
Abstract
Background
The moderate increase in postprandial plasma glucose in subjects with impaired glucose tolerance has been shown to be a predictor of cardiovascular disease. In the randomised STOP-NIDDM trial, we could demonstrate that lowering postprandial plasma glucose with acarbose in subjects with impaired oral glucose tolerance could reduce the risk of diabetes.
Methods
The current report focuses on the effect of acarbose on silent ischaemic events evaluated in the electrocardiographic substudy, using the Minnesota code classification.
Results
A total of 1181 patients were included in the ECG substudy. From these 72 patients had significant changes between the baseline and end of treatment ECG, 33 in the acarbose and 39 in the placebo group. Higher rates of myocardial infarctions occurred in the placebo group (P=0.07 with Fisher's Exact test and P = 0.023 with Chi-square test), while there were no differences between the two groups with ECG changes classified under the other Minnesota codes.
Conclusions
In this prospective intervention study we could show that acarbose, by decreasing postprandial hyperglycaemia, can reduce the incidence of silent myocardial infarctions in subjects with impaired glucose tolerance. This approach should therefore be evaluated in other higher risk populations.
Introduction
A cardiovascular complication is the predominant cause of death among patients with type II diabetes; accounting for about half of the total mortality [1]. Recently, attention has been given not only to fasting, but also to postprandial hyperglycaemia as a risk factor for cardiovascular disease in non-diabetic as well as in diabetic populations [2–4. It has been shown that an abnormal oral glucose tolerance test is a good surrogate for postprandial glucose evaluation [5]. There is evidence that the development of cardiovascular complications start well before the development of diabetes [6]. A number of studies have now independently confirmed that the risk of cardiovascular disease is increased in subjects with impaired glucose tolerance (IGT). The increase in postprandial plasma glucose in these subjects with IGT [7] has been shown to be a predictor of cardiovascular disease [8,9]. Acarbose is an α-glucosidase inhibitor, which prevents postprandial glucose peaks by reducing the digestion of oligosaccharides in the upper part of the small intestine and therefore delaying the absorption of monosaccharides and spreading it over a longer time. Hence, the postprandial phase is lasting longer and the early-phase insulin secretion and hyperinsulinaemia is minimized.
In the randomised STOP-NIDDM trial, we could demonstrate that lowering postprandial plasma glucose with acarbose in subjects with impaired oral glucose tolerance could reduce the risk of diabetes [10]. One of the secondary endpoints of this trial was to evaluate the impact of decreasing postprandial hyperglycaemia with acarbose on the risk of cardiovascular events. The current report focuses on the effect of acarbose on silent ischaemic events evaluated in the electrocardiographic substudy, using the Minnesota code classification [11]. The Minnesota code is a useful tool in evaluating the incidence of silent cardiac events in population studies and correlates with the subsequent rate of death in subjects at risk for developing cardiovascular diseases [12–14.
Methods
The STOP-NIDDM trial was an international, double blind, placebo-controlled, randomised study that took place in nine countries (Canada, Germany, Austria, Norway, Denmark, Sweden, Finland, Israel and Spain). The study design and the methodology have been described in more detail elsewhere [9,15]. Patients aged between 40–70 years with a body mass index (BMI) between 25–40 kg/m2 were eligible for the study if they had IGT according to WHO criteria [7] (glucose between 140–200 mg/dl after oral 75 g glucose = oral glucose tolerance test), plus a fasting plasma glucose concentration between 100–140 mg/dl. An important exclusion criterion was any cardiovascular event within the last six months. After inclusion and informed consent patients were randomised to placebo or acarbose 100 mg three times daily, taken with the first bite of each meal. In addition all patients received an instruction on a weight-reduction or weight-maintenance diet and were encouraged to exercise regularly. The investigator saw all patients every six months. Additionally the coordinating nurse interviewed the patients every three months for the documentation of adverse events. All participants were asked to remain in the study until the last randomised subject has been treated for three years. Appropriate institutional review boards approved the protocol, and each subject signed an informed consent form.
It was pre-specified in the protocol to evaluate the effect of acarbose on the occurrence of clinically overt and silent cardiovascular events. By protocol, all subjects had an electrocardiogram done before randomisation and at the end of treatment. Two independent cardiologists, blinded to treatment, read these. The changes in the electrocardiograms between baseline and end of treatment were classified according to the Minnesota code [11]. Analysis was carried out considering several Minnesota code categories and grouping and it was restricted to subjects free from clinically diagnosed heart disease at entry examination. Myocardial infarction was considered in subjects with Minnesota code 0 at entry and code 1.1 or code 1.2 + 5.1 or 5.2 or code 1.3 + 5.1 or 5.2 [11–14.
The silent and clinical overt cardiovascular endpoints were analysed on the intention-to-treat basis. Fisher's Exact test was used to compare the actual incidences of events between the two groups. We performed a logistic regression analysis for the influence of treatment allocation and other baseline variables for the occurrence of myocardial infarctions. In the multivariate model only significant variables from the univariate analysis were kept using a backward selection process.
Results
A total of 1429 patients were randomised to acarbose (n = 714) or placebo (n = 715). Sixty-one patients were excluded because they did not meet the criteria for IGT (nine on acarbose and eight on placebo), or they had no valid post-randomisation data (23 on acarbose and 21 on placebo). Therefore the intention-to-treat population consisted of 682 patients in the acarbose group and 686 subjects in the placebo group. The two groups were well balanced with respect to their clinical and biochemical baseline characteristics [10]. The mean follow-up was 3.3 ± 1.2 years.
Patients with myocardial infarctions reported by the investigators and confirmed during the endpoint validation process were excluded from the ECG analysis. In some patients no paired ECGs were available or the quality of an ECG was not sufficient for the Minnesota coding process. A total of 1181 patients were included in the ECG substudy. From these 72 patients had significant changes between the baseline and end of treatment ECG, 33 in the acarbose and 39 in the placebo group (Tables 1 and 2). Higher rates of myocardial infarctions occurred in the placebo group (P = 0.07 with Fisher's Exact test and P = 0.023 with Chi-square test), while there were no differences between the two groups with ECG changes classified to the other Minnesota codes. There were five patients who showed improvements using the Minnesota code between baseline and end of treatment, two in the acarbose and three in the placebo group.
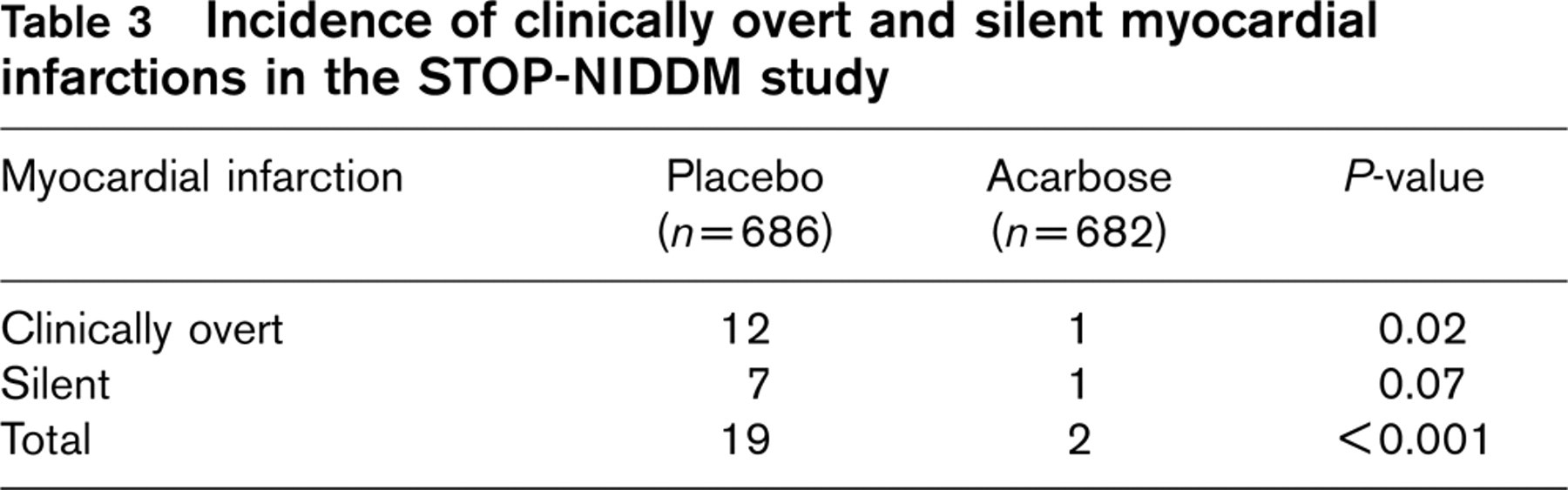
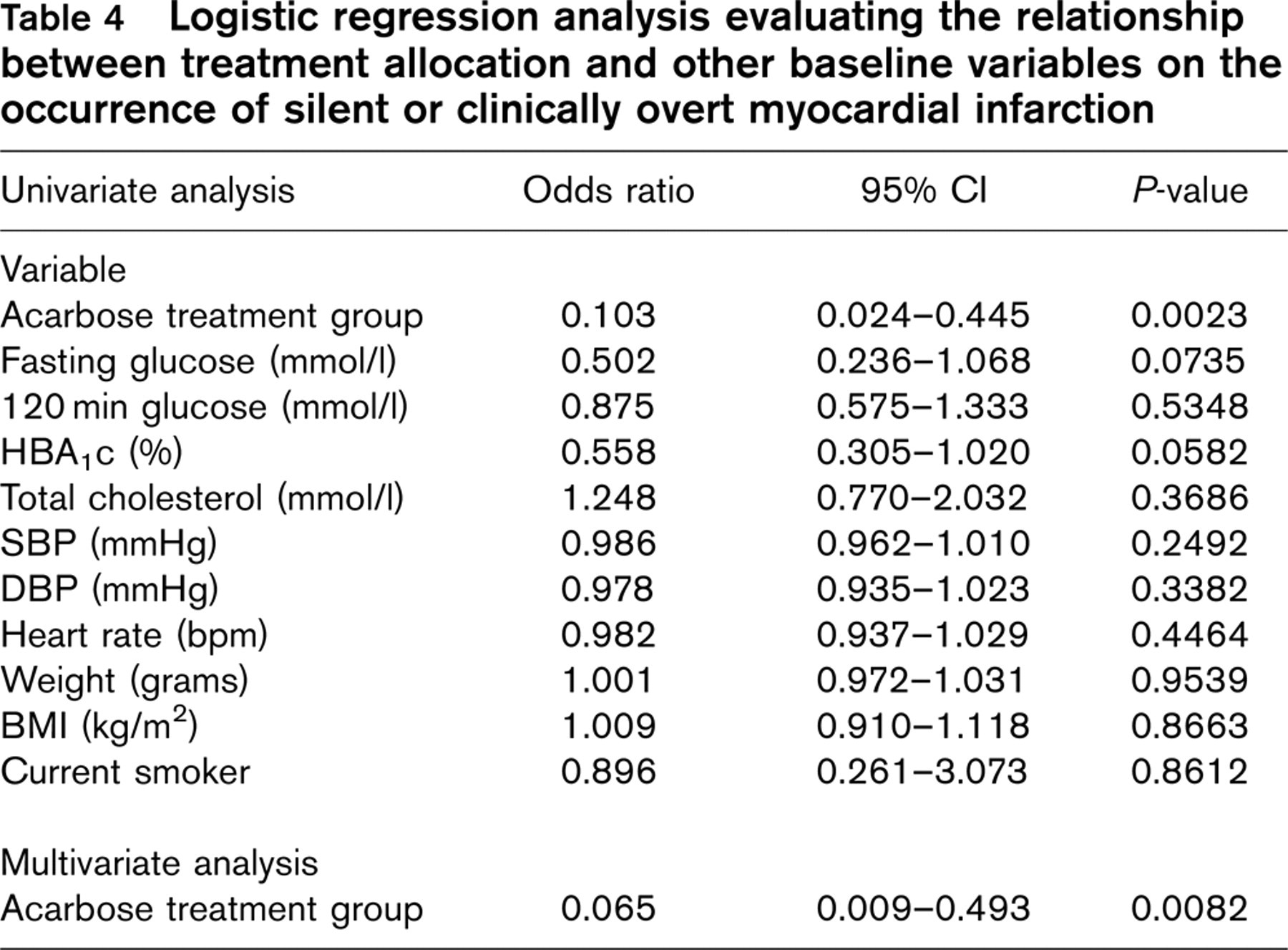
If the results of the clinical events, which are reported in more detail elsewhere [16] are included in the analysis, a total of two clinically overt and silent myocardial infarctions occurred under acarbose and 19 under placebo (P < 0.001) (Table 3). In a multivariate analysis (Table 4) acarbose treatment was independently associated with freedom of myocardial infarction.
Changes in the electrocardiogram between baseline and end of treatment classified according to the Minnesota code
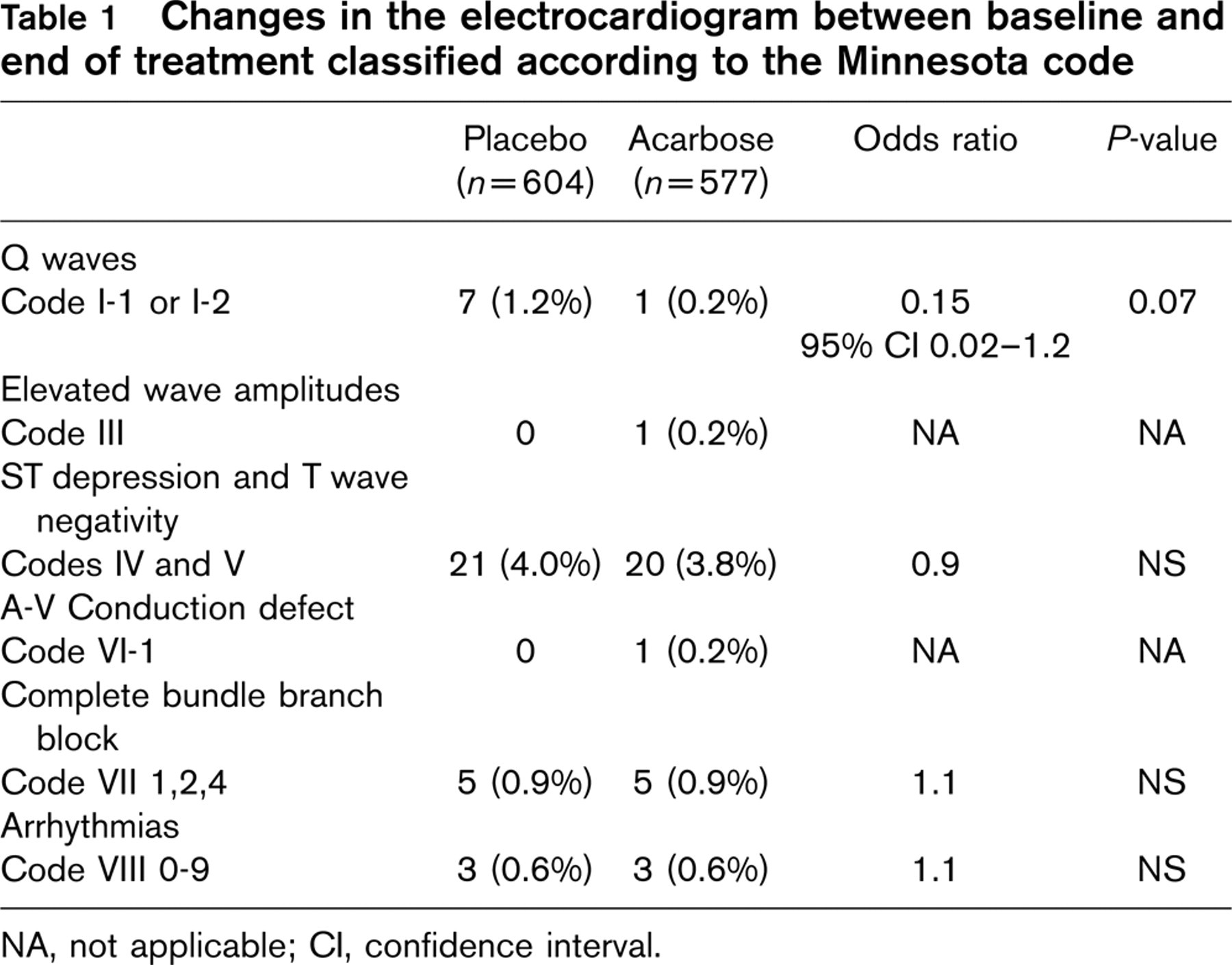
NA, not applicable; CI, confidence interval.
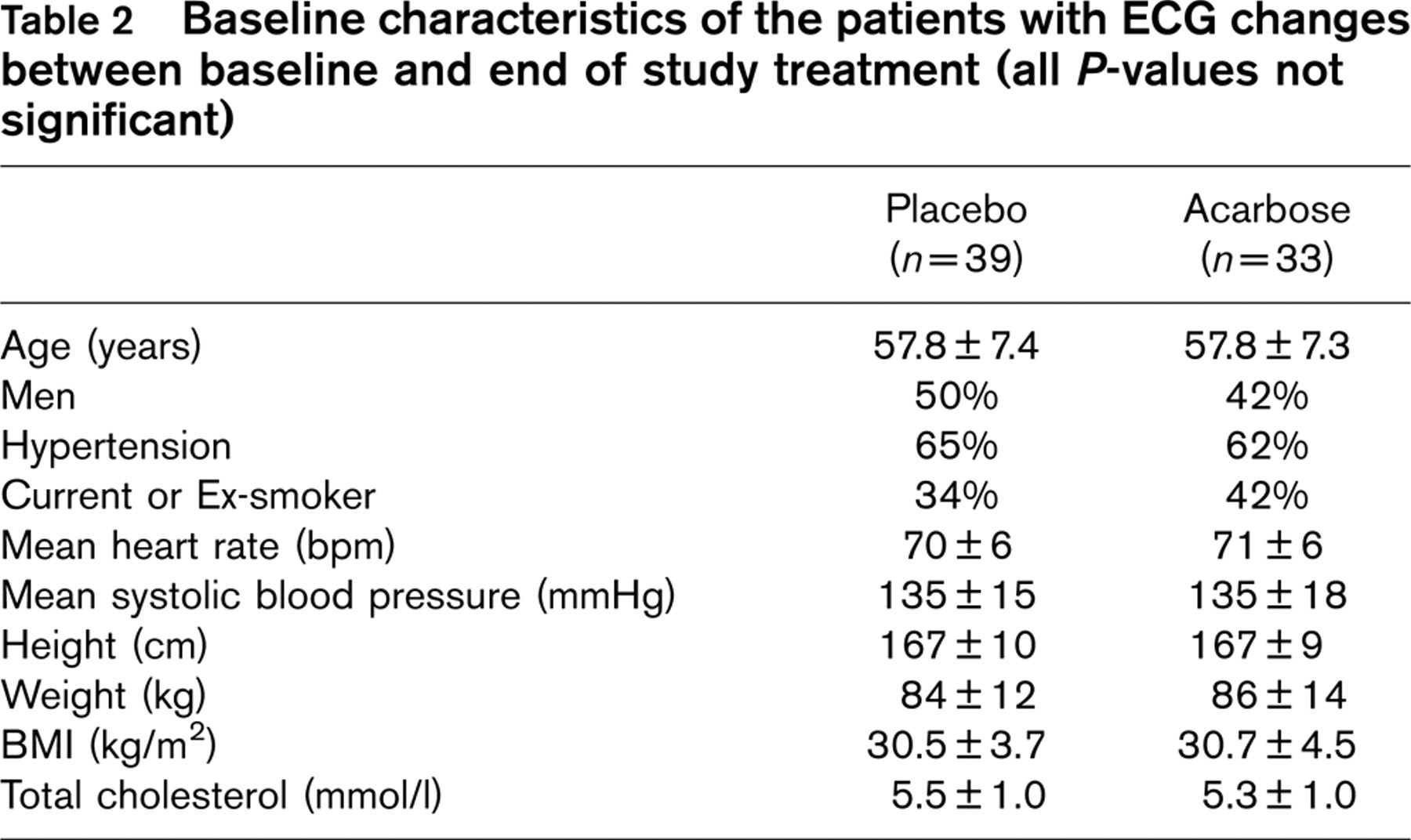
Baseline characteristics of the patients with ECG changes between baseline and end of study treatment (all P-values not significant)
Incidence of clinically overt and silent myocardial infarctions in the STOP-NIDDM study
Discussion
These data provide evidence that acarbose, by lowering postprandial hyperglycaemia, reduces the incidence of myocardial infarctions in a population with IGT characterized by moderate postprandial hyperglycaemia. Serial electrocardiographic changes of Minnesota code classifications have been shown to correlate with coronary deaths during follow-up, therefore incorporating these changes in the clinical event evaluation seems appropriate [12–14. We observed a lower incidence of silent myocardial infarctions in patients treated with acarbose. Since the incidence of other ECG findings not attributed to acute coronary events were equally distributed between the two groups, a chance finding for the lower rate of silent myocardial infarctions with acarbose seems unlikely. In addition the clinical events reported by the investigators show the same result with a higher rate of myocardial infarctions in the placebo group [16]. The pathophysiological relationship between postprandial hyperglycaemia and the development of myocardial infarction is not fully understood yet and awaits further research [17–20. Potential mechanisms include the production of glycosylation end products, enhancement of the polyol pathway, and activation of protein-kinase C inducing oxidative stress. Moreover, hyperglycaemia is associated with an increase and activation of pro-coagulation factors. Other mechanisms with impact on the cardiovascular event rate might be the loss of weight induced by acarbose and the effect of acarbose on short fatty acids [21,22]. All these potential mechanisms deserve further research in dedicated studies. However, our observations provide further support for the concept that postprandial hyperglycaemia is a risk factor for cardiovascular disease and provides a strong argument for the screening and treatment of subjects with dysglycaemia. Our findings of a beneficial effect of acarbose on cardiovascular events are supported by a recent meta-analysis of randomised studies in patients with type II diabetes [23]. Here acarbose was associated with a significant reduction in myocardial infarction (hazard ratio 0.36, 0.16–0.80) and the occurrence of any cardiovascular event (hazard ratio 0.65, 0.48–0.88).
Logistic regression analysis evaluating the relationship between treatment allocation and other baseline variables on the occurrence of silent or clinically overt myocardial infarction
In summary, in this prospective intervention study we could show, that acarbose by potentially decreasing postprandial hyperglycaemia can reduce the incidence of silent myocardial infarctions in subjects with IGT. Although the mechanisms for the beneficial effect of acarbose await further research, this approach should be evaluated in other higher risk populations in prospective clinical trials.