
Abstract
Background
The purpose of this study was to explore the duration of the association of major coronary risk factors measured on a single occasion with coronary heart disease (CHD) deaths during 40 years in a population sample of middle-aged men.
Design
Measurement of age, systolic blood pressure, serum total cholesterol, and cigarette smoking was made on a single occasion in 2376 cardiovascular disease free men, aged 40-59, belonging to the US Railroad cohort of the Seven Countries Study enrolled in the late 1950s. During 40 years of follow up 627 men died from typical CHD (sudden death coronary death or definite myocardial infarction).
Methods
Eight partitioned proportional hazards models were solved, one for each independent 5-year block of follow up, to predict the risk of CHD death. Eight 5-year partitioned hazard scores, derived from the coefficients, were cumulated for each risk factor.
Results
The resulting curves showed a regularly increasing time trend in risk for coronary deaths as a function of serum cholesterol, systolic blood pressure and cigarette smoking, for the first 30-35 years of follow up followed by a loss of predictive power thereafter. The curves fit straight lines, with large squared correlation coefficients ranging from 0.96 to 0.99. There was a relatively constant strength in the association of risk factors levels with events, which are predicted irrespective of the distance from risk factor measurements.
Conclusions
Measurement of major coronary risk factors taken on a single occasion in middle-aged men maintained a regular and almost monotonic relationship with the subsequent occurrence of CHD deaths for at least 30-35 years of follow up.
Introduction
In a preliminary analysis dealing with 40-year follow-up mortality of the US Railroad cohort of the Seven Countries Study, it was shown that baseline measurement of age, serum cholesterol, systolic blood pressure and cigarette smoking was strongly associated with coronary heart disease (CHD) mortality [1].
That analysis was run on cumulated events and could not show any time trend in the strength of the association. In fact, using as endpoint all events for the whole follow up, could not address possible time dependency in the hazard. That relationship could be regular and monotonic, or strong in early phases of the follow up and then less so, or null or even negative. These findings said only that, on average, there was a positive and significant overall association between risk factors and events.
Relatively simple statistical techniques can be used to describe the time trend of the association. In this analysis we hypothesized that major risk factors measured on one occasion in middle age were associated with 40-year CHD deaths in a monotonic fashion during the follow-up period.
Material and methods
The cohort was enrolled between 1957 and 1960 from railroad companies located in the midwest and northwest of the United States [2]. The roster was based on the identification of defined job profiles.
A total of 2571 men aged 40 to 59 were examined, corresponding to a participation rate of 75%. Individual characteristics considered for this analysis were (1) age in years, rounded to the nearest birthday; (2) systolic blood pressure in mmHg, as an average of two consecutive measurements taken by trained physicians, using a mercury sphygmomanometer, in supine position, at the end of a physical examination following procedures described in the WHO Cardiovascular Survey Methods Manual [3]; (3) serum cholesterol in mmol/l, measured in a casual blood sample using the method of Abell and Kendall as modified by Anderson and Keys [4]; and (4) smoking habits, derived from a questionnaire and estimating the current average number of cigarettes smoked per day.
Periodic checks were made on vital status in cooperation with the Railroad Retirement Board, to identify dates and causes of death. When causes of death were not reported, enquiries were made with the Departments of Health of the different States. During the first 5 years the quality of causes of death was checked against hospital discharge records, with satisfactory results [5]. The 40-year follow up for mortality was completed using the National Mortality Index to identify a few cases that were not detected by other procedures. There were no losses to follow up.
Causes of death were coded following the 8th Revision of the WHO-ICD [6] by one of the authors (HB) for the first 5 years and by another author (AM) for the remaining period, following pre-defined rules, mainly for the diagnosis of cardiovascular deaths. In case of multiple causes a hierarchical rule was adopted with violent causes, cancer in advanced stages, coronary heart disease, stroke and other causes taking precedence, in that order.
The mortality endpoint considered for the present study was coronary heart disease (cases classified as coronary heart disease or sudden death of possible coronary origin when other possible causes could be excluded). Subjects with any cardiovascular disease of atherosclerotic origin at entry examination were excluded from the analysis. Baseline data were collected in the 1950s before the era of the Helsinki Declaration. Oral informed consent was obtained prior to collecting follow-up data. The analysis was finally run among 2376 men free from cardiovascular diseases at entry and having all four risk factors measured.
The analysis was conducted using the Cox proportional hazards model [7] as available from the NCSS-97 statistical package [8] following two steps: (1) a model was first produced using all events in 40 years of follow up, as a function of baseline risk factors measurement; (2) then, eight different solutions were computed, each dealing with events occurring in subsequent and independent blocks of 5 years – for a total of 40 years – corresponding to the so-called partitioned or segmented modelling approach.
In the first step, subjects who died from nonCHD causes were automatically dropped from the denominator at the time of the event, as censored cases. In the second step those who died before the explored quinquennium of follow up were excluded from the denominator, while those who died in that quinquennium interval from causes other than coronary were treated as censored cases.
The coefficients for each risk factor and for each 5-year block of follow up were tested for heterogeneity [9]. A hazard score was created by subtracting 1 from the hazards ratios for one unit of measurement for each risk factor. Hazard scores were sequentially cumulated and plotted against time. They are not cumulative hazard functions. Confidence intervals around the scores were estimated from the standard errors of the coefficients and were also cumulated. Linear regression equations of cumulated hazard scores on time were computed, forcing the line through the origin of axes.
Results
During 40 years of follow up, on a total of 2376 subjects considered in the analysis there were 627 coronary deaths (out of 1966 overall deaths). A proportional hazards solution with all CHD deaths in 40 years as end-point versus all risk factors is given at the top of Table 1. The coefficients for all four factors are positive and statistically significant, accompanied by large hazards ratios.
Table 1 also gives the solutions of the eight proportional hazards models each dealing with an independent quinquennium of follow up. In the eight models, the coefficients for age and systolic blood pressure are significant on seven occasions; those for cholesterol and cigarette smoking on six occasions.
Solutions of the proportional hazards model for the whole period and for eight periods of 5 years each, with CHD deaths as end-point and four risk factors as covariates. Deltas for computing the hazard ratios are: 5 years for age; 20mmHg for systolic blood pressure; 1 mmol/l for serum cholesterol; 10 cigarettes per day for smoking habits
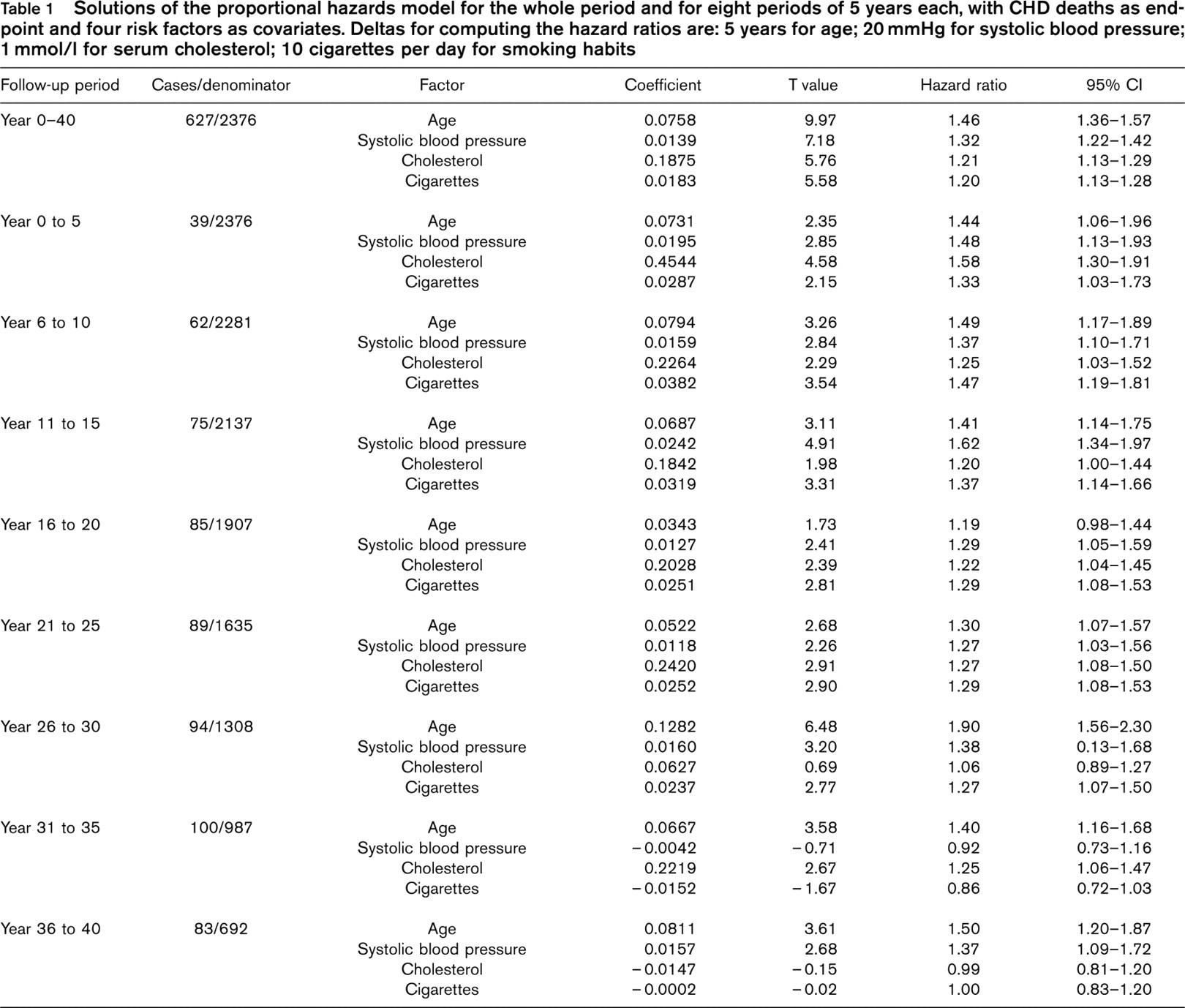
The coefficient of age is not statistically significant during the period 16 to 20 years. Cholesterol is unrelated to CHD mortality between years 36–40 and smoking is unrelated between years 31–40. Systolic blood pressure has a hazard rate ratio less than 1 between years 31–35, but substantially above 1 in the final quinquennium of follow up.
A test of heterogeneity applied to the coefficients of each risk factor of the different solutions gave P- values of 0.0704 for age, 0.0376 for systolic blood pressure, 0.0526 for serum cholesterol and 0.0008 for cigarette smoking. The hypothesis of heterogeneity among coefficients could not be rejected for systolic blood pressure, serum cholesterol and smoking habits. This was mainly due to the contribution of the third and the seventh quinquennia for systolic blood pressure, the first and the eighth quinquennia for serum cholesterol, and the contribution of the seventh and eighth quinquennia for cigarette smoking.
The cumulated hazard scores for a unit of each risk factor are graphically shown in Figure 1, together with their 95% confidence intervals and a fitted straight line forced at the origin of the axes. Figures should be read considering that, for each 5-year step, the steepness of the slope describes the strength of the association of baseline risk factors levels with events for the subsequent 5 years, on average.
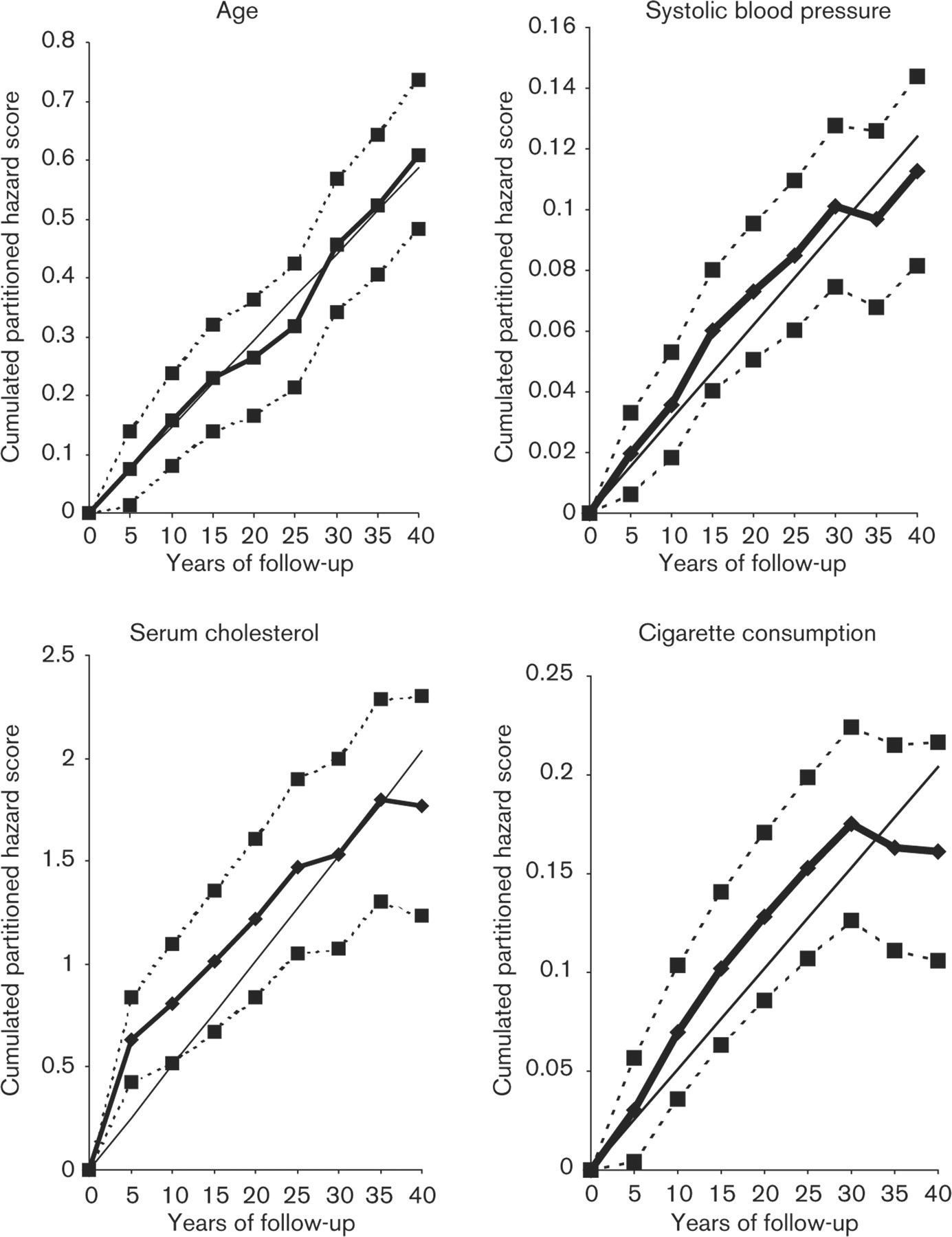
The cumulated partitioned hazard score for age, systolic blood pressure, serum cholesterol and cigarette smoking predicting CHD mortality risk during eight 5-year periods. R squared for the regression line are 0.99, 0.99, 0.97 and 0.96 respectively.
Time trends of cumulated hazard ratio score for age rises regularly during the eight quiquennia. Time trends of cumulated hazard ratio score for systolic blood pressure rises regularly until year 30, shows a steady state during the next 5 years, but it increases regularly again between year 35 and year 40 of follow up. The cumulated hazard ratio score for serum cholesterol increases sharply during the first 5 years, then regularly, although to a lesser degree, between year 5 and 35 and becomes flat during the last 5 years of follow up. The shape of the curve for cigarette smoking is regularly increasing during the first 30 years while thereafter it becomes flat.
The regression lines suggest good fits, corresponding to large values of R squared that are of 0.96 or more. However, the association of cholesterol and smoking habits becomes definitely weaker or null after 35 or 30 years of follow up.
Discussion
The above findings suggest that four major risk factor baseline levels – age, systolic blood pressure, serum cholesterol and cigarette smoking – are associated through a relatively constant relationship with the occurrence of CHD deaths during a 40-year follow up. This is fully true for the first 30 years, while later smoking habits tend to lose their association with CHD mortality risk, and the same happens to serum cholesterol after 35 years. A relatively uniform relationship could be expected only for age, as actually found.
The curves describing this phenomenon are interpreted as the strength and stability of the relationship of baseline risk factor levels with fatal events at each subsequent time block. This time interval is relatively long (5 years) but despite this there are irregularities in the risk factor/event relationship partly explainable by the small number of events found in each period years of follow up.
On the other hand, the straight lines fitted to the data provide large correlation coefficients suggesting a relatively monotonic and regular relationship between risk factor levels and CHD mortality risk at least for the first 30 years of follow up. The test of heterogeneity among coefficients of the same factors, as estimated for different time periods, helps in showing that the association between entry risk factor levels and events may vary during the follow up, losing strength during the last two quinquennia.
Some relationships may not be linear across the whole time period. This could be interpreted as a nonlinear relationship or the consequence of selection due the role of specific risk factors, such as systolic blood pressure and smoking habits, potentially important also for noncor-onary death risk. Also changes in risk factor levels may have a role in changing the strength of the baseline measurements with late events.
The use only of baseline measurements in longitudinal studies tends to underestimate the associations between risk factors levels and CHD rates, due to regression dilution effects [10]. However the application of this procedure in the partitioned analysis adds nothing substantial to the question since adjustment for regression-dilution bias would have been uniform for each time-period of the follow up.
On the other hand, the strength of the association during the eight subsequent time periods could be influenced by changes in risk factor levels that occurred during the follow up, but unfortunately only baseline and 5-year examinations are available for this cohort. The probable increasing use of antihypertensive drugs during the last decades might also have influenced the relationship of blood pressure with CHD events. For smoking habits the expectation is a decline of prevalence with ageing, while for serum cholesterol mean levels usually tend to stabilize or decline after the age of 60.
The problem of predicting early versus distant events has been considered in other studies using various approaches [11–20.
A technique similar to that employed here was used on data of the Italian Rural Areas of the Seven Countries, considering several risk factors, slightly different end-point and time intervals, but reaching similar conclusions [11–13.
Other studies used entirely different approaches and techniques to look at the relationship of entry risk factor levels with early versus late events.
In the Honolulu Heart Study in middle-aged men, early events were segregated from late events on the basis of age at the time of event (under 60 years, and 60 or over) [14]. Systolic blood pressure, alcohol intake, serum cholesterol, serum glucose and cigarette smoking were independent predictors for both early and late onset coronary events. On the other hand cigarette smoking had a smaller effect on late events, while serum triglycerides were predictors only of early events.
In the 25-year follow up of the Finnish cohorts of the Seven Countries Study, the association of baseline serum cholesterol with coronary mortality has a similar strength during the first 10 years and the subsequent 15 years of follow up [15]. When the analysis was extended to 30-year follow-up data, breaking down the time of observation into three decades, it was shown that baseline serum cholesterol and smoking habits were strong predictors of CHD death, either early and late, during the follow up, while baseline systolic blood pressure was no longer associated with CHD deaths after 20 years. Only after 20 years did baseline body mass index become directly associated with events [16].
An analysis of the Whitehall Study in the UK, showed that, for a given age at death, the longer the gap between cholesterol measurement and death the more predictive became the cholesterol concentration for coronary heart disease and all-cause mortality. This confirmed that a single measurement taken earlier in life holds predictive power for many years [17].
In the Chicago Heart Association Detection Project in Industry [18] distant follow-up events were predicted with the same strength as near follow-up events by baseline measurements of blood pressure, serum cholesterol and smoking habits.
In a British study the role of risk factors with increasing length of follow up was analysed in a way rather similar to that used by us, reaching similar findings, at least for the first 15 years of follow up [19].
More recently the role of antecedent blood pressure levels was recognized as a predictor of cardiovascular diseases in the Framingham Study [20].
Findings reported in the literature and those added by our analysis may help in interpreting the predictive power of risk factors in the elderly. The association of serum cholesterol levels and blood pressure with CHD events has been long debated and seems of uncertain interpretation [21–24. We are dealing with two entirely different questions: (1) whether a single measurement in adulthood keeps predictive power until very old ages; and (2) whether measurements taken in the elderly are able to predict the occurrence of events during subsequent years. The first question can likely be answered by stating that some risk factors keep a very long association even with very distant events, occurring in advanced ages. This seems to be true during as much as 30 years for smoking habits, 35 years for serum cholesterol and probably 40 years for systolic blood pressure. This means also that measurements taken at age 40 to 59 years are predictive when the individuals have a fatal event at age 80 and more.
The answer to the second question about risk factor levels in the elderly cannot be given by this analysis. However, at least for blood pressure, a recent meta-analysis involving huge numbers of individuals and events suggests that even measurements taken in old ages maintain a distinct, although lower, predictive power [25].
The fact that a measurement of a risk factor taken on a single in middle-aged men keeps its predictive power for a long time is not in contrast with the contribution that changes in risk factor levels can provide to the prediction of late events. An analysis run on the first 25 years of follow up of the Italian Rural Areas of the Seven Countries Study [26] showed that in a multivariate model both baseline values and indicators of 10-year change in risk factor levels were predictive of major CHD events during the subsequent 15 years.
Why a single measurement of some risk factors keeps such a long memory is not easy to explain. Levels of a personal characteristic in middle age may change during time, but at that age they likely reflect the personal history up to middle age and are indicative of a given amount of damage already established which maintains strength and predictive value for a long time. This does not negate the possible influence of changing levels of modifiable risk factors, but warns of the need to consider also their past levels whose association with the occurrence of events may last for life.
Footnotes
Acknowledgements
The authors acknowledge Professor Ancel Keys, Minneapolis, the founder of the Seven Countries Study, and the late Professor Henry Taylor, principal investigator of the US Railroad Study, for their historical contribution to the study. The authors also acknowledge Ms Rosemarie Hilk, Division of Epidemiology, University of Minnesota, Minneapolis, for her contribution in collection of mortality data.