
Abstract
Background
Despite evidence of its benefits, attendance at cardiac rehabilitation (CR) programmes is poor. Past studies to identify predictors of non-attendance have been limited by their small sample size, particularly for female patients. The present study was designed to identify socio-demographic and clinical predictors of non-attendance and drop-out separately for men and women automatically referred to CR programmes.
Method and subjects
Prospective study of CR programme attendance amongst 808 patients consecutively admitted over an 11-month period to one of two hospitals in Melbourne, Australia, after acute myocardial infarction (AMI), or to undergo coronary artery bypass graft surgery (CABGS) or percutaneous coronary intervention (PCI).
Results
Of the 652 eligible patients, 573 (88%) were successfully tracked at 4 months. Of these, 284 (49.6%) had attended a CR programme, while 272 (47.5%) had not. Using logistic regression, the significant predictors of programme non-attendance among men were having had a PCI, being a non-driver, and being aged 70 or more. The only factor predictive of non-attendance for women was being aged 70 or more. Amongst attenders, 67 (23.6%) patients discontinued the programme. Being a smoker, having diabetes and being unemployed at the time of hospital admission were predictive of programme drop-out by men. Being physically inactive at admission was predictive of programme drop-out by women.
Conclusions
The present study demonstrated a relatively high rate of CR programme attendance. Special attention needs to be directed towards males who are older, PCI patients, smokers, unemployed or non-drivers, and females who are older or inactive.
Keywords
Introduction
It is widely accepted that cardiac rehabilitation (CR) programmes can facilitate physical and psychological recovery following acute cardiac events [1–5], with similar benefits being produced from high and low intensity exercise programmes [6–9]. As well as improving quality of life, such programmes encourage behaviour change and adherence to regimens, thereby providing a strong foundation for secondary prevention of cardiovascular diseases (CVD) [1, 5].
Australia has an extensive network of outpatient CR programmes providing exercise, education and support. Nearly all are conducted in groups and are based upon low to moderate intensity exercise. Education sessions include discussion of CVD risk factors, symptoms, medication and other medical issues, nutrition, activities of daily living, emotional responses to the acute event, return to work and impact upon the family. Individual dietary or other counselling is available, as required. Patients attend both the exercise and education components. Programmes usually commence within a few weeks of the patient's discharge from hospital and are held once per week, continuing for 6 to 8 weeks [10]. Most programmes are offered free of charge, with the exception of those provided in private hospitals. Unfortunately, attendance at CR programmes is poor, both in Australia and elsewhere. Participation rates range from 21% [11] to 75% [12], with most being between 25 and 50% [13–19].
Participation is particularly low for some patient groups. Specifically, poorer attendance among patients who have had percutaneous coronary intervention (PCI) is generally reported [13, 20, 21]. Patients who smoke [22, 23] or are physically inactive [16] also commonly fail to attend programmes. Older patients are less likely to attend than younger patients [14, 15, 17, 21, 24, 25]. Although men and women achieve similar benefits from participation [26, 27], non-attendance and drop-out are more common among women [12, 15–17, 26, 28, 29]. Lower uptake of programmes has also been reported for patients who are unmarried [15, 16, 19, 30], unemployed [14–16], less well educated [11, 15, 31], of lower socio-economic status [25, 31], socially deprived [16, 32, 33], non-English-speaking [20], non-car drivers [34] or living some distance from the programme venue [11, 35].
Given the different attendance patterns for men and women, it is likely that different factors operate to inhibit their participation. Most importantly, there is some evidence of lower referral rates for women [21, 26, 36]. However, the few studies investigating predictors of non-attendance separately for men and for women have been limited by their small sample size [36, 37]. Indeed, the low rates of referral of women increase the difficulty of obtaining a sufficiently large sample of female participants. The present study was designed to identify the predictors of non-attendance and drop-out separately for men and women.
This paper reports the findings of a prospective study of patterns of attendance among patients who had experienced an acute cardiac event and were referred to outpatient CR programmes. All CR programmes comprised a 45-min exercise session of low intensity and a 45–60-min education session, with both components conducted in groups. Referrals were automatic rather than dependent upon specific physician referral, thereby potentially maximizing recruitment. Automatic referral means that all patients who have had an acute cardiac event [acute myocardial infarction (AMI), coronary artery bypass graft (CABGS) or percutaneous coronary intervention (PCI)] are approached by the cardiac rehabilitation programme coordinator, cardiologist/surgeon or other delegated member of the programme team, to advise them about the existence of the programme and encourage them to attend. This approach is widespread in Australia and consistent with policies of the World Health Organization [38] and the National Heart Foundation of Australia [39], which advocate that all patients, irrespective of age, should be offered a group programme of low to moderate intensity exercise and education following their acute cardiac event, tailored to suit their individual requirements. It was anticipated that the key socio-demographic and clinical predictors of non-attendance and drop-out might be more clearly identified in our population with automatic referral and no physician selection bias.
Method
Study population
Eligible subjects were patients who were consecutively admitted over an 11-month period to two major teaching hospitals in one metropolitan region following AMI or to undergo CABGS or PCI. Revascularization took place in only one of the two hospitals. Confirmation of eligibility was made by checking discharge records of diagnosis. In cases where patients experienced more than one cardiac event, classification was based on the first hospital admission.
Informed consent
The protocol for the study was approved by the human research ethics committees of both hospitals. Written consent was sought from each patient for the study team to conduct a brief interview in hospital, to access hospital medical records and to contact the patient a few months later to investigate progress. During interviews in hospital, CR was not mentioned in order to avoid a possible influence upon later attendance at an outpatient programme.
Baseline data collection
Baseline interviews were conducted with patients to investigate socio-demographic, medical and behavioural characteristics. Interviews were carried out in hospital (49%) or by telephone immediately after hospital discharge (32%) if patients had been discharged early or unexpectedly transferred to another hospital. Bilingual interviewers were used as required. In the remaining cases, it was necessary to gather information by postal questionnaires (1%) or, if eligibility was determined only later from discharge summaries, from medical records (17%), in which case minimal data only could be collected. Assessment of health behaviours and risk factor status was based upon self-report, using questions and protocols taken from previous national surveys of the prevalence of cardiovascular disease risk factors [40].
Follow-up data collection
Follow-up of patients took place 4 months after hospital admission. Initially, the CR programme coordinators of the two recruiting hospitals were consulted and their CR programme attendance records checked to determine whether or not patients in the study had participated in a CR programme during convalescence. Attendance records of other centres to which some patients had been referred were also checked. Where hospital records were incomplete or unclear, patients were approached directly by telephone (n = 231, 40%) or letter (n = 25, 4%) to determine attendance status.
Variables
Dependent variables
A dichotomous ‘attendance' variable was used to classify (1) those who attended one or more sessions of group exercise and education provided by the programme (attenders), and (2) those who did not attend any sessions (non-attenders). Amongst attenders, a dichotomous ‘drop-out' variable was used to distinguish between (1) those who attended at least 50% of the available sessions (continuers), and (2) those who attended less than 50% of the sessions (drop-outs). This cut-off point is consistent with that used previously to define ongoing attendance/drop-out [16, 23].
Independent variables
All independent variables were baseline characteristics identified a priori on the basis of research findings as potentially associated with attendance and/or drop-out. They were:
Socio-demographic factors including age (< 70/ ≤ 70 years), gender (men/women), marital status (married/ separated or divorced/widowed/never married), living arrangements (with partner/with others/alone/hostel), language spoken at home (English/other), education (upper secondary/lower secondary/primary or none), employment status (employed/unemployed/retired/ home duties), current or last occupation when in workforce (non-manual/manual) [41], car driver (driver/non-driver);
Diagnosis (AMI, CABGS, PCI);
Self-reported risk factors at admission, including high blood pressure (yes/no), high cholesterol (yes/no), positive family history (yes/no), obesity defined using body mass index (BMI > 30/BMI ≤ 30 kg/m2 [42]), diabetes (yes/no), smoking status (current smoker/ former smoker/never smoked), and physical inactivity (no activity/up to 6 h per week/ ≤ 6 h per week).
Statistical analyses
The data were analysed using SPSSx 10.0. Differences between men and women were analysed using χ2 tests. All subsequent analyses were undertaken separately for men and women. Differences between attenders and non-attenders, and between continuers and drop-outs were assessed using χ2 tests. The significance level was set at P < 0.05. Significant variables from univariate comparisons were entered into separate forced-entry logistic regression analyses to predict attendance and drop-out respectively. This two-step approach has been used in several previous studies [14, 23, 32].
Results
Participation rate for the follow-up study
During the study period there were 808 patients admitted to either of the two hospitals with an acute cardiac event. Of these, 136 (17%) were excluded from the study at baseline because of death (n = 86), refusal to participate (n = 25), language difficulties (n = 18) and physical illness (n = 7). A further 20 (2%) died following recruitment. Of the remaining 652 patients, 573 were successfully tracked 4 months after hospital discharge and CR attendance data were documented. There were 79 non-responders who either could not be located or did not return the questionnaire (n = 65), refused to participate (n = 2), or were unable to complete the questionnaire due to language difficulties (n = 10) or illness (n = 2). Thus, there was an 88% follow-up rate among known survivors in the study. Those not tracked were more likely to be living alone (P = 0.048), non-English speaking (P = 0.011), non-drivers (P < 0.001), AMI patients (P = 0.002) or to have diabetes (P = 0.004).
Rates of programme attendance
Of the 573 patients who were tracked, 284 (49.6%) attended at least one session of the CR programme offered to them (attenders): this group comprised 217 ‘continuers' and 67 ‘drop-outs'. Thus, there was a dropout rate of 23.6% amongst attenders. There were a further 272 (47.5%) patients who did not attend any sessions (non-attenders). These three groups accounted for 97% of the total follow-up sample. There were inadequate CR records from which to ascertain attendance status for the remaining 17 (3%) patients, who were therefore withdrawn from subsequent analyses. Importantly, attendance differed significantly in terms of diagnostic group (P < 0.001), with attendance rates of 66.2% for CABGS patients, 51.1% for AMI patients, and 25.0% for PCI patients. Figure 1 sets out the distribution of patients who were eligible, included, excluded, eligible for tracking, tracked and classified.
Baseline characteristics of patient population
Baseline characteristics are shown in Table 1. Ages of patients ranged from 20 to 93, with a mean age of 64.9 ± 12.1 years. The majority (70%) of patients were men. The demographic profile presented here is similar to that of patients included in other recently published Australian studies investigating CR attendance [18, 19], in terms of age, ethnicity, marital status, living arrangements and employment status. Significant gender differences were found for many of the baseline characteristics (Tables 1 and 2), as expected. Subsequent analyses were conducted separately for men and women.
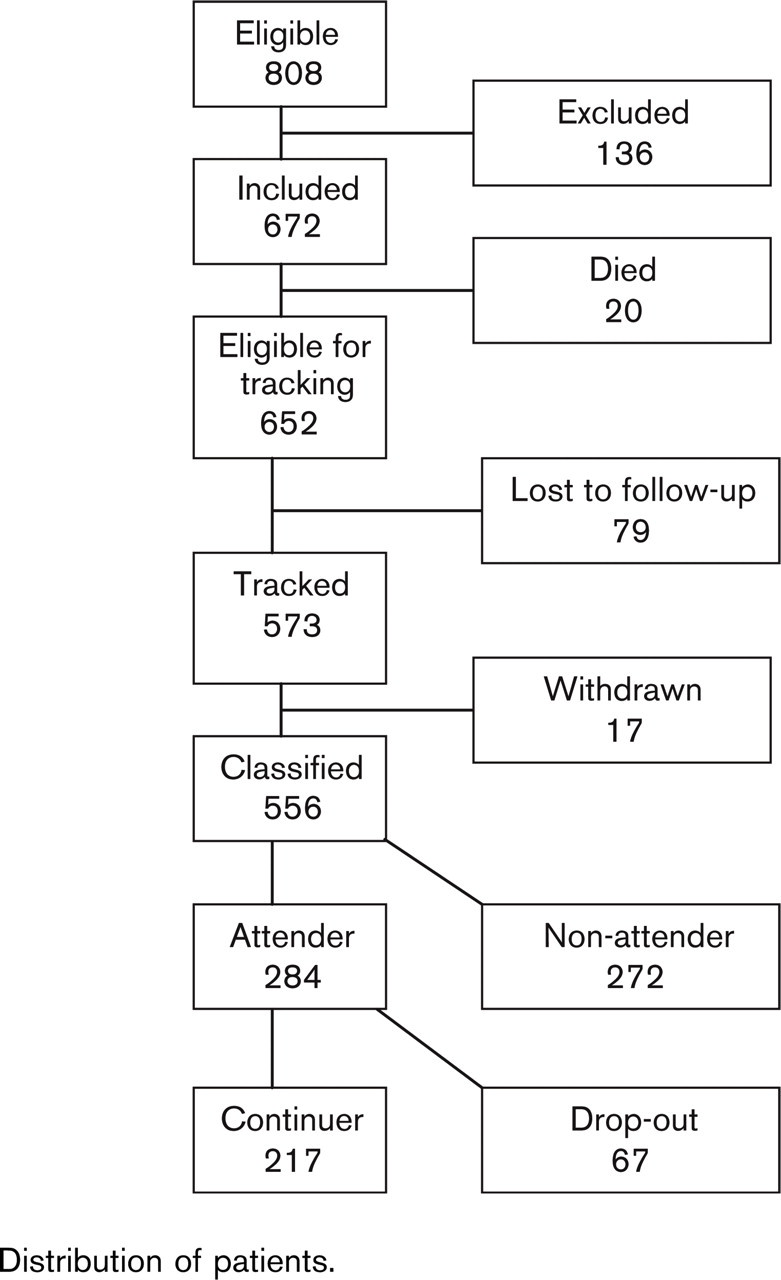
Distribution of patients.
Baseline socio-demographic characteristics of males and females
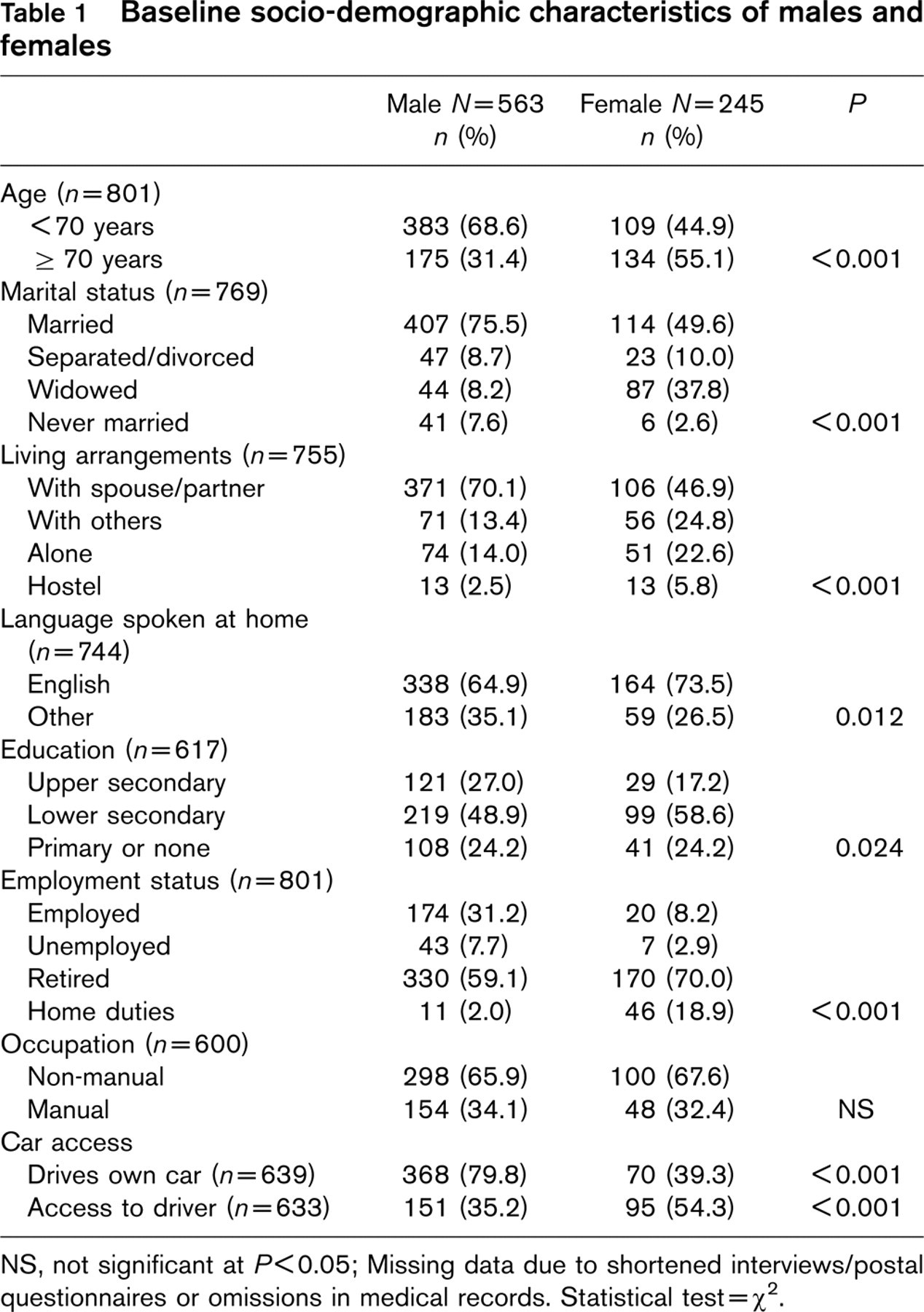
NS, not significant at P < 0.05; Missing data due to shortened interviews/postal questionnaires or omissions in medical records. Statistical test = χ2.
Women were older than men, were more likely to live alone, to be widowed and to speak English as a first language. Men were more likely to be married, to have had upper secondary school education and to be employed. Further, men were more likely to drive their own car, whereas women were more likely to have regular access to another driver (Table 1). Women were more likely to have had an AMI, high blood pressure, diabetes, to have never smoked and to have been physically inactive prior to admission. Men were more likely to have undergone CABGS and to be former smokers (Table 2).
Factors associated with programme non-attendance
Women were less likely than men to attend a programme, with attendance rates of 44.9 and 53.4%, respectively (P = 0.049). Univariate analyses revealed that, for men, non-attendance was significantly associated with being 70 years of age or more (P < 0.001), being unemployed (P = 0.044), not driving a car (P < 0.001), having had PCI or an AMI (P < 0.001), and not having a positive family history of heart disease (P < 0.007). In logistic regression, three factors were significantly and independently predictive of non-attendance amongst men, namely age, diagnosis and driver status. Having undergone PCI or, to a lesser extent, having had an AMI, being a non-driver, and being aged over 70 years all reduced the likelihood of attendance (Table 3).
Univariate analyses revealed that, for women, non-attendance was significantly associated with being 70 years of age or more (P < 0.001), being a non-driver (P = 0.013), not having elevated cholesterol (P = 0.014) and having diabetes (P = 0.013). In logistic regression, age remained the only significant and independent predictor of non-attendance, with older age reducing the likelihood of women attending (Table 3).
Factors associated with programme drop-out
Amongst attenders, 24.3% of men and 21.2% of women were classified as ‘drop-outs', with no significant gender difference in drop-out rate. Univariate analyses revealed that, for men, drop-out was significantly associated with being unemployed (P = 0.025), being a smoker at the time of admission (P = 0.027) and having diabetes (P = 0.006). In logistic regression, all three variables were significantly and independently predictive of dropout by men, all increasing the likelihood of drop-out (Table 4).
Univariate analyses revealed that, for women, drop-out was associated with being physically inactive prior to admission (P = 0.047). Activity level remained significant in the logistic regression, with women who had been undertaking no physical activity having an increased likelihood of drop-out (Table 4). For all logistic regression models, Hosmer and Lemeshow Goodness-of-Fit Tests produced low and non-significant chi-square values, indicating good model fit.
Baseline medical characteristics of males and females
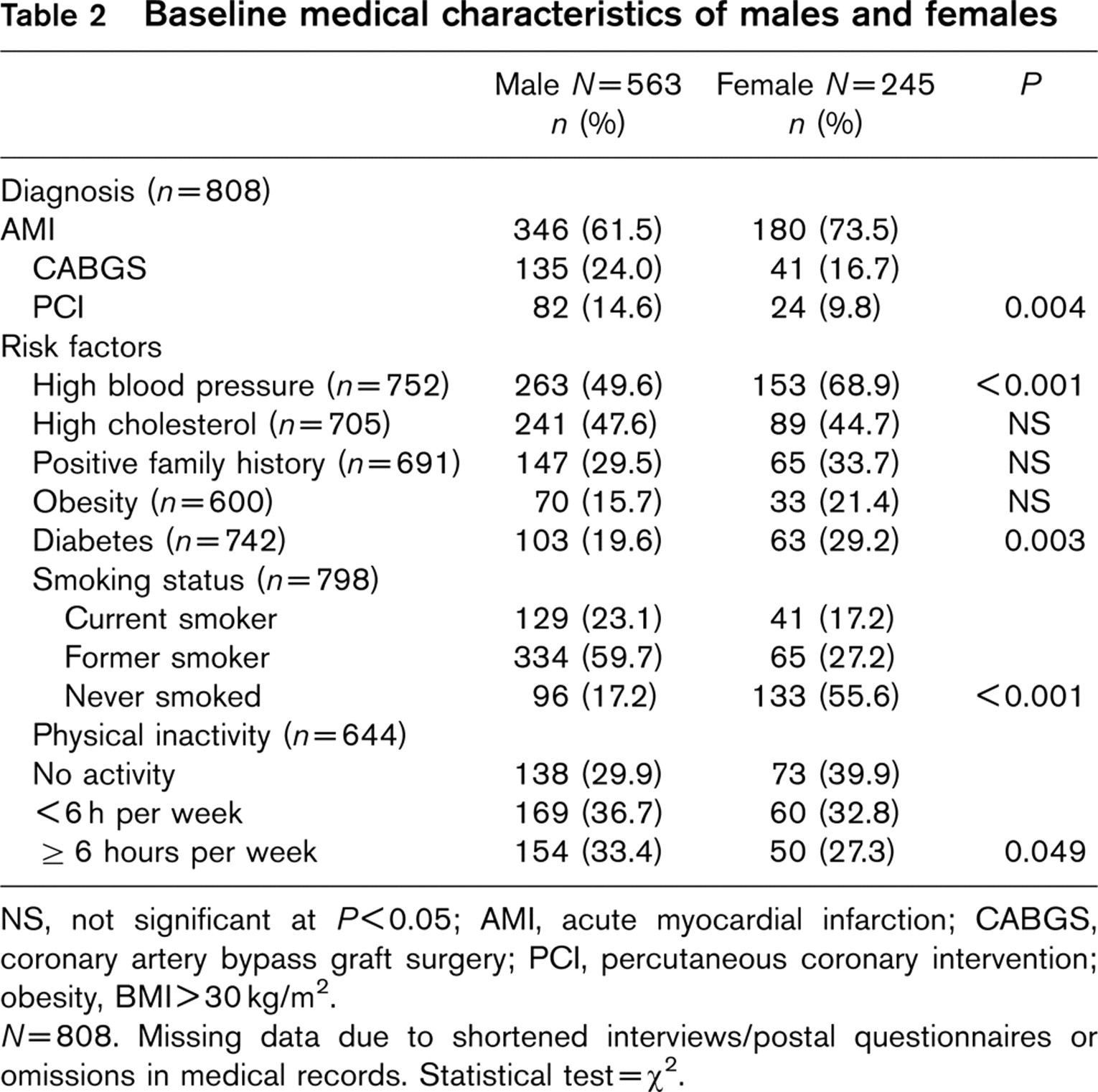
NS, not significant at P < 0.05; AMI, acute myocardial infarction; CABGS, coronary artery bypass graft surgery; PCI, percutaneous coronary intervention; obesity, BMI>30kg/m2.
N = 808. Missing data due to shortened interviews/postal questionnaires or omissions in medical records. Statistical test = χ2.
Predictors of non-attendance
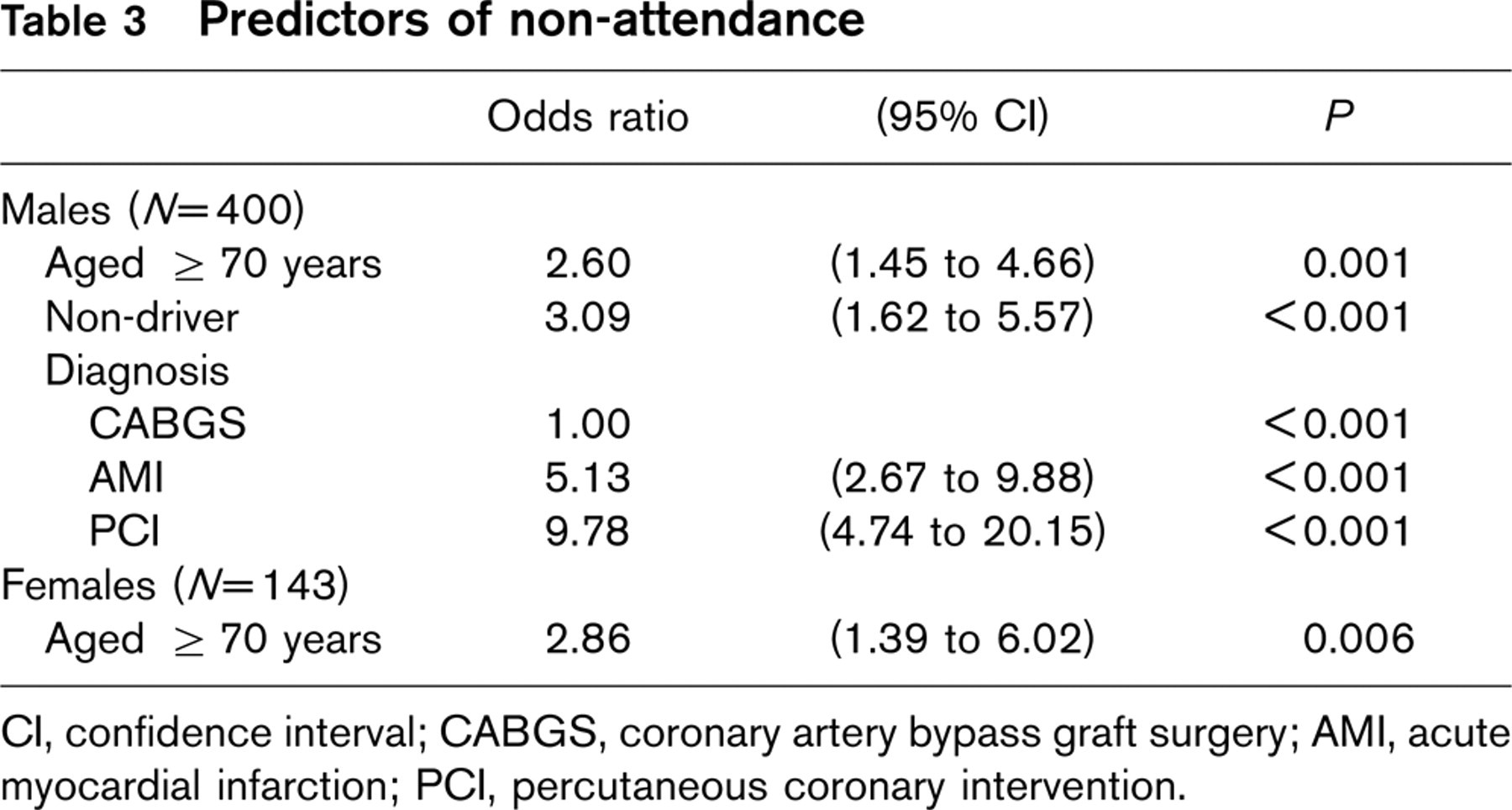
CI, confidence interval; CABGS, coronary artery bypass graft surgery; AMI, acute myocardial infarction; PCI, percutaneous coronary intervention.
Predictors of drop-out
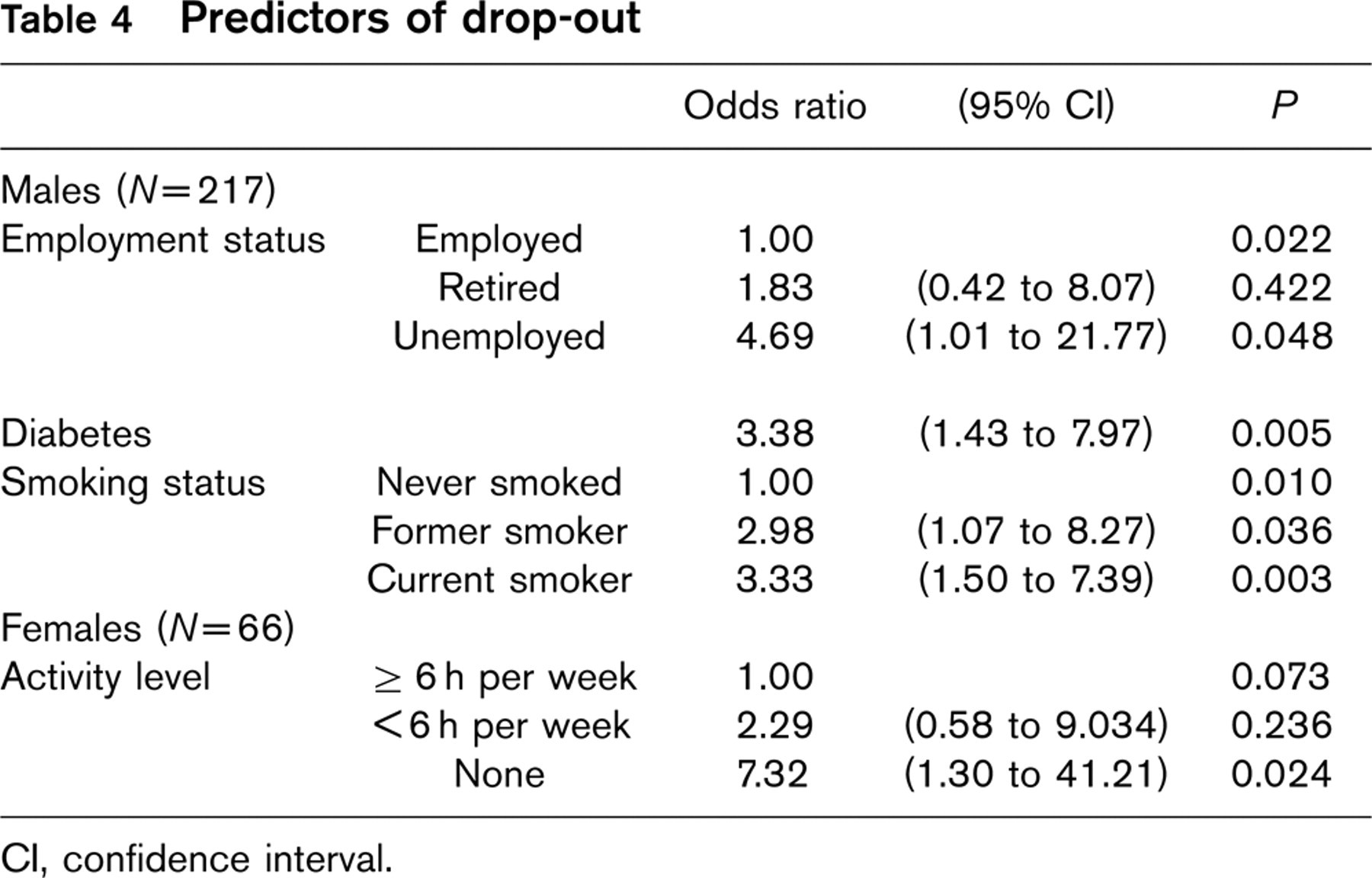
CI, confidence interval.
Discussion
Most past studies of participation in CR programmes have been confined to those patients who were formally referred to programmes by their physicians. Because a policy of routine referral applied at the hospitals in our study, we were able to investigate attendance patterns in a larger population that had no physician selection bias. Thus, the overall attendance rate of 49.6% (53.4% for men and 44.9% for women) represents a higher level of participation than that reported in most previous studies. The overall drop-out rate of 23.6% (24.3% for men and 21.2% for women) is comparable with previous reports.
The lower attendance rate amongst women supports findings of many previous studies of programme uptake [12, 15–17, 26]. Women in the present study were older than men, a factor associated with non-attendance. Further, many women lived alone or were widowed. The co-existence of these factors suggests reduced social support, which has previously been identified as a barrier to programme attendance [43]. Likewise, women were less likely to drive their own car, another recognized deterrent to participation [34]. Importantly in the present study, being a non-driver was also associated with non-attendance among men.
Nonetheless, we found higher rates of attendance among women than reported previously. While 44.9% of women in the present study attended, past studies have reported rates as low as 15% [11], 32% [18] and 34% [17]. It is likely that the absence of requirement for formal physician referral might have contributed to the more favourable participation rate by women in our study. Moreover, patients of any age were eligible to attend.
The poorer attendance amongst older patients, both men and women, is consistent with most previous findings [14, 15, 17, 18, 24–26], despite evidence that older patients can improve significantly by attending CR [44]. The failure of many older patients to attend in the present study might be explained, in part, by transport difficulties, since many were non-drivers. Slower recovery and a higher incidence of complications among older patients following acute cardiac illness might also have contributed [45, 46]. Older patients, especially older women, are likely to have greater disability, not only from cardiovascular disease, but also from co-morbidities such as arthritis [26, 45]. Even in the absence of any referral bias in this study, some physicians might consider CR and secondary prevention to be less relevant for such patients [47], hence giving less encouragement to attend.
Being unemployed was associated with both non-attendance and drop-out amongst men, consistent with some previous findings [4, 14, 15]. Unemployed patients were less likely to have access to a car (P < 0.001) and, amongst men, were more likely to rely on public transport (P < 0.001) and to live alone (P = 0.002), suggesting that transport difficulties might have partly accounted for their poor attendance. Practical assistance with transport is required to facilitate access to programmes by patients with transport difficulties, including older patients, women and those not in the workforce.
The lower participation rate among men who had undergone PCI or suffered an AMI is also consistent with past reports [13, 20, 21]. While higher rates of referral of CABGS patients might account for this pattern in other studies [18, 30], this bias was minimized in the present study. Nonetheless, surgical patients may perceive that they are more in need of cardiac rehabilitation than either AMI or PCI patients. Indeed, while CR programmes were originally developed for AMI patients, eligibility has since been extended to other patient groups. In this time we have seen higher uptake amongst CABGS patients and lower uptake amongst PCI patients relative to AMI patients, both in Australia and elsewhere [13, 24]. The attendance rates of 66, 51 and 25% respectively for CABGS, AMI and PCI patients in our study directly reflect this pattern. Indeed, the 51% attendance amongst AMI patients represents good attendance when considered in the light of many previous reports. Thus, it is not that AMI patients showed ‘poor' attendance but, rather, that CABGS patients showed relatively high attendance.
Additional factors also operate further to inhibit CR programme attendance by PCI patients. First, the very short hospital stay of PCI patients reduces opportunities for arranging referral to an outpatient CR programme. Second, both patients and health professionals commonly perceive that standard CR programmes are unnecessary for this group because these patients have not experienced sufficient physical or psychological trauma [12, 20, 48]. On the contrary though, secondary prevention interventions are especially important for PCI patients who are at high risk of future cardiac problems [20, 49]. Programmes should be devised or modified to incorporate specific modules vigorously addressing risk factor modification for PCI patients [1, 50].
In our study, we found that the presence of known risk factors prior to the cardiac event encourages subsequent participation in CR, especially amongst women with a history of high cholesterol and amongst men with a family history of heart disease. Presumably their perceptions of susceptibility to future cardiac illness motivated them to attend. Indeed, it has been suggested that high cholesterol is perceived as being amenable to dietary change and is therefore a strong motivator for programme attendance [14]. It is also possible that health professionals actively encourage CR participation for those with high cholesterol. In contrast, attendance was not associated with a history of hypertension, as reported previously [14], suggesting that the prognostic significance of this risk factor is less well recognized by patients. This finding suggests the need for further patient education regarding the importance of controlling high blood pressure.
While also a risk factor, physical inactivity appears to inhibit attendance amongst women. Physically inactive women were less likely to attend and, once attending, were more likely to drop out than those who were physically active before hospital admission. This finding might reflect a general reluctance to exercise [17, 26] or some dissatisfaction with the exercise programme [51]. Interestingly, it contrasts with one recently published Australian study where physically inactive men were more likely to attend CR programmes [19], highlighting the importance of physical inactivity as an inhibiting factor for women only.
Smoking also appears to reduce participation, as previously reported [22, 23]. Amongst attending men, those who smoked at the time of their hospital admission were more likely to discontinue the programme. The emphasis in CR programmes on quitting smoking might create cognitive dissonance amongst those patients who are unable or unwilling to quit, thereby discouraging continued participation. Indeed, smokers are more likely to remain in programmes if the difficulties of quitting smoking are acknowledged and the subject of smoking cessation handled sensitively [52].
Having a history of diabetes was associated with non-attendance amongst women and drop-out amongst attending men. It is possible that patients with diabetes already had prescribed regimens for lifestyle change, especially dietary control and weight loss, and therefore did not recognize a need for an additional programme of exercise and education. For women in the present study, having diabetes was associated with being physically inactive before admission to hospital (P = 0.017), which might also partially account for their non-attendance. Similarly, while obesity was itself not a predictor of non-attendance or drop-out, it was associated with other predictors, including smoking in men and physical inactivity in women.
Some previously reported associations with non-participation in programmes were not found in the present study. While patients of lower education and occupational levels often fail to attend programmes [11], reflecting lower socio-economic status and likely financial constraints, our study found no relationship between these factors and programme participation. The fact that our programmes were offered free of charge might account for this finding. The considerable ethnic diversity in the region of the two recruiting hospitals might explain why language was not a barrier. Over one-third of the men and over one-quarter of the women spoke languages other than English at home. This diversity possibly increased the likelihood of shared language at the CR programmes provided by these two hospitals.
Our study has several strengths. First, by studying a large sample and by analysing patterns of attendance for men and women separately, we were able to produce a clearer picture of attendance patterns among women than has been found in past studies of smaller samples. We were also able to study both non-attendance and drop-out in this prospective study by using separate dichotomous variables. Importantly, all variables included in our study were identified a priori to be potentially associated with attendance. We were therefore able to identify the key socio-demographic and clinical predictors of non-attendance and drop-out from amongst all those which have been shown to influence programme participation.
Secondly, we had a relatively small proportion of excluded or withdrawn patients. It was interesting to find that the characteristics of patients who were lost to follow-up closely resembled those of non-attending patients in that they were more likely to be living alone, non-drivers, AMI patients and to have diabetes. Although outside the scope of the present investigation, this group itself deserves closer examination.
However, some limitations of the present study should be noted. First, in many cases, baseline characteristics and attendance status were based on patient self-report with no external validation. Self-reporting of some health behaviours and risk factors is considered to be unreliable [53, 54]. Importantly, patients' CR programme attendance status was based on CR programme attendance records, as well as patient self-reports, thereby optimizing reporting accuracy for the dependent variable. Second, even with the relatively large study sample, prediction of drop-out by women was limited by small numbers. Third, the death rate of approximately 10% in our study is higher than that usually reported in the literature (5–7%). However, most of the in-hospital deaths were following AMI (80 deaths from 526 unselected admissions for AMI, representing a 15.2% mortality rate) which is similar to that reported previously for the same population [55]. Finally, our study was confined to investigation of socio-demographic and clinical factors. Other factors such as patient beliefs and perceptions [14], patient psychological state [16] and the strength of the physician's recommendation [25, 26, 30, 37] can also influence patients' willingness to attend CR programmes. The quality of the programme, the skills of those delivering the programme [51, 56] and patient distance from the programme [11, 32] can also impact on attendance and completion.
There is sound scientific evidence to support the benefits of attending CR programmes [1–5]. The present findings highlight the need for targeted encouragement and support for those patients at higher risk of non-attendance, particularly women who are older or inactive, and men who are older, PCI patients, smokers, unemployed or non-drivers. Health professionals working in cardiac rehabilitation can use these findings to encourage attendance amongst these high-risk groups. In particular, practical assistance with transport might facilitate attendance amongst those who are older, non-drivers or unemployed. In addition, education regarding the relevance of CR programmes for PCI patients and those with hypertension might be warranted. In light of the relatively high overall attendance rate reported here, it is possible that automatic referral to programmes for all patients would optimize attendance. The present findings also suggest that physicians and patients should be made more aware of the benefits and content of programmes [35], especially that exercise sessions are commonly based on low to moderate intensity exercise that can be tailored to suit the needs and capacity of individual patients, irrespective of age.
Footnotes
Acknowledgements
The project was supported by a 3-year grant from the Australian Commonwealth Department of Health and Ageing. The authors would like to acknowledge Dr Peter Elliott who provided statistical advice.