
Abstract
Aerobic endurance training has been an integral component of the international recommendations for cardiac rehabilitation for more than 30 years. Notwithstanding, only in recent years have recommendations for a dynamic resistance-training program been cautiously put forward. The perceived increased risk of cardiovascular complications related to blood pressure elevations are the primary concern with resistance training in cardiac patients; recent studies however have demonstrated that this need not be a contraindication in all cardiac patients. While blood pressure certainly may rise excessively during resistance training, the actual rise depends on a variety of controllable factors including magnitude of the isometric component, the load intensity, the amount of muscle mass involved as well as the number of repetitions and/or the load duration. Intra-arterial blood pressure measurements in cardiac patients have demonstrated that that during low-intensity resistance training [40–60% maximum voluntary contraction (MVC)] with 15–20 repetitions, only modest elevations in blood pressure are revealed, similar to those seen during moderate endurance training. When properly implemented by an experienced exercise therapist, in specific patient groups an individually tailored, medically supervised dynamic resistance training program carries no inherent higher risk for the patient than aerobic endurance training. As an adjunct to endurance training, in selected patients, resistance training can increase muscle strength and endurance, as well as positively influence cardiovascular risk factors, metabolism, cardiovascular function, psychosocial well-being and quality of life. According to present data, resistance training is however not recommended for all patient groups. The appropriate training method and correct performance are highly dependent on each patient's clinical status, cardiac stress tolerance and possible comorbidities. Most studies have used middle-aged men of average normal aerobic performance capacity and with good left-ventricular (LV) function. Data are lacking for high-risk groups, women and older patients. With the current knowledge it is reasonable to include resistance training without any restraints as part of cardiac rehabilitation programs for coronary artery disease (CAD) patients with good cardiac performance capacity (i.e., revascularised and with good myocardial function). As patients with myocardial ischaemia and/or poor left ventricular function may develop wall motion disturbances and/or severe ventricular arrhythmias during resistance exercise, the following criteria are suggested for resistance training: moderate-to-good LV function, good cardiac performance capacity [> 5–6 metabolic equivalents of oxygen consumption (METS) = 1.4 watt/kg body weight], no symptoms of angina pectoris or ST segment depression under continued maintenance of the medical therapy. Based on available data, this article presents recommendations for risk stratification in cardiac rehabilitation programs with respect to the implementation of dynamic resistance training. Additional recommendations for specific patient groups and detailed directions showing how to structure and implement such therapy programs are presented as well.
Keywords
Introduction
Although aerobic endurance training has been an integral part of international recommendations for the prevention and rehabilitation of cardiovascular diseases for the last 30 years, the medical community has been more hesitant to endorse resistance training for these patients [1–4]. This hesitation is based mainly on the notion that blood pressure elevations during resistance training increase the risk of cardiovascular complications, especially in elderly patients and those with previous impairments [1, 5]. Accumulated data from numerous studies over the past two decades have shown that these concerns need not contraindicate resistance training in all cases. This is especially true for resistance training of coronary artery disease (CAD) patients with good aerobic performance capacity and good left ventricular function [3, 6]. Complementary resistance training in this patient group, when appropriately implemented and supervised does not have a higher inherent risk than aerobic endurance training alone. As an adjunct to endurance training it can help positively influence psychosocial well-being and the patient's quality of life [3, 7, 8]. Preliminary recommendations have been published in the last few years for CAD patients with good aerobic performance capacity [3, 7, 8].
Based on its numerous health-promoting factors, moderate resistance training is recommended for persons of all ages as an important component of a comprehensive fitness program [9, 10]. Resistance exercise can lead to an increase in muscle strength and endurance as well as increased muscle mass and/or improve coordination and metabolism.
Muscle mass and muscle strength decrease by about 30% between the third and sixth decades of life [11]. With aging, the total number of muscle fibers decreases, especially the fast-twitch muscle fibres, which are recruited in force development. It is not yet clear to what extent this is due to the biological aging process or simply from a distinct lack of exercise. In order to maintain an essential strength elderly individuals especially need proper load stimulus. Through adapted resistance exercises it is possible to provoke an increase in muscle mass even in the elderly [5, 12–16]. This training-induced hypertrophy involves mostly fast-twitch muscle fibers [13, 15, 16].
Further decreases of muscle mass and strength in cardiac patients can be attributed to long-term bed-confinement, physical inactivity, and/or glucocorticoid therapy. In some cases (especially in elderly patients) this muscle wasting causes a more significant impairment than the cardiovascular disease itself with regard to functionality. Appropriate resistance training can oppose and reverse this loss of muscle mass, as well as improve cardiac stress tolerance.
In certain patient groups increasing muscle strength and function can lead to significant improvements in quality of life. The patients' improved functionality in carrying out everyday activities supports their independence, positively influences their self-confidence and psycho-social well-being, and can prevent or reduce the need for future home-care. In addition, the improvements in physical and functional performance capacity are an important prerequisite for rapid and more efficient social and occupational re-integration.
Resistance exercise positively influences proprioceptive abilities leading to a gradual improvement in co-ordination and equilibrium. This improved motor ability reduces the danger of falls (especially in the elderly) with all the possible setbacks that they can entail [1].
Regular load stimuli on the structures involved in joint function constitute an important prerequisite for maintaining a healthy musculo-skeletal system and plays a significant role in delaying the onset of a multitude of arthrotic problems which become relevant in middle-aged and elderly patients.
Appropriate resistance training represents an important tool in the fight against degenerative joint diseases. It strengthens the surrounding structures that support the joint and combats degenerative processes within it. A well-developed musculature prevents arthrosis and reduces the symptoms that arise from pre-existing degenerative changes [15, 17].
Resistance training positively influences bone density in both women and men. Regular resistance training can reduce and prevent, respectively, decreases in bone mass that may accompany aging and/or the postmenopausal period [18–21]. It is important in the prevention as well as in the therapy of osteoporosis [22]. Mechanical stress induces bone formation. Thus, all kinds of physical activity that cause mechanical stress to the bones are effective. This applies above all to resistance exercise but also to endurance training, such as walking or hiking, where the body mass is itself moved. Activities like swimming and biking, which do not cause mechanical stress to the skeleton, are not effective in this respect [18, 23, 24]. In order to counteract losses in bone mass, it is necessary to exercise regularly [25]. The risk of fractures is higher with lower muscle mass and decreased co-ordinative abilities [26, 27]. Both factors can be improved through a specific resistance exercise program.
Provoked by long-term glucocorticoid therapy, heart transplant recipients develop skeletal muscle atrophy (steroid myopathy) [28] as well as skeletal demineralization, resulting in a decrease in bone mass [29] and an increased fracture risk [30]. Adequate resistance exercise can prevent these developments and/or level out the losses [31, 32]. Wasting of muscle mass and muscle strength as a result of long-standing congestive heart failure and physical inactivity are considered to be the primary reasons for reduced performance capacity of heart transplant recipients prior to operation [33].
Although maximal oxygen uptake cannot be significantly elevated by resistance exercise, studies revealed that intensive resistance training could improve submaximal endurance capacity. Ades et al. [12] reported an increase in exhaustive submaximal walking distance by 38% in elderly participants after they completed a 12-week resistance exercise program. These findings attain a greater significance the greater the actual reduction in the patient's physical performance is.
In fact, resistance exercise can result in extreme increases in blood pressure, but this is not the case for all kinds of load. The actual blood pressure response to resistance exercise depends on the magnitude of the isometric component, the load intensity [in percentage of maximum voluntary contraction (MVC)] [34, 35], and the amount of muscle mass involved [36]. The blood pressure response is also dependent on the number of repetitions and the load duration. The highest blood pressure values are reached when multiple sets at 70–95% of MVC are performed up to exhaustion. The pressure values are then higher than those measured at lower intensities or during one repetition maximum (1 RM) [37–39]. Apparently, both factors involved in the rise in blood pressure, load intensity and duration, take full effect at 75–90% of MVC. At an MVC below 70% the intensity is not high enough, and beyond 95% the duration is not long enough to produce maximum blood pressure reactions [40]. If the Valsalva manoeuvre is carried out during resistance exercise the rise in blood pressure is more pronounced. [38]. The peak blood pressure may lead to arterial ruptures whereas the diminution in cardiac output results in a lowered perfusion in the coronary arteries. Complications may occur such as rhythm disturbances and myocardial infarction. Bradycardia, occurring post-Valsalva manoeuvre, may provoke severe arrhythmias, or even ventricular fibrillation. A rapid fall in blood pressure after straining at maximal workload sometimes leads to syncope, even in healthy persons [41].
Changes in blood pressure and heart rate in response to muscle activity are, at least in part, evoked by sensory nerve fibers, which pick up information from the working muscles [42, 43]. Their receptors primarily react to metabolic changes rather than mechanical stimuli [44–47].
Accordingly, the perfusion of the peripheral work musculature [48] and the magnitude of contraction [35], along with the amount of involved muscle mass [36] influence the blood pressure and heart rate reactions. When perfusion is limited, the load duration also becomes an important variable, as the blood pressure does not attain steady-state conditions. In the case of continuous skeletal muscle contraction, the arteries are compressed and perfusion is diminished; this occurs even at contraction levels as low as 10% MVC [49]. It is thereby less important if the type of contraction is dynamic or isometric. It is more decisive for muscle perfusion if periods of relaxation occur during the workload and—in case they do—the temporal relationship of contraction to relaxation phases.
Intra-arterial blood pressure measurements recorded during resistance training in cardiac patients demonstrated that training carried out at low intensities (40– 60% of MVC) and with fewer repetitions (10–15 repetitions) evokes only a moderate rise in blood pressure compared to the increases seen during moderate endurance training [50]. Results of a meta-analysis show, that when progressive resistance training is performed regularly, a reduction in resting systolic and diastolic blood pressure values can be attained [51]. However, for therapeutic assessment of these findings further studies need to be conducted. Improved muscle strength leads to a reduction in heart rate and blood pressure response to a given load as the exertion level required can be achieved at a lower percentage of MVC [52]. In this way, the danger of cardiac overload caused by muscular activity in sports, daily routines and occupational activities is reduced [3]. A lower blood pressure–heart rate product and higher diastolic blood pressures probably lead to better oxygenation of the myocardium when compared to endurance training. The results of numerous studies report fewer cardiac symptoms, wall motion disturbances, signs of ischaemia (angina pectoris, ST changes), or significant ventricular arrhythmias being observed during resistance training than during endurance training [50, 53–57].
Although the metabolic response to resistance training is only moderate (comparable to slow walking), the rate of energy turnover increases slightly. This increased rate persists for several hours after the training has been discontinued [58]. Increased muscle mass also increases basal energy turnover. Thus, resistance training can induce a stabilization or reduction in body weight [59]. It also leads to an increase in insulin sensitivity, independent of weight changes and aerobic endurance capacity [60–62]. This also applies to patients with a type 2 diabetes (non-insulin-dependent diabetes mellitus [NIDDM]) [63–65]. Resistance exercise therefore plays an important role in the control of this metabolic syndrome in cardiac rehabilitation programs.
Recent studies revealed that resistance training also has a positive influence in patients with peripheral vasoocclusive disease. McGuigan et al. [66] demonstrated that, in this subset of patients, muscular strength improved, significant changes in muscular composition occurred, capillary density increased and the pain-free walking distance increased by 158% following a tailored 24-week resistance exercise program.
When correctly carried out, resistance training has a very low inherent risk of injury. Pollock et al. [67] found an average of 2.2 minor muscle-joint-ligament injuries per 1000 training hours.
In summary, and in accordance with the recommendations, an adapted resistance-training program, individually dosed and medically supervised and controlled by experienced exercise therapists, can improve not only muscular strength, endurance, cardiovascular function, metabolism, psycho-social well being and quality of life, but also minimize cardiovascular risk factors [3].
Despite these well-documented positive effects, resistance training is not universally recommended to all patient populations. The suitable form of training and its correct execution depends largely on the clinical status of the patient, cardiac stress tolerance as well as the presence of other comorbidities. Most studies done thus far have included small groups of middle-aged men (< 70 years) in good general health including good cardiac performance capability, normal or near normal aerobic capacity and good left ventricular (LV) function. Specific data focusing on risk groups such as older patients or women are still missing. Based on current data, the incorporation of resistance training into cardiac rehabilitation programs can only be recommended without restraint to CAD patients with a good cardiac performance capacity (good myocardial function, revascularised). Due to the fact that patients with myocardial ischaemia and/or poor LV function may develop wall motion disturbances and/or severe ventricular rhythm disturbances in the course of resistance exercise, the following criteria are recommended for the selection of suitable candidates for resistance training: moderate-to-good LV function, good cardiac performance capacity [> 5–6 metabolic equivalents of oxygen consumption (METS) = 1.4 watt/kg body weight], no symptoms of angina pectoris or ST segment depression under continued medication [3, 7].
Before beginning with a resistance-training program, these patients should participate in a typical 2–4 week aerobic training program. This also applies to patients who have had a percutaneous intervention (PTCA) [3]. Due to a lack of data an accurate risk assessment of resistance training in patients with a moderate-to-high cardiac risk, women and elderly patients, is not possible. A few studies with small patient cohorts have demonstrated positive results for resistance exercise in such patients without a higher risk [68–72]. Considering the lack of long-term studies for these patient groups more research, dealing especially with the hemodynamic consequences of resistance training, is necessary before general recommendations can be made. The final solution to this compelling question is of the utmost importance because improvements in muscular strength and endurance – precisely for these groups of patients—would be very advantageous, assuming of course that these goals could be achieved without higher cardiac risks.
Recommendations for risk assessment in resistance training
In accordance with the recommendations of the German Society for Prevention and Rehabilitation [55], a typical patient evaluation involves: medical history, clinical examination, a rest-electrocardiogram (ECG), a symptom-limited stress-ECG and echocardiography (with Doppler/colour-Doppler). Other supplementary options are: Holter monitoring, 24-h blood pressure monitoring, stress echocardiography, CXR and, in a few cases, evaluation of the filling pressures with a Swan–Ganz catheter under stress conditions. All the above-mentioned diagnostic methods are readily available in cardiac rehabilitation centres. If recent (< 4 weeks old) results from other examinations are available, they may also be used. If the clinical status of a patient is unclear and previous examinations/tests are lacking, invasive diagnostic measures should be undertaken in order to clarify the situation.
A thorough medical examination must also be carried out in order to exclude patients who have cardiovascular and/or orthopedic-musculo-skeletal contraindications [3, 7]. Muscle atrophy, which may occur as a result of aging, long-term bed confinement, a sedentary lifestyle or glucocorticoid therapy, must be evaluated and recorded.
For selected patients the beginning of a resistance-training program may be considered in phase II and III of cardiac rehabilitation. In phase I, resistance training is contraindicated. Risk stratification can be made according to the exercise standards for testing and training (American Heart Association, 38, Table 1).
For risk ‘class A' there are no set limitations to physical activity. In ‘class A2', it is recommended, and in ‘class A3', it is imperative, that a medical examination and a stress-ECG be carried out before beginning intensive physical exercise. Supervised training, ECG or blood pressure monitoring are not obligatory. In untrained patients, it is advisable to begin with a 2–4 week aerobic training program before the resistance training is started.
Risk stratification according to the recommendations of the American Heart Association [1]
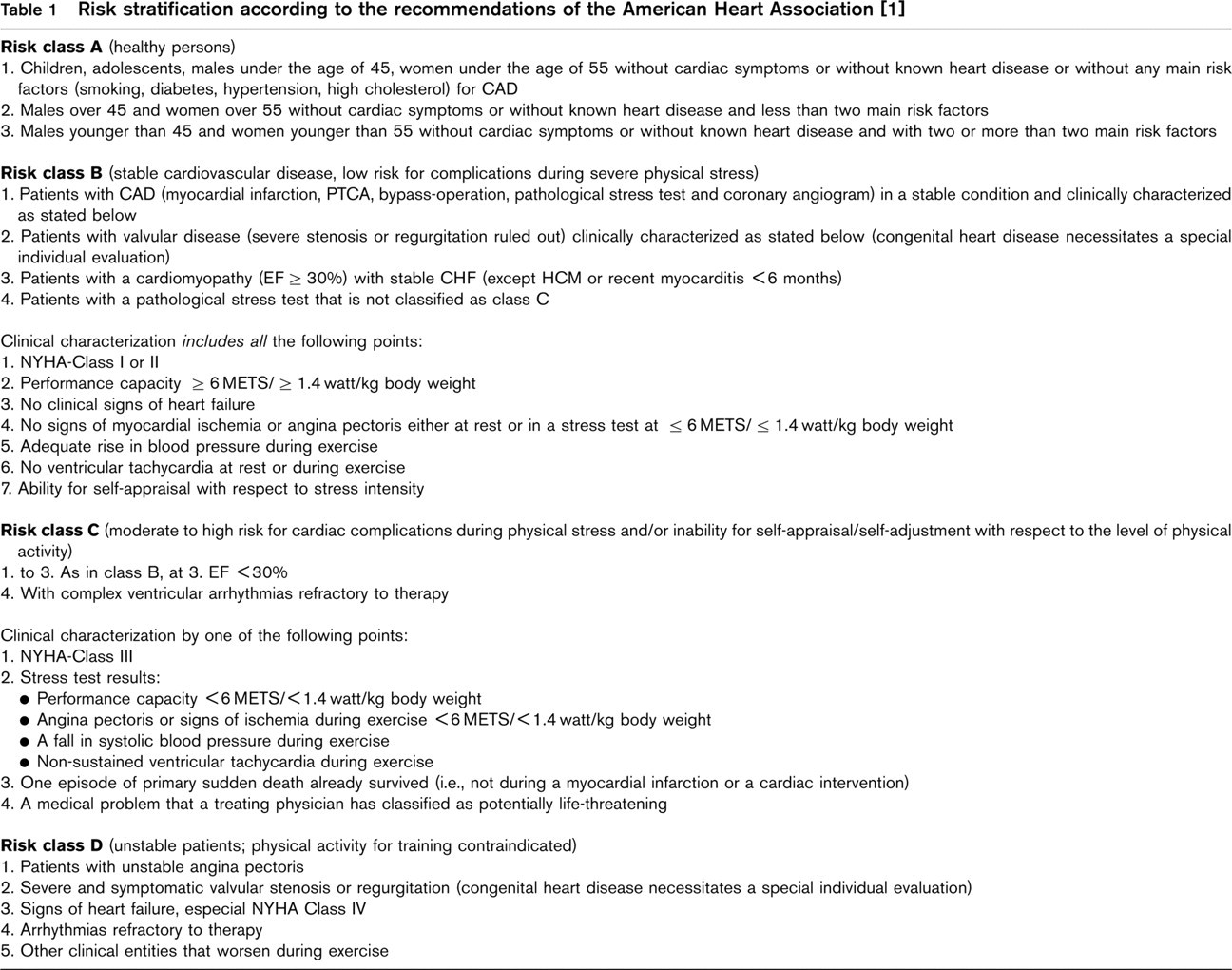
Risk ‘class B' is comprised of typical cardiac rehabilitation patients. The intensity of the physical activity must be individually adapted to the patient by qualified doctors according to the results of the patient's stress test. For members of this patient group a medically supervised, individually adapted and controlled resistance training program that is under the supervision of an experienced exercise therapist, can be recommended (there are no respective data for women). During the first several training units, ECG and blood pressure monitoring is advised along with keeping a record of subjective symptoms during training (Borg scale). Before these patients, with a low-to-moderate risk, begin resistance training, a 1–2 week aerobic endurance training program should be completed prior to the start of resistance exercise [3]. This also applies to patients after a percutaneous intervention (PTCA). After a myocardial infarction (MI), low-dose resistance training may be started at the earliest 2–3 weeks post-MI [3]. An experienced doctor (internist with experience in cardiac rehabilitation) must be available and individual consultation and patient guidance with the physician and therapist must be guaranteed.
For patients in risk ‘class C' there are no randomized, controlled studies dealing with the efficacy and safety of resistance training. For this patient group, more high quality investigations of the hemodynamic effects of resistance stress are needed. The results of several small studies have indicated that this patient subset does profit from resistance training when done in a suitable manner. Due to the lack of data, however, this cannot be incorporated into the general recommendations in all cases without restrictions. In these patients it is necessary that an individual risk assessment be done before the start of a resistance training program. The resistance training should begin at low intensity (30% MVC) and, given that training continues without complications, may be gradually increased. Medical supervision and patient guidance from an experienced and qualified therapist are mandatory. The same safety aspects as in risk ‘class B' apply here as well.
For the risk ‘class D', resistance training is contra-indicated. Absolute contraindications for resistance exercise are: unstable angina pectoris, poorly controlled high blood pressure (systolic BP >160 mmHg, diastolic BP >100 mmHg), uncontrolled arrhythmias, heart failure (not sufficiently diagnosed and/or controlled or treated), severely stenotic and incompetent heart valves and hypertrophic obstructive cardiomyopathy [3].
Special problem situations
‘The elderly patient'
In cardiac rehabilitation programs, patients older than 65 need special attention. In addition to the increased risk of myocardial infarction and arrhythmias, various comorbidities must be taken into consideration (vascular, orthopedic/joint, metabolic problems etc.). This situation, often combined with muscle deconditioning, makes it necessary to begin training in frequent units of low intensity (40–50% of VO2max) and short duration. Psychosocial problems must also be addressed. These aged patients are often classified in ‘group C'. In this age group, the stabilization and improvement in flexibility and muscle strength is especially important with respect to the maintenance of an independent lifestyle. This aspect is actually more important than their improvement in endurance capacity. As already mentioned, there are no existing data for this patient group and therefore clear recommendations for resistance exercise in this group cannot be given. Low-dose resistance training may, however, have very valuable effects in this patient group. For example, monitored interval training (ECG and blood pressure) on a bicycle ergometer could be done, also as an adjunct to endurance training.
After cardiac operations
After a thoracotomy (on or off-pump) and/or saphenect-omy, the patients' capacity for physical activity is limited. Wound healing takes approximately 4–6 weeks. Physical exertion, which causes tangential vector forces in the sternal area (pressure or sheering stress), should be avoided for 3 months postoperatively. Before resistance training is started, the treating physician must confirm that the sternum is stable [3, 7]. If there are no complications during the postoperative course, and the patient has a good cardiac performance capacity, a light, low-dose resistance exercise program focusing on the lower extremities can be carried out earlier. A stable body trunk is required. Quite often, muscular deconditioning is present and when taking the wound healing into consideration, the patients are generally classified in ‘group C' for the first 3–4 weeks postoperatively.
After cardiac transplantation
In cardiac transplant patients, the continuous postoperative glucocorticoid therapy can lead to muscle atrophy and a decrease in bone mass. This is usually in addition to a previously poor musculoskeletal state and as a consequence, the daily physical stress tolerance in these patients is often extremely low. Specific exercises designed to increase muscle strength are quite effective in this patient group. It is recommended that in clinically stable patients, individually adapted, moderate resistance training can begin as soon as possible in the postoperative phase with the aim to counteract the negative side-effects of the operation [31, 33].
After percutaneous coronary intervention (PTCA/stent)
There are no existing studies reporting conclusively how soon physical training can be started after an intervention. It is recommended that training should not be performed earlier than the second to seventh postinterventional day. Attention must be paid to any symptoms of angina pectoris and to possible complications of any indwelling catheters. Even if the post-PTCA/post-stent patient has seemingly good cardiac performance capacity, he should first take part in a 1–2 week aerobic training program.
Heart failure
Exercise intolerance in patients with chronic heart failure (CHF) shows no correlation to the degree of left ventricular dysfunction [73]. A reduction in exercise capacity is much rather related to morphological [24, 74], metabolic [75, 76] and functional changes [77] in the patient's peripheral musculature. Without intervention, disease-related loss of function, combined with early signs of fatigue, lead to a decrease in muscular activity which consequently result in muscle wasting, which then, in turn, leads to more fatigue and more physical inactivity and further muscle atrophy (so-called muscle hypothesis in chronic heart failure) [78]. An aerobic endurance-training program may increase the physical performance capacity of stable chronic heart failure (CHF) patients by 12–21% (measured in %VO2max) [79, 80]. Beyond these symptomatic benefits, physical activity also counteracts the intrinsic changes in the peripheral musculature: the number of mitochondria and the oxidative capacity are increased [81], inflammation is reduced [82] and anti-apoptotic factors are increased (e.g., insulin-like growth factor-1 [IGF-1]). In contrast to previous fears, aerobic endurance training actually leads to a reduction in after-load with a decrease in systemic resistance at rest and at maximal exertion as well as to a small improvement in left ventricular ejection fraction [83]. One mono-centre study, even demonstrated a reduction in mortality [84]. Similar data for resistance training in CHF patients do not exist. Aerobic endurance training thus still forms the basis of training therapies for CHF patients [85]. Critical appraisal of (predominantly) isometric resistance training (hand-grip training, stress time > 3 min) is based on older studies that found a drastic rise in after-load along with an acute reduction in cardiac output [86, 87] and an increase in the severity of mitral regurgitation [88]. Contrary to these findings, 2 × 10 repetition leg-press exercises at 70% of maximal capacity or interval training do not cause a decrease in ejection fraction or an increase in systolic blood pressure [71, 89, 90]. By shortening the isometric and lengthening the isotonic phase of the exercise, it is possible to avoid haemodynamic strain. Pure resistance training in CHF patients leads to an increase in muscular strength. There is, however, no accompanying increase in maximal O2-uptake [72]. It is only through the combination of resistance with endurance training that the important prognostic marker VO2max can be improved [91]. A combination of resistance with endurance training seems to promote anti-inflammatory responses as with aerobic endurance training alone [82, 92].
Experimental studies with animals have shown that resistance training leads to enhanced local expression of IGF-1 [61]. In this way it may be possible for supplementary, individually adapted resistance training of specific extremities to positively influence the catabolic breakdown of muscle tissue that is often associated with congestive heart failure. Specific data relating to this are still lacking.
To summarize, patients in risk groups ‘B' and ‘C' may benefit from a resistance training program with short stress phases (10 repetitions max.) at < 60% MVC, interrupted by phases of muscle relaxation, without causing haemodynamic deterioration. As a supplementary training modality, resistance training can complement, but not replace, the well-established aerobic endurance training.
Directions for training implementation
When choosing a certain exercise and considering its implementation in cardiac rehabilitation, the safety of the patient must be the primary concern. The training program must be individually adapted to the patient by an experienced exercise therapist and be under medical supervision. Formulating attainable training objectives and discussing them thoroughly with the patient is mandatory. Each patient must also be individually introduced into the training regimen. Table 2 shows recommendations for the implementation of a resistance endurance and muscle build-up training program in cardiac rehabilitation.
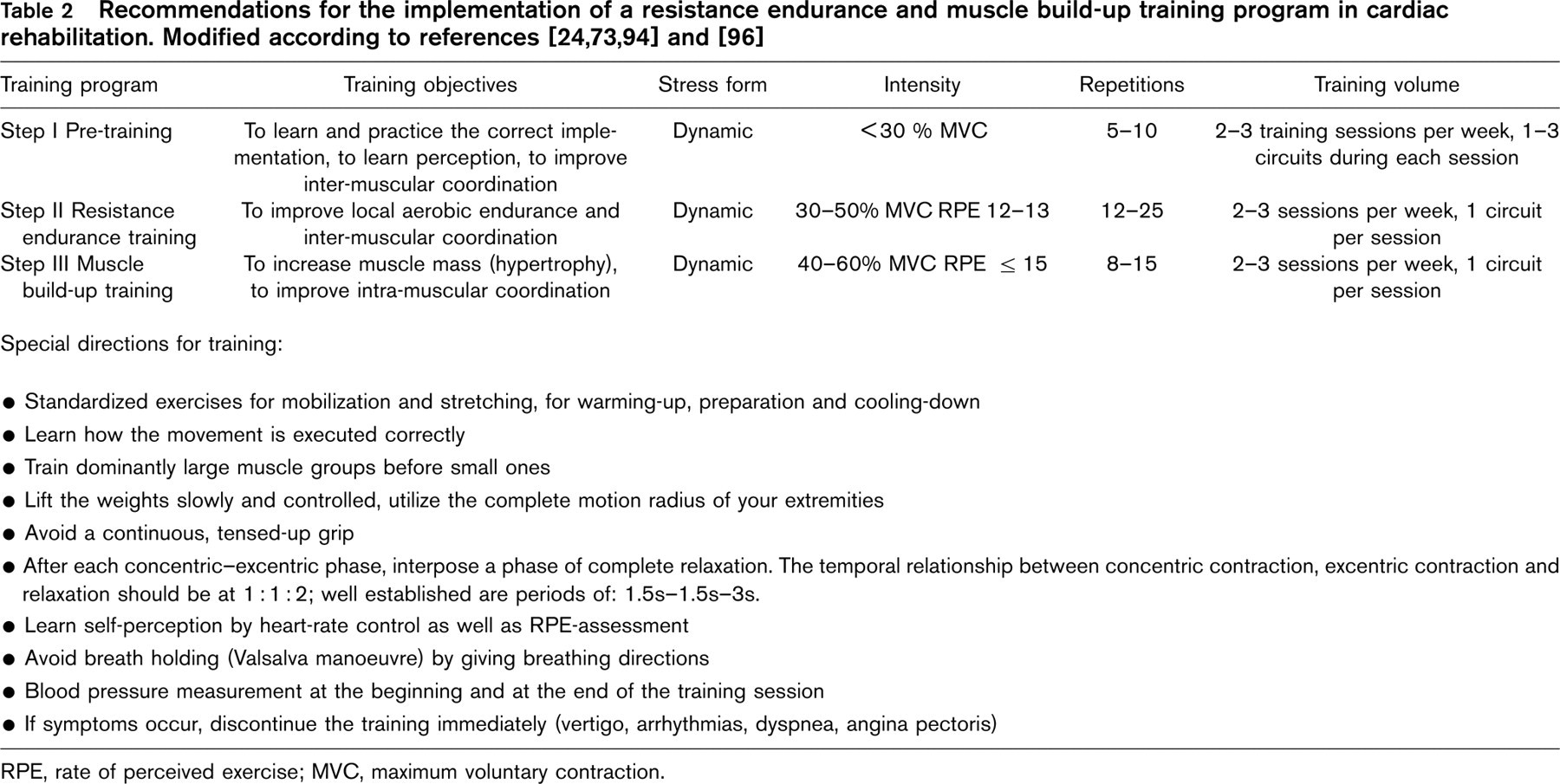
RPE, rate of perceived exercise; MVC, maximum voluntary contraction.
To minimize increases in blood pressure, resistance training of cardiac patients should involve mostly dynamic stress as opposed to pure static (i.e., isometric) stress, which should be avoided. The danger of the Valsalva manoeuvre is especially high during isometric stress. In addition, it is difficult to prescribe the appropriate level of training because each patient trains more or less intensively, according to his/her motivation, personality or other factors.
Before the actual training starts and during the first few training units, the patient must be adequately prepared for the subsequent training stimuli and stressors through improved inter-muscular coordination and physical perception. At the same time, the patient must carefully learn how to carry out the training exercise in the correct manner. This pre-training is to be done slowly, with only a few repetitions (approx. 5–10) and at a very low intensity (<30% MVC, or without resistance).
For cardiac patients, combined endurance and resistance training is the method of choice, i.e., dynamic training with many repetitions (12–25) and a low-level of intensity (30–50% MVC). When a resistance endurance training program (2–3 times per week for 4–6 weeks) at this level has been successfully completed without any complications, the patient can proceed to resistance training at higher intensity (40–60% MVC) in order to increase muscle mass. In resistance training of cardiac patients, the use of elastic bands (Theraband) and/or small weights is very suitable. More precise training with less risk of overloading can be achieved through the use of training machines, whereby the load dose can be individually adjusted and the execution of the movement is predetermined. The bicycle ergometer is also a suitable apparatus for interval training of the lower extremities and it allows for patient monitoring (ECG/BP), if necessary.
In order to find the correct intensity, it is important to consider that the same exercise may lead to different levels of stress in different patients. Factors such as body weight, coordination, intention and athletic confidence play a role. The correct dosage depends largely upon the patient's subjective perception of the stress during training.
The development of the patient's level of motor and stress coordination and body awareness is an important prerequisite when determining the appropriate load of resistance training. Use of the Borg perception scale [93], among other things, can be helpful. In order to prevent cardiac overload and injury, training should be started at low intensity and begin at 30–50% MVC [94]. If the patient has low stress tolerance and/or is elderly, training should start at 30% MVC. Patients with better performance capability can start at up to 50% MVC [3]. The exercise should be easy to complete, have 12–15 repetitions without breath holding (Valsalva manoeuvre) and should not generate cardiovascular symptoms. Well-trained patients with a good cardiac performance capacity and low cardiac risk, who have completed a 4–6 week training program may increase the load and adjust it according to their individual stress awareness. This only applies, however, to acceptable stress values of up to 60% MVC [3, 35, 94], and should only be done after conferring with the treating physician and supervising therapist. When determining the correct training intensity, a maximal strength test is unsuitable for cardiac patients because it leads to abdominal straining (Valsalva manoeuvre) and blood pressure elevations. The correct intensity can be found by using a graded stress test beginning at a very low intensity which the patient can overcome without difficulty and then gradually increasing the resistance. The point at which the patient achieves 10–15 repetitions without abdominal straining and without symptoms is the training intensity to be used. In order to prevent breath holding (Valsalva manoeuvre), the patients must be instructed to breathe out during the contractive phase (e.g., breathe out when the weight is lifted above the head) and breathe in when the weight is lowered (relaxation phase). When assessing the load on a patient the Borg's scale [93] provides the patient's own subjective stress perceptions in addition to the measured objective physiologic parameters. In patients with moderate risk, stress perception should be at a maximum rate of perceived exertion (RPE) of 15 or lower (RPE 12–13) [3]. In resistance training, the heart rate attained does not necessarily reveal the actual stress intensity. Monitoring the heart rate can however be helpful for the patient's self-perception and can prevent the patients from exceeding their maximal heart rate limits at high training intensities. Monitoring blood pressure elevations would be helpful, but this cannot be achieved with the usual standard methods. Likewise, measuring the blood pressure at the end of training does not reflect blood pressure elevations that occur during training, because blood pressure falls rapidly upon resting. A blood pressure measurement taken before and after training is, however, important for supervision and documentation purposes. The main training effect is achieved during the first set of exercises. Studies demonstrate that adding a second or third set does not provide any significant additional strength augmentation [95]. The main focus should be on a versatile, all-round training program whereby many different muscle groups are conditioned rather than carrying out many sets with few exercises [1, 3]. Two to three training units per week are recommended keeping in mind however that 75% of the benefits of training are attained from training only twice a week rather than three times a week. Training and rest days should alternate with one another.