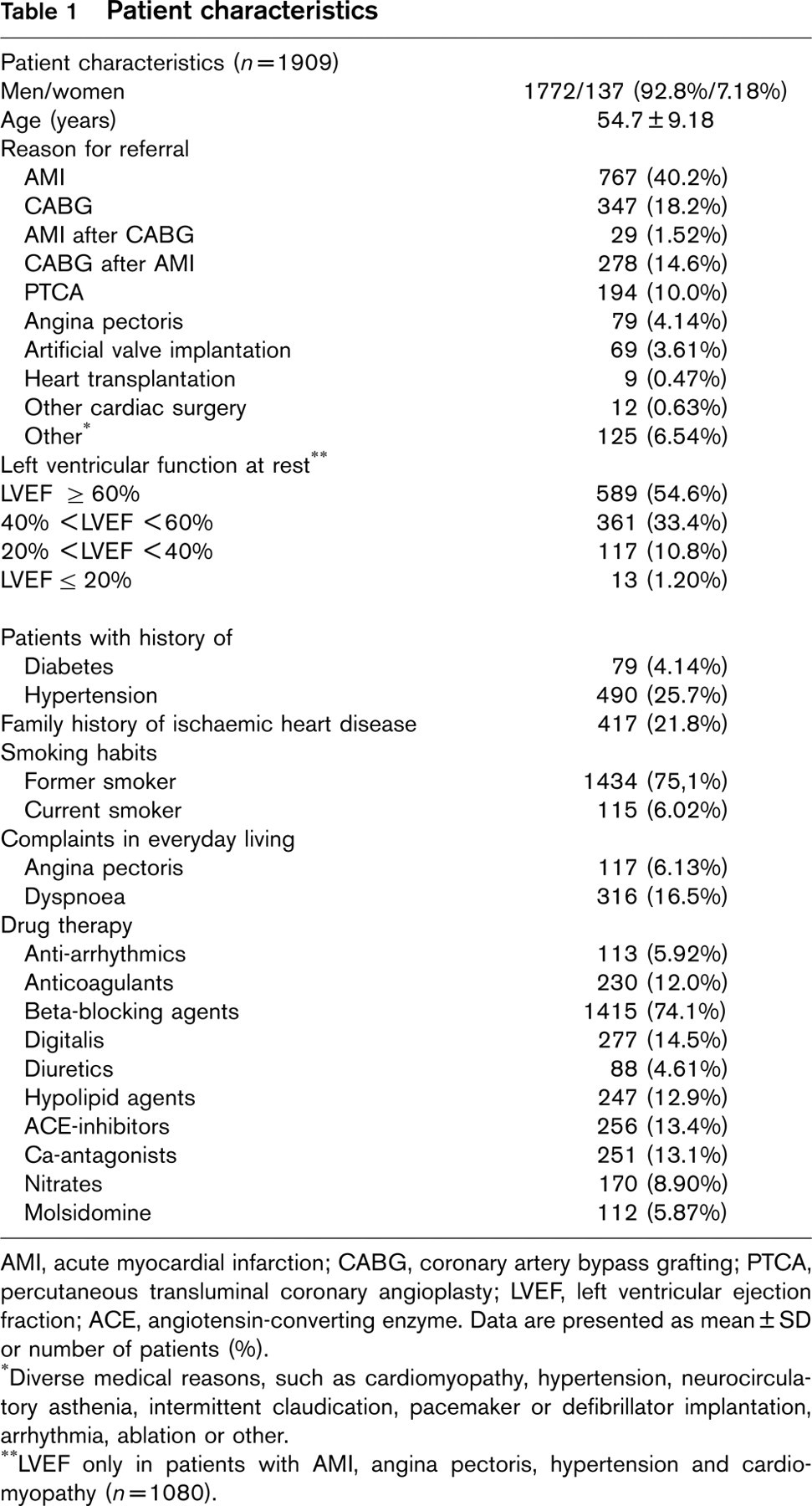
AMI, acute myocardial infarction; CABG, coronary artery bypass grafting; PTCA, percutaneous transluminal coronary angioplasty; LVEF, left ventricular ejection fraction; ACE, angiotensin-converting enzyme. Data are presented as mean ± SD or number of patients (%).
Diverse medical reasons, such as cardiomyopathy, hypertension, neurocirculatory asthenia, intermittent claudication, pacemaker or defibrillator implantation, arrhythmia, ablation or other.
LVEF only in patients with AMI, angina pectoris, hypertension and cardiomyopathy (n = 1080).
Complications
All patients who experienced an event requiring resuscitation during exercise at the rehabilitation programme at the hospital or in the local sports club for cardiac patients, also in the period 1979–2000, were selected for the present analysis.
Methods
Exercise testing
Maximal exercise tests on the bicycle ergometer (Siemens-Elema 380B; Ergometrics 800S, Ergometrics, Bitz, Germany) were performed in the laboratory where room temperature was stabilized at 18 to 22°C. The initial workload of 20W was increased by 30W every 3 min until exhaustion. Systolic and diastolic blood pressures were measured every 3 min by auscultation using a mercury sphygmomanometer or an STBP-780 device (Colin, Komaki, Japan). A 12-lead electrocardiogram (Max Personal Exercise Testing, Marquette, Wisconsin, USA) and respiratory data through breath-by-breath analysis (standard temperature pressure dry conditions of the gas; Sensormedics 920, Bilthoven, The Netherlands and Oxygen Alpha, Jaeger, Mijnhardt, Bunnik, The Netherlands) were registered continuously. Heart rate was calculated from the electrocardiogram. The gas analysers and the flowmeter were calibrated before each test according to the manufacturer's instructions. Oxygen uptake (VO2) and carbon dioxide output (VCO2) were determined from the continuous measurement of oxygen and carbon dioxide concentration in the inspired and expired air. The respiratory gas exchange ratio (carbon dioxide output/oxygen uptake; RER), ventilatory equivalent for oxygen (pulmonary ventilation/oxygen uptake; EqO2), and oxygen pulse (oxygen uptake/heart rate) were calculated. The ventilatory threshold was determined according to the method of Wasserman [19].
Patients participated in an ambulatory, supervised exercise programme for a period of 3 to 6 months (phase II cardiac rehabilitation). Three exercise sessions per week were offered, with duration of approximately 90 min per session. Each training session consisted of cycling, running, arm ergometry, rowing, callisthenics and relaxation. The initial exercise intensity was individually determined for each patient by calculating an interval for training heart rate, using the formula of Karvonen: resting heart rate + 60 (peak heart rate - resting heart rate), and was further progressively increased up to 90% of heart rate reserve.
After finishing phase II rehabilitation, patients could go to a sports club for cardiac patients (Phase III rehabilitation) where they could participate in weekly sessions of swimming (1 h/week), volleyball (1 h/week), walking (3 h/2 weeks) and in- and outdoor training, involving running, callisthenics, floor exercises, basketball or football (two sessions of 1 h/week). There is no limitation in time period for phase III rehabilitation.
Complication rates
The incidence of complications requiring resuscitation during exercise from the period 1979–2000 were assessed in the ambulatory rehabilitation programme at the hospital as well as in the local sports club for cardiac patients (SC) and are expressed per patient-hours of exercise (attendance rates multiplied by training hours). The training programme at the hospital exceeds the 3 months that are mentioned previously, and is normally finished at 6 months. However, it is possible that patients remain active in the programme (one training/week), especially when they are considered to have a high-risk profile for complications.
Statistical methods
Data were analysed using SAS statistical software version 8.0 for Windows (SAS Institute Inc, Cary, North Carolina, USA). Data were reported as means ± standard deviations or as number of patients and frequency rates for dichotomous variables. Dichotomous variables were encoded as 1 in presence of the characteristic and otherwise as 0; men were encoded as 0, women as 1. Comparisons of two means were made by means of a two-tailed paired Student's t-test; analysis of variance was used for multiple comparisons of means. The Tukey test was used for post-hoc comparisons.
Stepwise regression analyses were performed on the total database regarding changes in peak VO2. Variables included in the stepwise analyses were gender; age; body mass index; pharmacological treatment; underlying pathology; a history of angina and/or dyspnoea in daily life at the start of the rehabilitation programme; diabetes; intermittent claudication; chronic atrial fibrillation; past and present smoking; sitting blood pressure; presence of rhythm disturbances, significant ST-changes during the baseline exercise test (ST depression ≤ 1 mm); exercise duration at the baseline exercise test. In a second analysis, also peak heart rate and ventilatory threshold from the baseline test were included. Left ventricular ejection fraction (LVEF) was only included in separate regression analyses on patients in whom it was available. A stepwise regression analysis was also performed regarding baseline peak VO2 on the group of patients in whom LVEF was available.
Stepwise logistic regression analysis was performed to identify risk factors for complications requiring resuscitation.
The level of statistical significance was set at P < 0.05.
Training effects
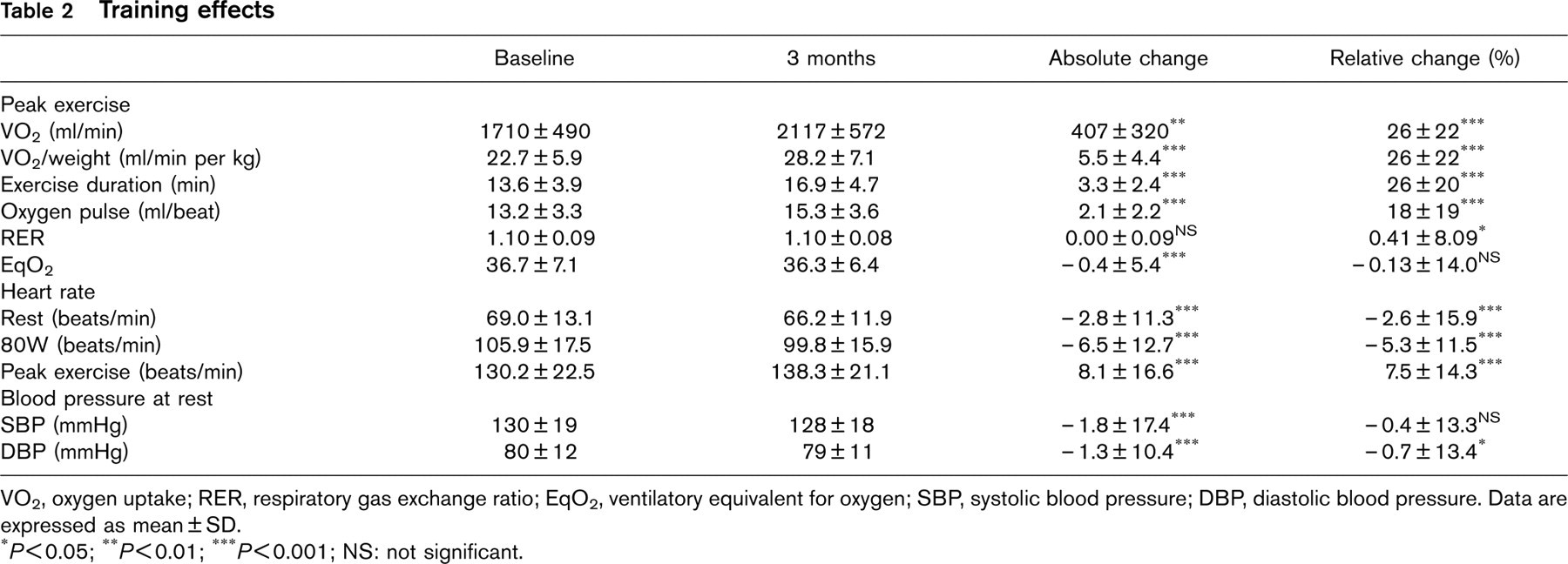
VO2, oxygen uptake; RER, respiratory gas exchange ratio; EqO2, ventilatory equivalent for oxygen; SBP, systolic blood pressure; DBP, diastolic blood pressure. Data are expressed as mean ± SD.
P < 0.05; ∗∗ P < 0.01; ∗∗∗ P < 0.001; NS: not significant.
Results
Training effects
The duration of the training period averaged 13.5 ± 4.4 weeks and mean attendance rate was 2.3 ± 0.5 times per week. Mean training intensity, determined as the ratio of mean exercise heart rate during the last three training sessions and peak heart rate during the post-training exercise test, was 81.4 ± 11.4%.
Training effects are illustrated in Table 2. Exercise performance was significantly increased after training as evidenced by the 26% average improvement in peak oxygen uptake (VO2) and exercise duration. Figure 1a and 1b indicate approximately normal Gaussian distribution curves for absolute and relative changes in peak VO2, but with a large spread of the data (−50% to + 181%). Peak oxygen pulse increased with 18% (P < 0.001). The respiratory data at the end of exercise (RER and EqO2) indicate a similar maximal effort as well before as after the training period. Other results of training were the reduction of resting and submaximal heart rate and the small, though significant, decrease in blood pressure.
For comparison of relative training effects between patients with different pathologies, eight groups of patients were defined: patients with myocardial infarction (AMI), coronary artery bypass grafting (CABG), AMI combined with CABG, angina pectoris, artificial valve implantation, heart transplantation, percutaneous transluminal coronary angioplasty (PTCA) and others. Training effects regarding peak VO2 according to these groups are illustrated in Table 3. Analysis of variance revealed significant differences in absolute as well as relative changes in peak VO2 and exercise duration among the groups (P < 0.001). Results of post-hoc comparisons for relative changes in peak VO2 are illustrated in Figure 2. The group of patients who underwent PTCA had significantly smaller training effects for peak VO2 compared with the groups of patients with AMI, AMI + CABG and CABG. Comparison of baseline capacity showed that the initial level of peak VO2 was higher in patients with PTCA compared with all other groups (P < 0.05), except for patients with AP. The group of patients defined as ‘other' made less improvement in peak VO2 compared with the groups AMI + CABG and CABG. Analysis with exercise duration yielded similar results.
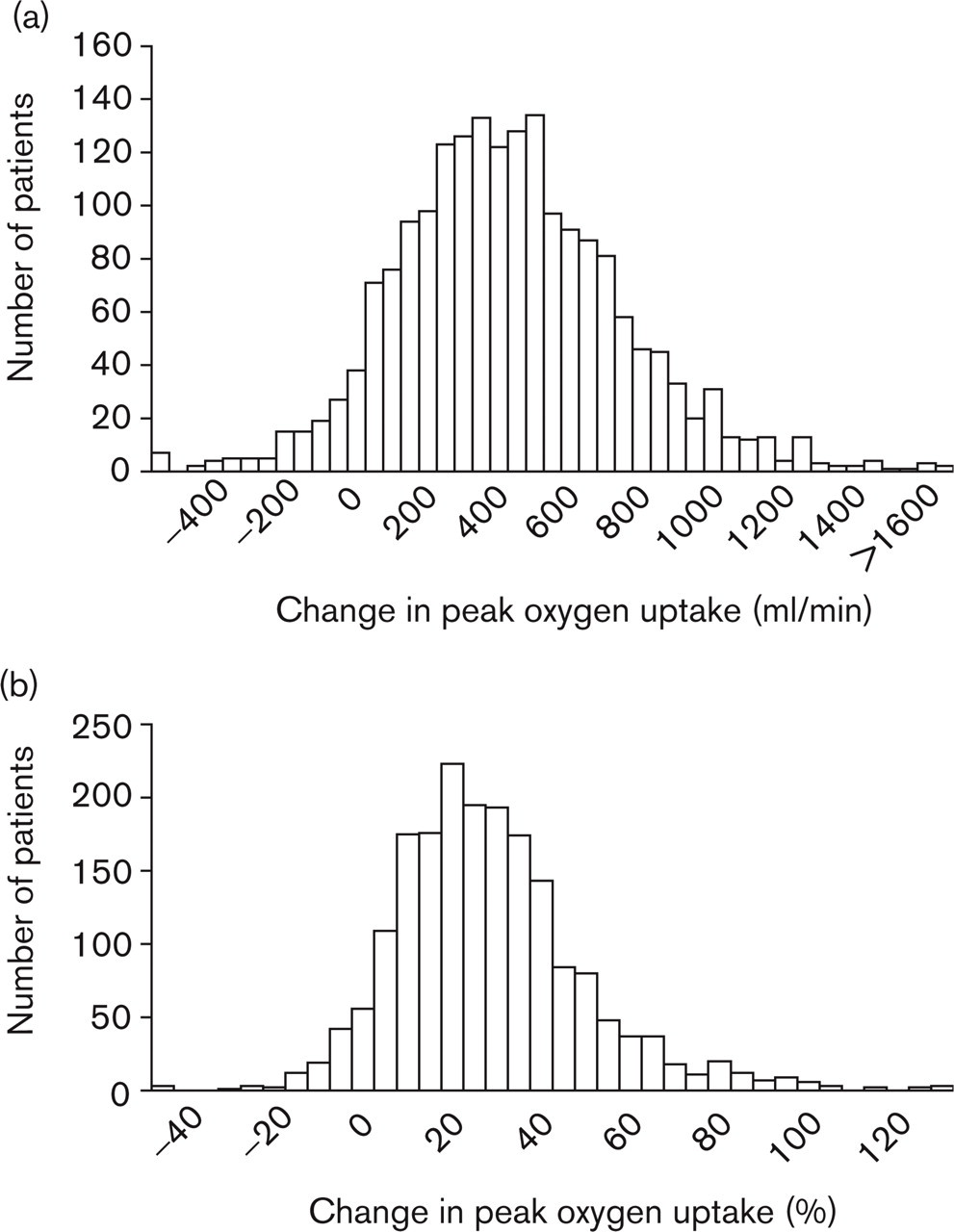
(a) Histogram regarding the distribution of absolute change in peak VO2; (b) Histogram regarding the distribution of relative change in peak VO2.
Training effects regarding peak VO2 in different groups of patients
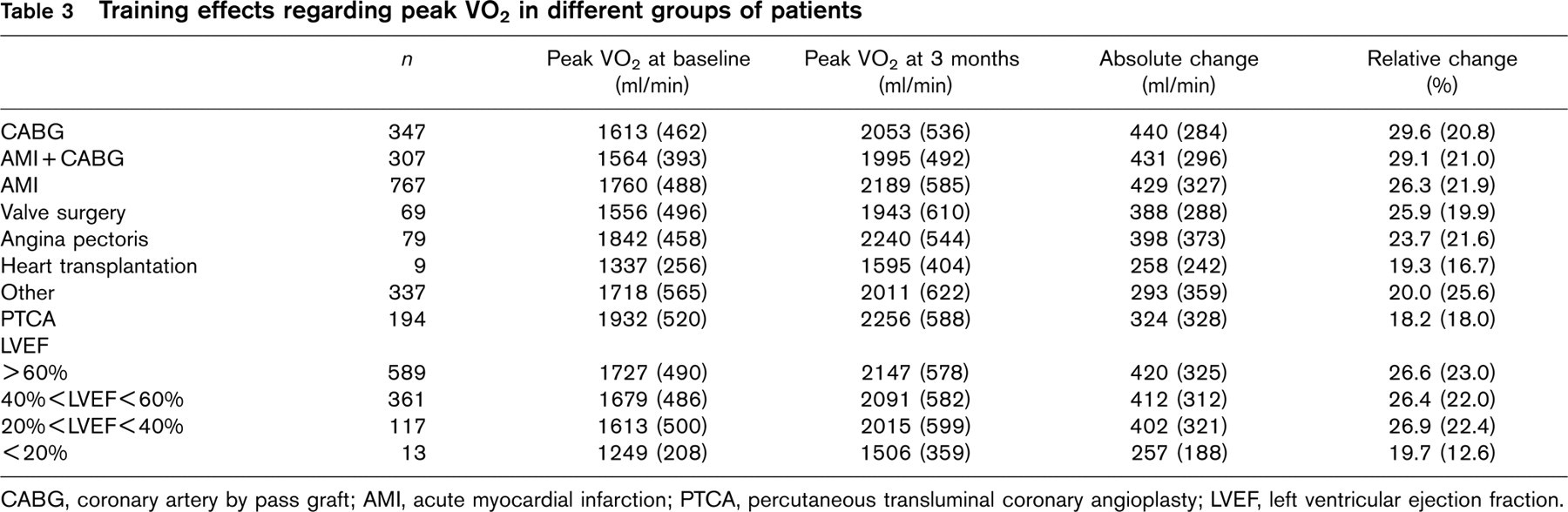
CABG, coronary artery by pass graft; AMI, acute myocardial infarction; PTCA, percutaneous transluminal coronary angioplasty; LVEF, left ventricular ejection fraction.
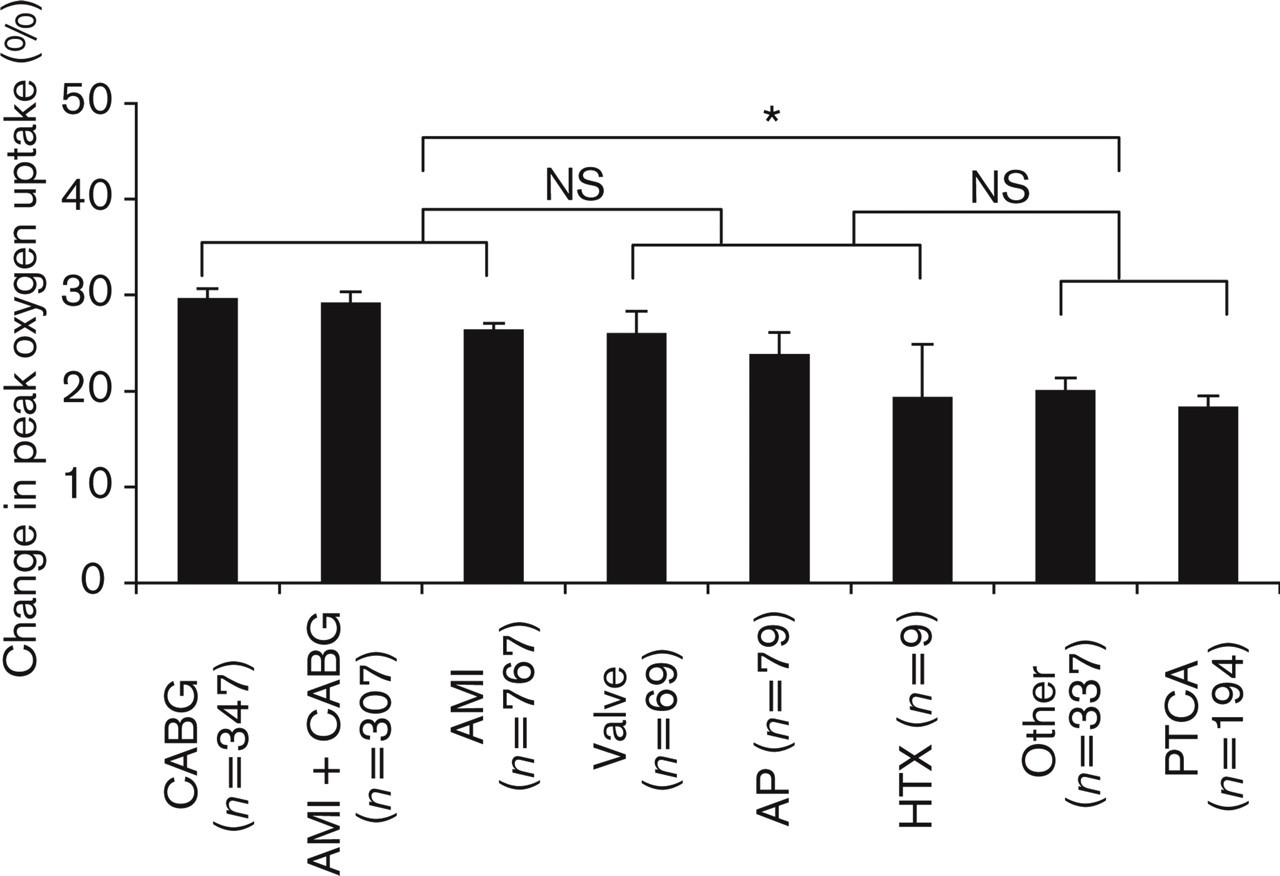
Comparison of training effects for peak VO2 (F = 7.76; P<0.001) in patients with various cardiac pathologies, expressed as relative change. The Tukey test was used for post-hoc comparisons, P < 0.05. Data are presented as mean ± SEM. CABG, coronary artery bypass grafting; AMI, myocardial infarction; Valve, artificial valve implantation; AP, angina pectoris; HTX, heart transplantation; PTCA, percutaneous transluminal coronary angioplasty. ∗Significantly different; NS, not significantly different.
Patients were divided into four groups with regard to left ventricular ejection fraction (LVEF ≤ 20%; 20% <LVEF ≤ 40%; 40% <LVEF ≤ 60%; LVEF>60%). Training effects regarding peak VO2 according to these groups are illustrated in Table 3. The multiple regression analysis on this group of patients (n = 1080) regarding baseline VO2 did not reveal LVEF as a variable in the prediction of baseline peak VO2. Also the relative changes in peak VO2 by training were not significantly related to LVEF (Fig. 3), although for the absolute changes LVEF was a significant independent determinant (R = 0.07; P = 0.02).
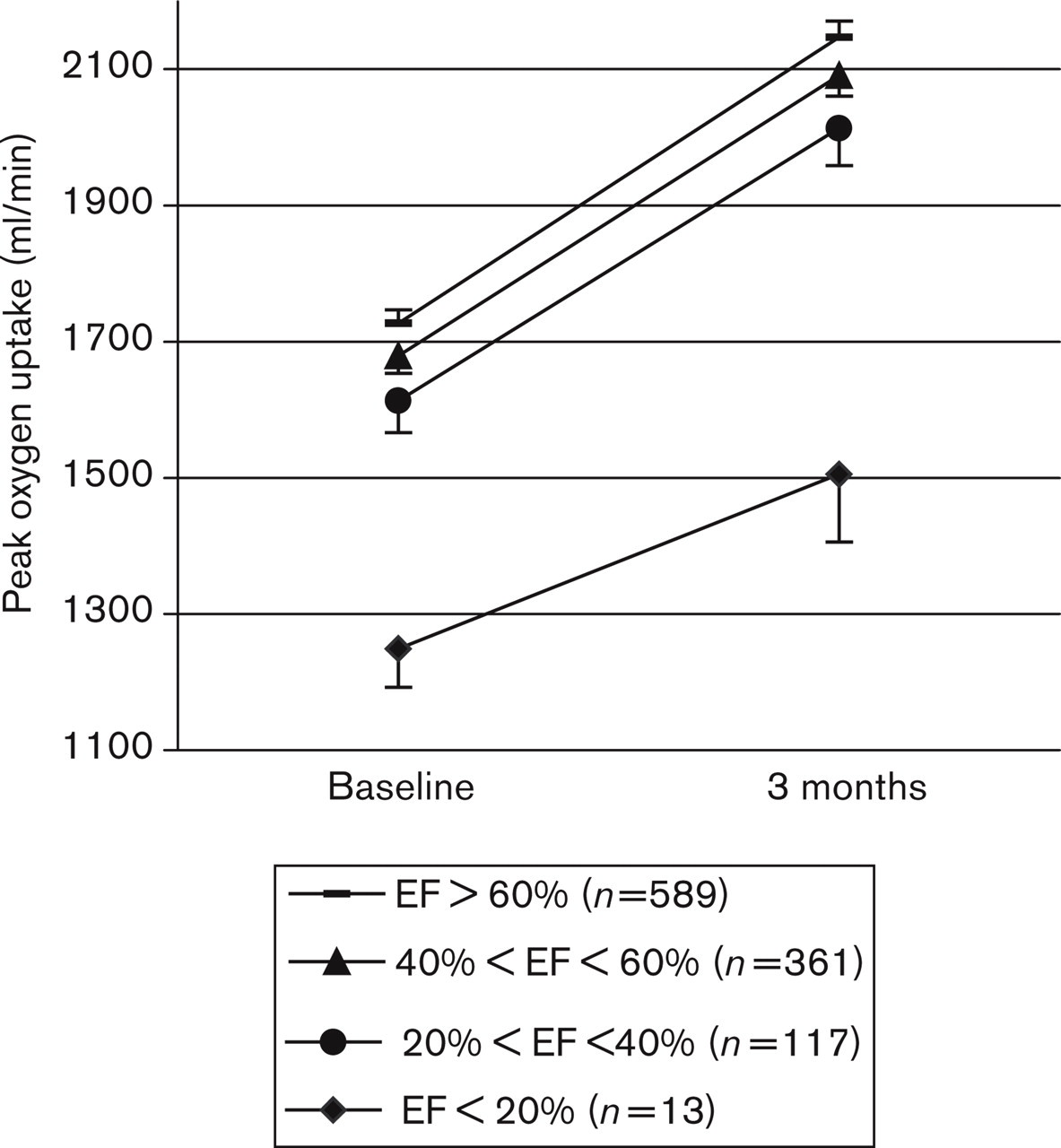
Comparison of training effects for peak VO2 according to left ventricular function. The difference in relative improvements between groups was not statistically significant (F = 0.42; P < 0.74). Data are presented as mean ± SEM. EF, left ventricular ejection fraction.
Table 4 shows the results from multiple regression analysis for investigation of the determinants regarding the absolute and relative change in peak VO2 after training. The multiple correlation coefficient for absolute changes was R = 0.42 (P < 0.001), with 11 variables to explain 18% of the changes in peak VO2. Twelve variables explained 21% of the relative changes in peak VO2 (R = 0.46; P < 0.001). Age and baseline exercise performance, given as exercise duration, had the strongest partial correlation coefficients for absolute and relative changes in peak VO2, respectively. Training characteristics (frequency and intensity) appeared in the second and third place in both models. When peak heart rate and ventilatory threshold from the baseline exercise test were included in the analysis for absolute changes in peak VO2, the variance explained increased to 37%.
Significant partial correlation coefficients and parameter estimates of absolute and relative changes in peak oxygen uptake: data from multiple regression analysis
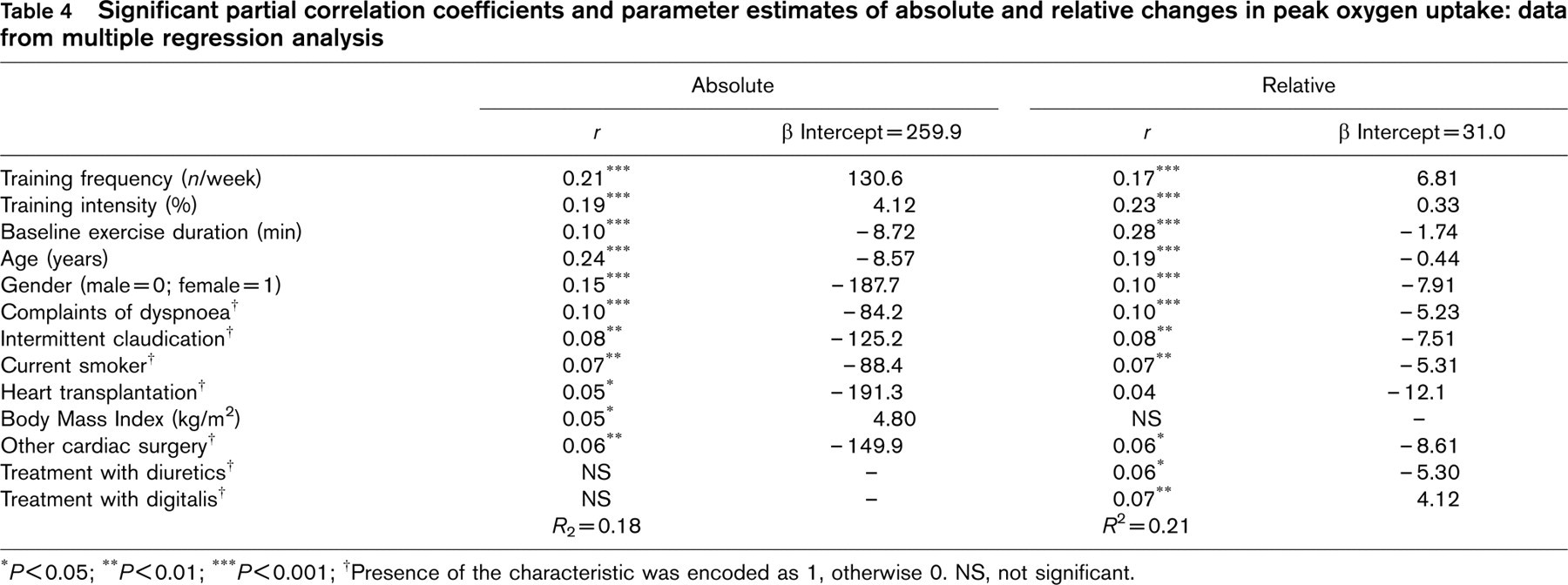
P < 0.05; ∗∗ P < 0.01; ∗∗∗ P < 0.001; †Presence of the characteristic was encoded as 1, otherwise 0. NS, not significant.
Complications
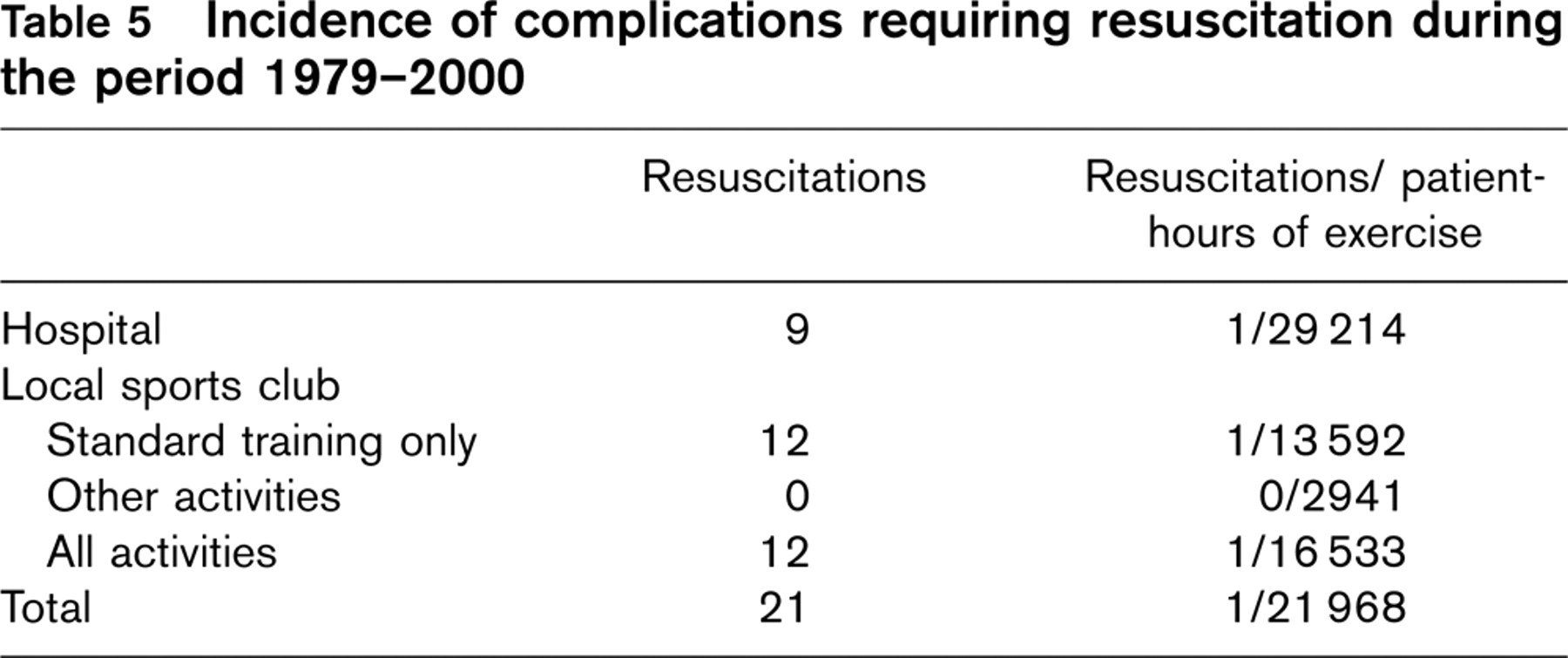
The incidence of complications requiring resuscitation during exercise over 20 years of cardiac rehabilitation and activities of the local sports club for cardiac patients (SC) are summarized in Table 5. In the hospital, 262 925 patient-hours were accumulated, compared with 198 396 patient-hours of exercise at the SC. There were more events at the SC in absolute figures and when expressed in patient-hours of exercise. All events during the SC activities occurred during the indoor and outdoor training.
During the same time period, severe complications not requiring resuscitation also occurred. Four patients experienced an AMI during training (hospital: 2, SC: 2). On seven occasions, a ventricular tachycardia with temporary loss of consciousness but with spontaneous recovery was recorded (hospital: 4, SC: 3). One sustained atrial tachycardia was observed during training at the SC.
The time between the start of the ambulatory rehabilitation programme and the event averaged 402 days in patients who experienced their event in the rehabilitation at the hospital. This exceeds the standard rehabilitation period of 6 months at the hospital, which means that this group included patients who continued the training in the safe environment of the hospital because they were considered to have a high-risk profile for complications.
The patients who were resuscitated at the SC were younger (age 50 ± 8 years versus 56 ± 9 years, not significant) and had a better exercise performance at the start of rehabilitation (2013 ± 571 ml/min versus 1232 ± 388 ml/min, P <0.01) compared with the patients who experienced their event in the hospital. Peak heart rate was higher in patients who experienced the event at the SC (141 ± 25 beats/min versus 108 ± 25 beats/min), although the intake of beta-blocking agents was somewhat higher (45 versus 29%, not significant). Progressions made after the first 3 months of rehabilitation were not significantly different between the two groups.
Incidence of complications requiring resuscitation during the period 1979–2000
Stepwise logistic regression analysis was performed to describe the risk factors for complications requiring resuscitation. The intake of anti-arrhythmics [odds ratio = 5.5; 95% confidence interval (CI) = 1.95–15.51; P < 0.001] and the presence of significant (≤ 1 mm) ST-segment depression during baseline exercise testing (odds ratio = 1.6; 95% CI = 1.21–2.06; P < 0.001) were positively associated with severe complications requiring resuscitation.
Discussion
The first part of the present paper investigated the factors that influence the physical training effects in patients with cardiovascular disease. The individual variability regarding the effects of the cardiac rehabilitation programme with exercise therapy is high. Factors to identify the patients who are likely to benefit most from exercise therapy have been studied in sub-populations of cardiac patients [9–15], but it remains unclear which are the determinants of the improvements in physical exercise performance. Therefore, the present study aimed to identify the determinants of the training effects in cardiac rehabilitation in a large database of patients.
Training effects
An improvement in exercise performance was established after a training period of 3 months: peak VO2 increased with 26%, which is higher compared with results from other studies. The American College of Sports Medicine [5] reported an average increase of 20% in maximal VO2 in CAD patients. One review [3] concluded that a 3-month cardiac rehabilitation period results in an increase in peak VO2 of 15 to 20%. The range and standard deviation of the improvement in peak VO2 in the present study were substantial and show that training responses resulting from exercise therapy differ between patients.
Stepwise regression analysis
Two models were presented as the result of the stepwise regression analysis for the absolute and relative changes in peak VO2. The first model consisted of 11 variables that explained 18% of the absolute changes. The second model contained 12 variables that accounted for 21% of the relative changes. When variables from the baseline exercise test were included, 37% of the variance of absolute changes could be explained. Age and training characteristics appeared as the major predictors for absolute changes in peak VO2. For relative changes, baseline exercise performance was the best determinant followed by training characteristics.
Determinants
There was a significant negative relation between age and improvement in exercise performance in both models. Women, who represented only 7% of the patient-population, made smaller improvements in exercise performance compared with men. These results confirm the findings of one study [5] that found that age and gender were determining factors for training effects. When the effects of age, programme adherence and exercise intensity are ruled out, men still seem to take more profit from cardiac rehabilitation compared with women. Gender can thus be put forward as an independent factor affecting physical training effects in cardiac rehabilitation. The present study did not assess psychosocial factors, which could possibly be of importance in explaining differences between men and women. Nevertheless, one small study [5] in 66 patients found that age and gender were not predictive factors.
Baseline exercise performance, expressed as exercise duration, was a substantial factor in predicting absolute and relative training response. Patients with the lowest initial exercise performance were most likely to show greater improvements. In one study [11], baseline exercise performance (expressed as workload attained) was the only independent predictive variable for improvements in exercise performance in 66 patients with CAD and could account for 24% of the variance. Another study concluded that the group of patients with an initial peak MET level below 5 benefit most from cardiac rehabilitation [20].
The more frequent and the more intense the training was performed, the greater the improvement in exercise performance in both models. For frequency, this is in contrast with the results of one prospective study that compared a high- (10 times a week) versus low- (twice a week) frequency exercise training programme for patients with CAD [21]. They found that VO2 peak improved equally in both programmes. The results of this study should be interpreted with caution, as the difference between the two training conditions is substantial and 10 training sessions of 2 h a week could induce overtraining. The minimal training frequency in order to improve exercise performance in patients with CAD, as recommended by The American College of Sports Medicine, is three times per week [5]. Concerning intensity, the same Position Stand [5] recommends exercise at 55 to 90% of the maximal heart rate, which corresponds to 40 to 85% of maximal aerobic power. Within this range, one study [22] found greater improvements in patients with CAD who trained at a higher intensity (85%) compared with patients who trained at a lower intensity (50%).
Although it is an important factor for survival, former and current smoking is not included in many studies looking for factors that influence training effects. According to both models, current smokers did not benefit as much from cardiac rehabilitation as non-smokers. The question can be raised whether this is an independent effect of smoking, or whether these patients have a different attitude towards rehabilitation, medication and management of risk factors. The reason why former smoking did not appear in the model could be that the majority of the patients in cardiac rehabilitation used to smoke.
Treatment with beta-blocking agents, described as a predictor in one study with AMI patients [8], did not appear to be significantly related to training effects. This is not surprising, as previous studies [23, 24] have shown that the treatment with beta-blocking agents does not impair the improvements in exercise performance in patients with coronary artery disease.
There was a negative relationship between complaints of dyspnoea in daily life at the time of entry into the programme and the prescription of diuretics regarding both absolute and relative training effects. It is probable that these variables refer to patients with heart failure. The presence of dyspnoea could also point to patients with the comorbidity of chronic obstructive pulmonary disease.
Initially, left ventricular ejection fraction was not included in the regression analysis because there were too many missing data for this variable and because it was not relevant for a considerable part of the patient population. A separate analysis was performed to investigate the influence of the contribution of LVEF on physical training effects. It revealed that LVEF was a correlate for absolute, but not for relative changes in peak VO2. In accordance with latter results, other studies [10, 11, 25] have stated that LVEF is not a decisive factor for training effects. Regarding baseline peak VO2, LVEF was not a significant determinant, although a difference was observed for the group of patients with the lowest LVEF. The lack of significance is probably due to the low number of patients in the latter group. It can be concluded that patients with left ventricle dysfunction can benefit from a cardiac rehabilitation programme.
Heart transplantation recipients made less improvement in exercise performance, although significance was not reached for relative improvements. To the best of our knowledge, the training effects in heart transplantation recipients have not been compared with the training effects in a general cardiac rehabilitation population, although some studies [26–29] have reported that these patients respond well to exercise.
The presence of chronic atrial fibrillation or an implanted cardioverter defibrillator were not determinants for the effects of training. This confirms the results of two studies [30, 31], which reported that these conditions did not have any influence on the physical benefits of cardiac rehabilitation.
For further comparison of relative training effects between groups of patients with different pathologies, eight groups were defined. Patients who underwent PTCA and patients who were classified as ‘other' did not improve as much as the groups of patients who underwent CABG and patients with an AMI. This is at least partly due to the higher baseline exercise performance in patients with PTCA, who did not undergo open-chest surgery. The smaller improvements for patients with PTCA compared with patients with CABG have recently been described in one study [32]. The findings of another study [11], which stated that patients with both AMI and CABG had more improvements than patients with AMI alone, could not be confirmed in the present study. The group of patients classified as ‘other' was composed of patients with various pathologies, and therefore it is hard to draw further conclusions from results concerning this group of patients.
Complications
The factors that can predict which cardiac patients are likely to suffer serious complications requiring resuscitation during exercise have not been investigated yet. Furthermore, limited data exist on the incidence of complications requiring resuscitation during exercise activities during and after a cardiac rehabilitation programme. The second aim of the present study was therefore to investigate the determinants for complications requiring resuscitation in cardiac rehabilitation. The incidence of complications from exercise activities at the hospital and at a sports club for cardiac patients was also compared.
Complication rates from a period of 20 years showed that the incidence of events is higher during the activities at the local SC. No complications requiring resuscitation occurred during swimming, volleyball and walking. Possibly, the intensity of these activities is not as high as in the standard indoor and outdoor training sessions. The complication rate for the activities of the ambulatory rehabilitation programme is one per 29 214 patient-hours, which is similar to findings in the literature. Data on complications during exercise in cardiac rehabilitation are scarce, but comparison can be made with the data of Cantwell [16], who described three cardiac arrests in 93 679 patient-hours of training in cardiac rehabilitation or one per 31 226 patient-hours of exercise. Two studies gathered data from rehabilitation programmes by means of a questionnaire or a telephone interview: one [17] found one event per 111 996 patients-hours exercise; the other study described one per 32 593 patient-hours of exercise [18]. The validity of these data can be questioned because of the methods used and the lack of data about exercise intensity. To the best of our knowledge, no data exist on complications during exercise activities after a hospital-based ambulatory cardiac rehabilitation programme.
The time between the start of the phase II rehabilitation at the hospital and the event in patients training at the hospital averaged 1.1 years. This exceeds the standard rehabilitation period of 6 months at the hospital: these patients continued the training in the safe environment of the hospital because they were considered to have a high-risk profile for complications. However, the incidence of events was lower in these patients with a higher risk profile, compared with patients training at the SC. The time to event was much longer in the patients training at the SC (6.5 years), suggesting that the cause of the complications is different. It might be that recurrent medical problems are responsible for complications in patients training at the SC.
Two factors were predictive for an event requiring resuscitation. Patients taking anti-arrhythmics, not including beta-blocking agents, still had a five times greater chance of serious complications. Furthermore, the presence of significant ST-segment depression at baseline exercise testing was connected with serious events, indicating a remaining oxygen deficit of the heart.
Conclusions
Age and training characteristics were the strongest predictors for absolute changes in peak VO2. Baseline exercise performance was the best determinant for relative changes, followed by training characteristics.
The intake of anti-arrhythmic agents and the presence of ST-segment depression at baseline exercise testing are predictive for complications requiring resuscitation during exercise activities during and after cardiac rehabilitation. The occurrence of complications requiring resuscitation during training was higher in the sports club for cardiac patients, compared with rehabilitation activities at the hospital. Safety measures should therefore be emphasized continuously, especially after the traditional reconditioning phase.
Footnotes
Acknowledgements
This study is granted by the Flemish Fund for Scientific Research (grant G.0124.02) (Belgium) and by the Research Council of the Catholic University of Leuven (grant OT/01/46) (Belgium). L.V. is holder of the ‘Faculty Chair Health and Lifestyle' of the Faculty of Health Care of the University of Professional Education, Utrecht (The Netherlands). J.D. is Research Assistant of the Flemish Fund for Scientific Research. R.F. is holder of the Professor A. Amery Chair in Hypertension Research, founded by Merck, Sharp and Dohme (Belgium).