
Abstract
Background
The average life expectancy of a person aged 75 in Finland is approximately 10 years. A substantial threat to the quality of life during these years is stroke, which is common among the elderly, may hamper independent living and places a substantial burden on health care resources. The aim of the present study was to analyse the trends in incidence, mortality and prognosis of acute stroke events in persons aged ≥ 75 years in Finland.
Design
A population-based stroke register study.
Methods
The FINSTROKE register recorded all stroke events in persons aged ≥ 75 years (n = 5493) among inhabitants of the town of Turku from 1982 to 1992 and again from 1996 to 1998, and in the Kuopio area from 1990 to 1997.
Results
At the end of the study period, the age group ≥ 75 years constituted 3.8% of the population of study areas among men and 8.7% among women. This population segment contributed 35% of strokes among men and 66% among women. Of all strokes in this age group, 73% occurred among women. Data suggested that the mortality and incidence of acute stroke events were declining, but the 28-day case fatality did not change. At day 28 after the onset of stroke, only 26% of men and 19% of women had recovered well enough to be capable of independent living.
Conclusions
Stroke mortality among the elderly is declining in Finland, which is mainly due to the decline in the incidence of stroke events.
Introduction
Survival to old age has increased dramatically in all western countries, including Finland. The increase in the ageing population is expected to increase the burden of vascular diseases; ischaemic heart disease, stroke and peripheral vascular disease. Stroke is one of the most common causes of death. In many ways, however, the greatest burden of stroke is the disability it impacts on stroke survivors. About half of the stroke survivors suffer permanent disability; for those whose handicaps are reversible, the process of recovery can be long.
Old age is the strongest but nonmodifiable risk factor for stroke. In the year 2000, the average life-expectancy of a person aged 75 in Finland was 9.1 years among men and 11.5 years among women. One of the main threats to quality of life in the elderly during these years is stroke. Relatively little is, however, known about the epidemiology of stroke events among the elderly. For example, the large stroke register study of the WHO MONICA Project considered only stroke events among persons aged younger than 65 years thus excluding the overwhelming majority of stroke events [1]. In Finland, part of the FINMONICA stroke registration took place without the upper age limit and after the end of the MONICA Project [2], the FINSTROKE register continued to include also elderly persons. The aim of the present study was to analyse the trends in incidence, mortality and prognosis of stroke in persons aged 75 years or over in Finland during 1983 to 1998.
Material and methods
The Turku stroke register was a population based register set up in 1982 as part of the larger FINMONICA stroke register, in turn participating in the WHO MONICA project, an international collaboration aiming at multinational monitoring of trends and determinants in cardiovascular disease [3]. After the end of the FINMONICA Project, the stroke registration was continued under the name FINSTROKE. While the FINMONICA register limited stroke registration to the age group 25–74 years, we registered in Turku, south-western Finland, all suspected strokes occurring in subjects older than 74 years from 1982 to 1992 and again from 1996 to 1998. In Kuopio area in eastern Finland this older age group was included in the registration from 1990 to 1997. With this exception, we strictly followed the same data collection and quality control procedures as used in the stroke registers of the WHO MONICA Project. A detailed description of the FINMONICA stroke register, its case finding and registration procedures, has been published [4]. Here we give only a brief overview of the main definitions used for the present analyses.
The diagnosis of stroke was based, as specified in the WHO MONICA protocol [3] on clinical signs lasting more than 24 h, except in cases of sudden death or if the development of symptoms was interrupted by surgical intervention. All acute suspected strokes have been registered and classified as ‘definite stroke', ‘not stroke’ or ‘insufficient data', the latter restricted, with few exceptions, to fatal events occurring before arrival at hospital and with no autopsy. There were altogether 96 such cases (1.7%). All hospital admission and discharge diagnoses, as well as cerebrovascular deaths, were routinely checked as source data, and all suspected stroke cases were included in stroke classification. The stroke register data were annually cross-checked with National Death Register for completeness [5].
Acute stroke events with no previous history of a clinically symptomatic stroke were coded as first events. All subsequent attacks occurring after 28 days from the onset were registered as recurrent strokes; within 28 days they were considered to belong to the same event. Twenty-eight days from the onset was also the cut-off point used to define fatal stroke. Thus, if the subject was alive after 28 days from the onset of symptoms, the event was considered nonfatal.
The functional ability of the subject at day 28 after the onset of stroke was classified: (1) the patient does not need help in his/her activities of daily living, (2) needs some help, (3) severe disability means that the patient is bedridden and fully dependent of help from others.
In this analysis unspecified stroke and cases with insufficient data were combined with the ischaemic stroke group. In the age group 25 to 64 there were 1.4%, in the age group 65 to 74 years 5% and in the age group ≥ 75 years 10% of events with unspecified stroke or insufficient data. The proportions did not vary through the study years, among nonfatal vs. fatal, or first vs. recurrent events.
The Finnish Population Register provided us with population data for rate calculations. The Segi's European standard population was used for direct age standardization [6]. The 28-day case fatality was age-standardized using weights derived from the combined age distribution of MI and stroke patients in the WHO MONICA Project. The 95% confidence intervals (CI) were calculated assuming Poisson distribution for the annual number of events. A log-linear model was used to estimate incidence and mortality trends, thus obtaining the confidence interval for the trends from the standard error of the regression coefficient. With this model, the average annual change in the trend is obtained multiplying the regression coefficient by 100.
Results
The number of men aged > 75 years living in the register area of Turku was 2393 in 1983. By the year 1997 this number had increased by 40%, to 3416. The corresponding numbers for women were much larger and also increasing: 6352 in 1983 and 8933 in 1997. In Kuopio register area there were 1885 men aged > 75 years in 1993 and 2172 in 1997. The numbers of women aged > 75 years in Kuopio area were 4907 in 1993 and 5264 in 1997. At the end of the study period, the age group ≥ 75 years constituted 3.8% of the population among men and 8.7% among women. This population segment contributed 35% of all strokes among men and 66% among women. Of all strokes in this age group, 72.4% occurred among women.
According to the official mortality statistics, age-standardized mortality from stroke among persons aged ≥ 75 years declined in Finland during 1985 to 2000 on average by 2.6% (95% CI −3.3; −2.0%) per year among men and by 2.9% (−3.3; −2.4%) per year among women (Fig. 1). In the FINSTROKE areas, altogether 484 men and 1268 women aged ≥ 75 years died from stroke during the study period. The average annual change in age-standardized mortality from stroke among men was −4.0% (−6.3, −1.6%) in Turku and −4.0% (−11.4, 3.4%) in Kuopio (Table 1). Among women, the corresponding changes in age-standardized mortality were −3.6% (−5.0, −2.1%) in Turku and −0.1% (−4.7, 4.6%) in Kuopio.
The average annual change in the incidence of first stroke events among men was −3.0% (−4.6, −1.4%) in Turku and −0.6% (−5.2, 4.0%) in Kuopio (Table 1). Among women, the annual change in the incidence of stroke was −2.0% (−3.0, −1.1.%) in Turku and −2.3% (−5.4, 0.7%) in Kuopio. The 28-day case fatality did not change significantly during the study period in either area or in either sex, although there was a small decreasing tendency (Table 1).
At day 28 after the onset of stroke 33% of men had died, 9% were bed-ridden, 33% needed some help and 26% did not need help in their activities of daily living. Among women 38% had died, 9% were bed-ridden, 35% needed some help and only 19% did not need help in their activities. Figure 2 shows stratified analysis by the age group 75–84 and ≥ 85 years. The 28-day case fatality was higher in the age group ≥ 85 years, especially in women. Only a small number of women aged ≥ 85 years did not need help in their activities of daily living at day 28 after the onset of stroke. On the other hand, in the age group 75–84 years a substantial proportion of both men and women had recovered well enough to be capable of independent living.
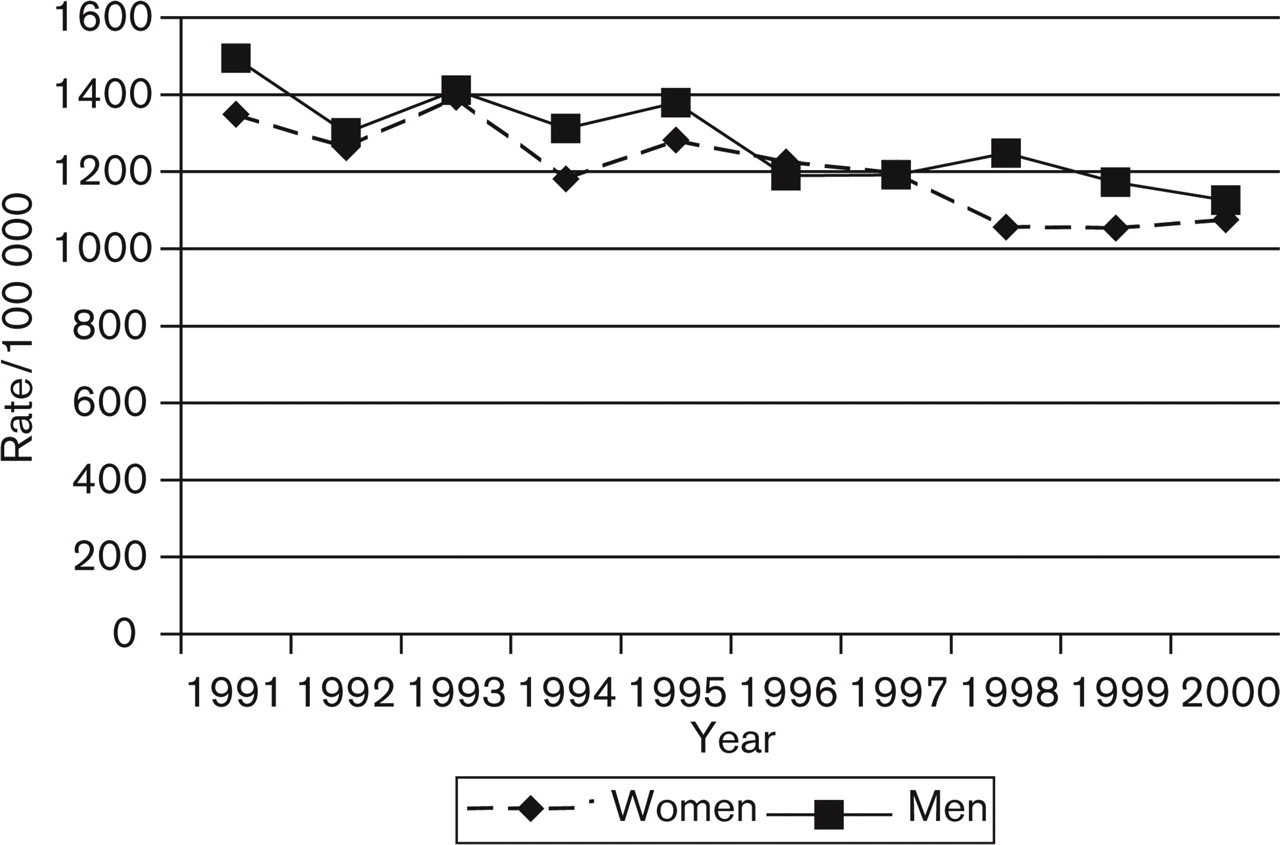
Trends in stroke mortality among men and women aged ≥ 75 years in Finland during 1991–2000 according to the official mortality statistics (ICD 10 I 60 - I 69). The annual average change is −2.6% (95% confidence interval −3.3; −2.0%) among men and −2.9% (−3.3; −2.4%) among women.
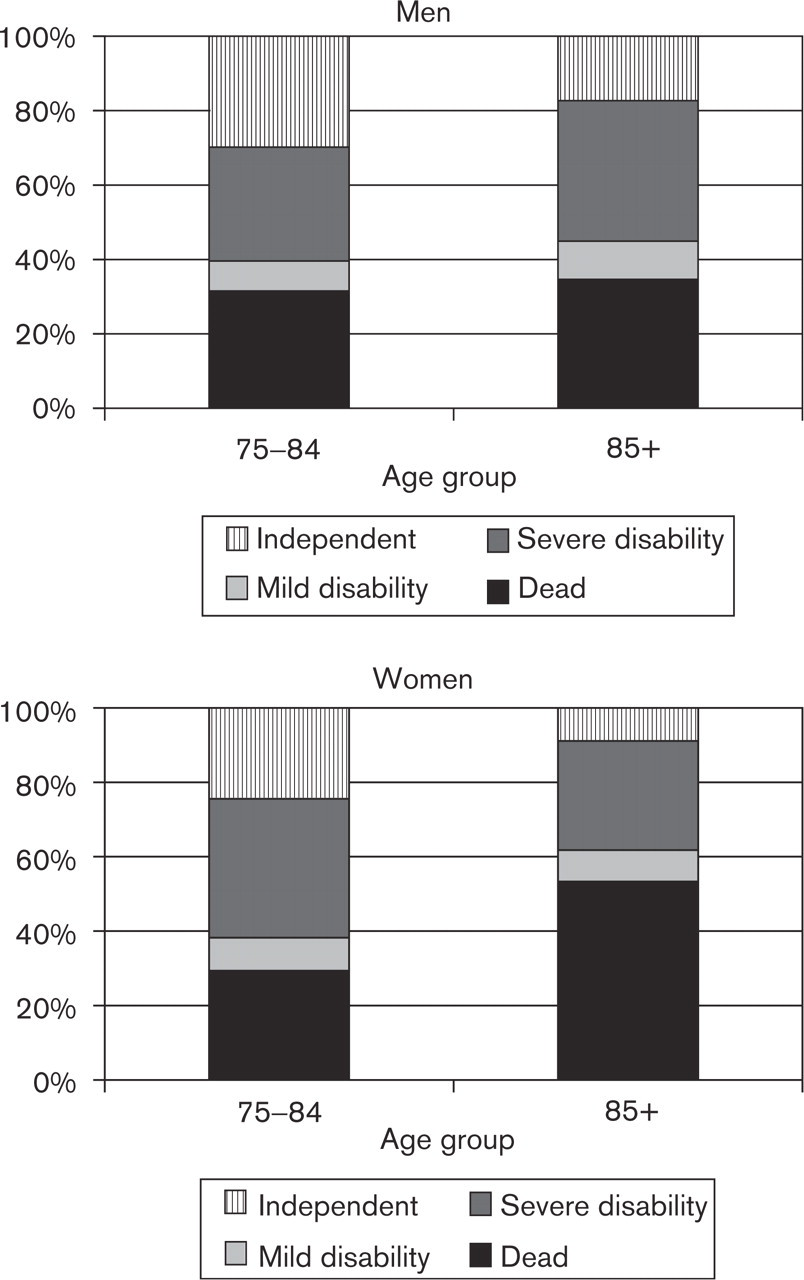
Status of the patients aged 75–84 years and 85+ years at day 28 after the onset of stroke event that occurred in 1996–1997. Mild disability means that the patient needs some help in his/her activities of daily living, severe disability means that the patient is bedridden and fully dependent of help from others.
Trends 1 (%/year) in age-standardized stroke mortality, incidence of first stroke events and 28-day case fatality among men and women aged 75–99 years in the FINSTROKE areas during 1982–1998

1Average annual change.
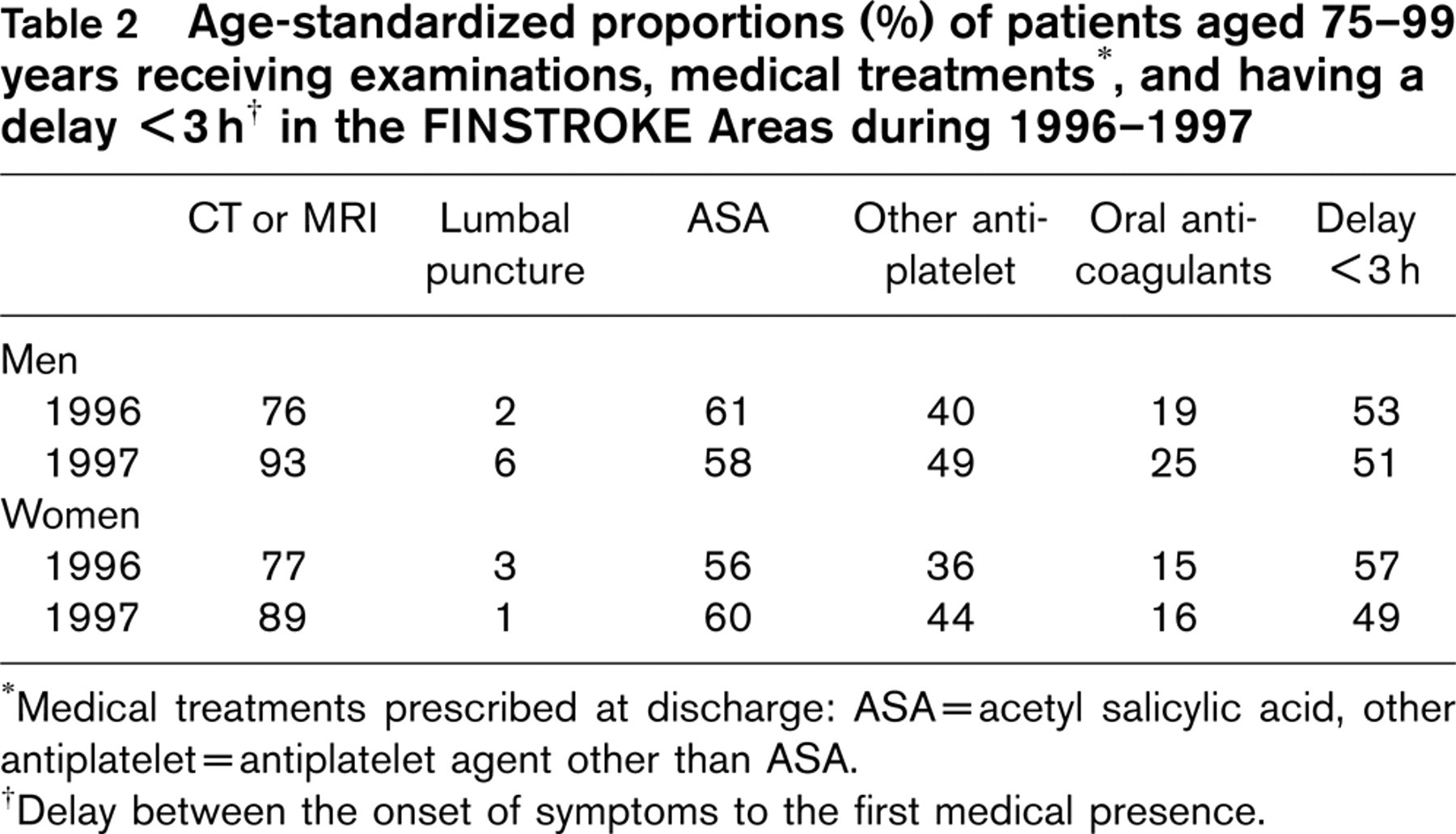
∗Medical treatments prescribed at discharge: ASA = acetyl salicylic acid, other antiplatelet = antiplatelet agent other than ASA.
†Delay between the onset of symptoms to the first medical presence.
The age-standardized proportions of selected examinations, medical treatments and delay from the onset of symptoms to the first medical presence are shown in Table 2. In 1997, approximately 90% of stroke patients aged ≥ 75 years were examined with computerized tomography or magnetic resonance imaging. Lumbar puncture was rare. About 60% of stroke patients received acetyl salicylic acid (ASA) at discharge from hospital and 40% other antiplatelet treatment. Oral anticoagulants were prescribed to 15–25% of patients. Half of these elderly stroke patients had a delay < 3 h between the onset of symptoms and the first medical presence.
Discussion
This is the first article reporting data from the FINSTROKE areas in the population aged 75 years or more. Ten-year trends in stroke events in the FINMONICA study covering the age group 25 to 75 years have been published [6, 8] and 11-year trends of stroke in Turku area in the age group 25 to 74 years as well as in the population older than 74 years [2]. In our study, the period of data collection according to a standardized protocol is 15 years. The incidence of stroke declined annually between 0.6% and 3% in this age group over 74 years. The observed average decline in mortality from stroke was between 0.6% and 4.0% depending on gender and study area. The absolute number of registered strokes remained almost stable through the study years due to the steep increase in the size of the elderly population. Thus, in spite of the observed declining trends, the need for stroke care has not diminished, but has obtained geriatric features.
A strength of our study is the long period of data collection applying a standardized protocol. The strict criteria established in the WHO MONICA project [3] and followed also in the FINSTROKE Project ensure that secular trends in the incidence of stroke are not affected by changes in diagnostic practices. Completeness of case finding could be ascertained using computerized national Causes-of-Death register.
The only other stroke register which participated in the WHO MONICA project which has published data on stroke events among persons aged ≥ 75 years is Glostrup, Denmark [9]. The incidence of stroke in our study was higher than that observed in Glostrup. The average annual decrease in the age-standardized stroke rates in the age group over 74 years in Glostrup was 2.4% among men and 3.1% among women [9]. The occurrence of stroke increased exponentially with age until the age group of 75–84 years, but among the oldest age group the increase started to level off slightly [9]. Similar patterns were found in Perth, Australia [10], Auckland, New Zealand [11] and Rochester, USA [12].
The age-standardized stroke mortality decreased significantly in our population. This was mainly due to the decrease in the incidence of stroke, because the 28-day case fatality of stroke events did not decrease significantly. However, in Kuopio area the decline in incidence among men was nonsignificant and the 28-day case fatality declined quite substantially, although nonsignificantly.
At day 28 after the onset of symptoms 33% of men and 38% of women had died. In Glostrup, the case fatality increased significantly with increasing age and the age-adjusted case fatality was higher among women (32%) than among men (28%) [9]. In studies examining the direct cause of death within 30 days after the first stroke, death was due to cerebrovascular disease in 91% of patients in the Oxfordshire Community Stroke project and in 85% in the Perth Community Stroke Project [13–15. Loor et al. [15] found that only one of 58 patients did not die of the index stroke. The highest risk for death is in the acute phase of a stroke and then it gradually decreases [16].
More than one year after the first stroke the excess mortality appears to level off so that the risk for death is approximately twice that of the general population. The most frequent cause of death during the post-stroke period in patients who survived acute stroke is cardiovascular disease. Cerebrovascular diseases accounted for 32–43% and ischaemic heart disease for 23–34% of deaths in some post-stroke surveillance studies [13–16.
The incidence rate of stroke declined in our study. The decline in the incidence of stroke has been reported in other studies, Glostrup, Denmark [9], Shanghai, China [17], Perth, Australia [18] and Minnesota, USA [19]. Data from the Northern Sweden MONICA Stroke Register [20] showed a decline in stroke rates among men younger than 65 years but an increasing stroke incidence among the older men.
Cardioembolism is the most common aetiology of stroke [21, 22] and cardioembolic strokes particularly dominate in the oldest group [22]. This is most likely caused by the increase of atrial fibrillation parallel to ageing [23]. In the last years of our study about 20% of stroke patients received oral anticoagulants at discharge from hospital, about 60% had ASA and 40% other antiplatelet treatment. About 50% of patients had the delay from the onset of symptoms to medical presence less than 3h and the use of CT and MRI were high, about 80%. The short delay and specific diagnosis achieved through neuroimaging give possibilities to consider thrombolytic treatment also for some of the elderly patients. An important risk for a stroke survivor is recurrent cerebrovascular disease attack. This is a strong argument for increasing efforts in the field of secondary prevention. Post-stroke disability was very common in stroke patients in our material, especially in the age group over 85 years. It emphasizes the need for improved rehabilitation to minimize post-stroke disability.
In conclusion, the incidence and mortality of stroke have been declining in Finland in the age group ≥ 75 years. Over half of all stroke events originate from this age group and the majority of patients are females. Regarding the absolute number of stroke events, however, the increase in the elderly people in the background population counterbalanced the effect of improved prevention and the reduction in incidence. Thus, the number of stroke events was not significantly reduced.
Footnotes
Acknowledgements
This study was supported by grants from the Foundation of King Gustaf V and Queen Victoria and from Finnish Foundation for Cardiovascular Research.