
Abstract
Purpose
The purpose of this study was to describe the impact of self-report heart disease, other chronic comorbidities, and perceived health status on activity limitation among community dwelling persons older than 50 years of age.
Methods
Odds ratios for activity limitation in activities of daily living, mobility, and other activities were estimated for respondents with self-report heart disease, eight other chronic comorbid conditions, and perceived health status using data generated in two nationally representative cross-sectional surveys, the Health and Retirement Survey (HRS; respondents aged 51 to 60 years) and the Assets and Health Dynamics of the Oldest Old study (AHEAD; respondents aged 70 years and older).
Results
The prevalence of activity limitation increased significantly across the spectrum from activities of daily living to mobility to other activities in both surveys in respondents with and without heart disease. There was a significantly increased likelihood of mobility and other activity limitation among those with heart disease. Among the HRS respondents with heart disease, five or more of the eight comorbid conditions plus poor or fair perceived health were associated with a significantly increased limitation in each activity category. Among the AHEAD respondents with heart disease, three comorbid conditions plus perceived health were associated with a significantly increased limitation in activities of daily living whereas six comorbid conditions plus perceived health were associated with a significantly increased limitation in mobility and in other activities.
Conclusions
As a prime objective of cardiac rehabilitation is to reduce activity limitation, the strong associations between comorbidity and activity limitation observed in this study among persons older than 50 years with heart disease suggest that the burden of comorbidity-associated is considerable but should not be an automatic exclusion criterion for referral to cardiac rehabilitation. The lack of rigorous scientific information on how these associations may influence clinicians who refer patients to rehabilitation and those who manage these programs strongly reinforces the need for more research to explore the real-world spectrum of comorbidity among persons with heart disease and the impact on activity limitation.
Introduction
The eligibility criteria cited in many published trials of physical activity cardiac rehabilitation often ruled out older patients who frequently have activity limitations and this unwittingly may have limited physician referral to and patient requests for cardiac rehabilitation services [1,2]. A number of recent cardiac rehabilitation trials have included patients 65 years of age and older [3,4] and in our recent randomized clinical trial of cardiac rehabilitation in patients with myocardial infarction (MI) from 45 to 86 years of age we observed similar adverse event rates and similar relative improvements in work capacity and health-related quality of life in the younger and older intervention patients [4]. Despite the increasing body of rigorous scientific evidence about the safety and effectiveness of cardiac rehabilitation in older patients with heart disease [5], the elderly are an important target population for research where there is special need to focus on strategies aimed at reducing barriers to referral to cardiac rehabilitation services [6].
The World Health Organization has replaced the term ‘disability’ in the International Classification of Impairments, Activities, and Participation (ICIDH-2) with “activity limitation” which is now considered in terms of performance and difficulty in accomplishing an activity or task [7]. An important predictor of activity limitation and health status in older persons is the presence of heart disease [8–13 with activity limitation reported by 37% and fair to poor health status reported by 28% persons 65 years and older [14]. However, heart disease itself may not be as strong a predictor of activity limitation as assumed [15,16]. The real-world spectrum of illness is that many elderly patients with heart disease, who would otherwise be eligible for referral to exercise training cardiac rehabilitation, frequently have activity limitation that may be associated with comorbid conditions, psychiatric illnesses, medications, and social situations. Some of relatively limited penetration of cardiac rehabilitation in the overall management of heart disease [5,17] may be associated with a reluctance to refer older patients with heart disease, comorbidity, and activity limitation to cardiac rehabilitation even though one of the explicit goals of cardiac rehabilitation is to reduce activity limitation [6].
The purpose of this report is to describe and explore the relationships between heart disease, selected comorbidities, and perceived health status and activity limitation, specifically activities of daily living (ADLs), mobility, and other activities among 17,272 community-dwelling respondents in two nationally representative cross-sectional surveys, the Health and Retirement Survey [HRS] for adults aged 51 to 61 years (middle-age; n = 9,825) [18] and the Assets and Health Dynamics of the Oldest Old (AHEAD) for adults aged 70 years and over (old; n = 7,447) [19].
Methods
Sample
The 1992 HRS [18] and the 1993 AHEAD study [19] were conducted by the Institute for Survey Research at the University of Michigan and funded by the National Institute on Aging. The AHEAD survey of persons 70 years of age and older was initiated as a supplement to the HRS in 1992 so ‘taking advantage of the opportunity afforded by the existence of the screening sample … [of the HRS] … to develop a study of the very old’ [20]. The differences between the two surveys were minimized by adapting the survey design of the HRS to make it suitable for studying older persons and by smoothing existing differences, for example, measures were included in the AHEAD if they represented significant variables in models of behavior among the elderly [19]. The major difference in the items associated with activity limitation was a greater emphasis on ADLs and lower-level physical functions in the AHEAD whereas the items in the HRS focused on higher-level physical function [19].
Households (approximately 70 000) obtained through an area probability sample were screened for age-eligible persons. The HRS was targeted to middle-aged persons, 51 to 61 years of age, and the AHEAD focused on people 70 years and older. All age-eligible persons residing in a household were selected for the HRS. In the AHEAD, if more than one age-eligible individual was residing in the household, one individual was randomly selected.
Response rates at baseline were 82% for the HRS and 80% for the AHEAD and previous reports have shown that non-respondents did not differ significantly from respondents [18,19]. Census tracts containing a high-density of African Americans or Mexican Americans were over-sampled 2 : 1 in the HRS and 1.8 : 1 in the AHEAD.
Clinical and demographic measures
All data for both the HRS and AHEAD were obtained through face-to-face interviews that lasted an average of 1h. The HRS and AHEAD data, as in many federal surveys (e.g., the National Health and Nutrition Examination Survey and the Behavioral Risk Factor Surveillance System), are self-report with the medical indicators for both surveys created according to the same question. If participants responded ‘yes’ to this question, they were then asked two ‘yes/no’ follow-up questions with respect to their angina and/or myocardial infarction. The actual questions about heart disease were as follows: ‘Has a doctor ever told you that you had a heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems?'. If the respondent answered ‘yes’ they were then asked: ‘Did you have a heart attack or myocardial infarction?’ and ‘Do you currently have any angina or chest pains due to your heart?'.
This approach allowed the classification of both HRS and AHEAD respondents into a self-report ‘heart disease’ or ‘no heart disease’ category with the following specific heart disease diagnostic categories: angina only; MI only; angina + MI; and other heart disease. In the same way, respondents were asked to identify the following eight self-report comorbidities: arthritis; cancer; diabetes; hypertension; low back problems; lung disease; overweight (body mass index); and stroke and perceived health status (poor + fair/good + very good + excellent).
Standard measures of gender, race, income, personal net worth, private or supplemental insurance, education, smoking status, and alcohol use were available.
Activity limitation measures
The self-report activity limitation items used in both surveys are aggregated into three indices: ADLs, mobility and other activities [18,19]. For this report, we coded each index as ‘yes’ if there were two or more activity limitations in an index or as ‘no’ if there were only one or no activity limitation. The AHEAD activity limitation items (n = 10) are a subset of the HRS items (n = 16) and, because of the differences in age in the HRS and AHEAD cohorts, were specifically chosen to represent the activities expected in the more functionally limited older aged AHEAD cohort [19].
The activity limitation items used in the HRS activity limitation are as follows (the AHEAD items are underlined): ADLs – (1) bathing, (2) eating, (3) dressing, (4) walking across a room, (5) getting in and out of bed, and (6) getting up from a chair; mobility – (1) walking several blocks, (2) walking one block, (3) climbing several flights of stairs, and (4) climbing one flight of stairs; other activities – (1) stooping, (2) sitting for 2 h, (3) reaching arms over head, (4) lifting 10 lbs, (5) pulling or pushing large objects, and (6) picking up a small coin. This means that direct age-specific comparisons for each activity limitation category are not possible as the items in the HRS and AHEAD surveys are different but that condition-specific comparisons are available within each of the two age groups.
Although self-report data are less reliable than diagnostic or medical record data, recent reports have shown that test–retest reliability of self-report medical conditions and activity limitation is well over 80% [15, 21,22] with positive associations between mobility limitation and self-related health [23] and between performance-based scores and self-report disability [24].
Analyses
All analyses were stratified by survey (age group) and weighted to account for the sampling schemes [18,19]. The software package SUDAAN was used in all analyses to adjust for the complex sampling scheme in both groups [25]. We first compared the prevalence estimates of the demographic and clinical variables in each survey; the observed prevalences are considered significantly different when the 95% confidence intervals do not overlap. We then generated odds ratios (OR) with 95% confidence intervals (95% CI) for the activity limitation categories and the activity limitation predictor variables using logistic regression models; the ORs are considered significant when the 95% CIs do not include 1.00. The following demographic and clinical predictor variables were included in each of the models: age (years), gender (male/female), race (white/ non-white), income (≥$10000, ≤$9999), private insurance (yes/no), education (years), smoking status (yes/no), alcohol use (yes/no); self-report arthritis, cancer, diabetes, heart disease, hypertension, low back problems, lung disease, overweight (body mass index), stroke, and perceived health (poor + fair/good + very good + excellent).
Results
Demographic and clinical characteristics
Descriptive statistics (with 95% confidence intervals) are presented in Table 1 for the demographic and clinical characteristics of the middle-age HRS and the old AHEAD respondents. The HRS respondents were significantly more likely than the AHEAD respondents to be male and white, to have an income of more than $10 000, private health insurance, and more years of education, and to smoke and use alcohol. The HRS respondents were less likely than the AHEAD respondents to report heart disease, diabetes, hypertension, lung disease, cancer, stroke, and poor/fair perceived health but more likely to report arthritis, low back problems, and a higher body mass index. With specific reference to heart disease, the HRS respondents were significantly less likely than the AHEAD respondents to report angina only and other heart disease with no difference in the prevalence of MI only or angina plus MI.
Activity limitation prevalence
There was a progressive and significant increase in the prevalence of limitation in ADLs, mobility, and other activities among all HRS and AHEAD respondents and also among those with and without heart disease in each survey (Table 2).
Odds ratios and predictor variables for activity limitation
For both the HRS (Table 3) and the AHEAD (Table 4) surveys, we first present the ORs for activity limitation among all respondents by presence or absence of the condition and then present the ORs by presence or absence of the coexistence of a comorbid condition in respondents with heart disease.
Among all HRS respondents (Table 3a), the highest ORs for ADL, mobility, and other activity limitation were observed in respondents with comorbid back problems (OR = 5.20, 3.03 and 4.74, respectively) and with poor to fair health compared to good or excellent health (OR = 4.10, 4.03 and 3.48, respectively). Heart disease was associated with a lower, but still significantly increased, OR for mobility and other activity limitation (OR = 1.73 and 1.63, respectively] but not for ADLs. None of the heart disease diagnoses were associated with an increased OR for ADL limitation, all were associated with mobility limitation, and all except ‘angina only’ were associated with other activity limitation.
Among HRS respondents who reported having heart disease (Table 3b), (i) all comorbidities, except hypertension and cancer, were associated with an increased likelihood of ADL limitation; (ii) all comorbidities, except cancer and stroke, were associated with an increased likelihood of mobility limitation; and (iii) all comorbidities, except diabetes and hypertension, were associated with an increased likelihood of other activity limitation. Limitation in each activity category (ADL, mobility, and other activities) was increased among middle-aged HRS respondents with self-reported heart disease and (a) comorbid arthritis (OR = 2.52, 1.87 and 1.90, respectively], (b) low back problems (OR = 3.68, 2.01 and 2.76, respectively), (c) lung disease (OR = 1.60, 1.96 and 2.01, respectively), and (d) fair or poor health compared with good or excellent health (OR = 3.19, 4.60 and 3.15, respectively). Limitation in ADL and other activities was increased among HRS respondents with heart disease and comorbid stroke (OR = 2.64 and 1.90, respectively); limitation in ADL and mobility was increased among those with comorbid diabetes (OR = 2.22 and 1.80, respectively); and mobility limitation was increased among respondents with hypertension (OR = 1.07) and those who were overweight (OR =1.52).
Among all AHEAD respondents (Table 4a), the highest ORs for ADL, mobility, and other activity limitation were observed in respondents with poor to fair health (OR = 3.89, 4.28 and 4.55, respectively) and stroke (OR = 2.77, 2.30 and 2.79, respectively). Heart disease was associated with a lower, but still significantly increased, OR for mobility and other activity limitation (OR = 1.34 and 1.46, respectively). Among the heart disease diagnoses, angina only and angina + MI were associated with ADL and mobility limitation whereas MI only was associated with other activity limitation.
Among AHEAD respondents who reported having heart disease (Table 4b), (i) comorbid arthritis, diabetes, stroke, and poor and fair health were associated with an increased likelihood of ADL limitation, (ii) comorbid arthritis, diabetes, lung disease, stroke, being overweight, and poor and fair health were associated with an increased likelihood of mobility limitation, and (iii) comorbid arthritis, diabetes, cancer, lung disease, stroke, and poor and fair health were associated with an increased likelihood of other activity limitation. The likelihood of each limitation category (ADL, mobility, and other activities) was increased among AHEAD respondents with heart disease and comorbid (a) arthritis (OR = 1.88, 1.72 and 1.84, respectively], (b) diabetes (OR = 1.64, 1.73 and 1.39, respectively), (c) stroke (OR = 2.02, 2.06 and 2.29, respectively), and (d) fair and poor health (OR = 3.54, 4.41 and 5.03, respectively). In AHEAD respondents with heart disease there was a significant likelihood of mobility and other activity limitation in those with comorbid lung disease (OR = 2.38 and 1.96, respectively); mobility limitation was increased among overweight respondents (OR = 1.04); and other activity limitation was increased among respondents with cancer (OR = 1.52).
Demographic and clinical characteristics in the Health and Retirement Study (HRS) and the Assets and Health Dynamics of the Oldest Old (AHEAD) study
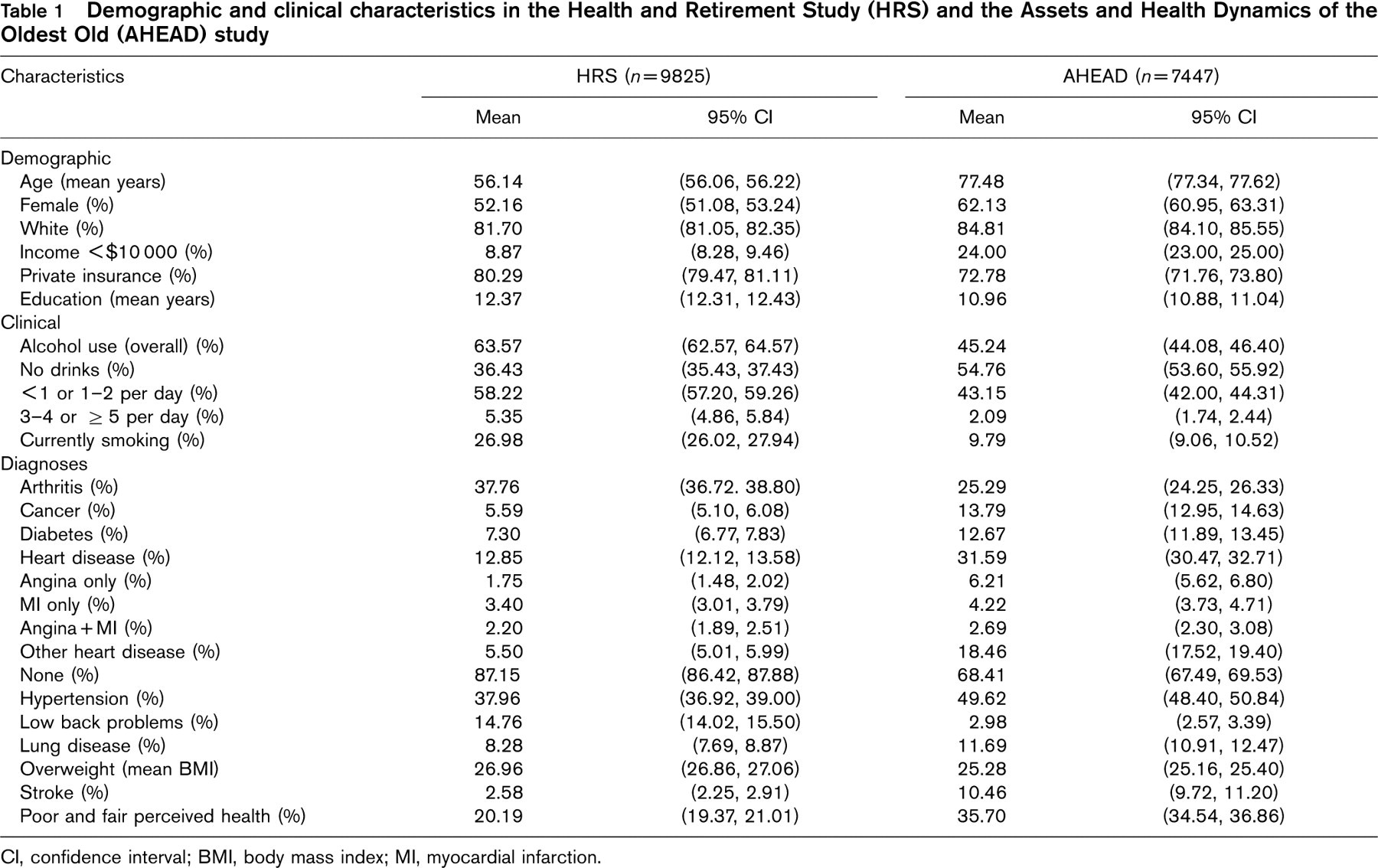
CI, confidence interval; BMI, body mass index; MI, myocardial infarction.
Prevalence of activity limitation outcomes (≥ 2 limitations in a category) for all patients and for patients with and without heart disease in the Health and Retirement Study (HRS) and the Assets and Health Dynamics of the Oldest Old (AHEAD) study
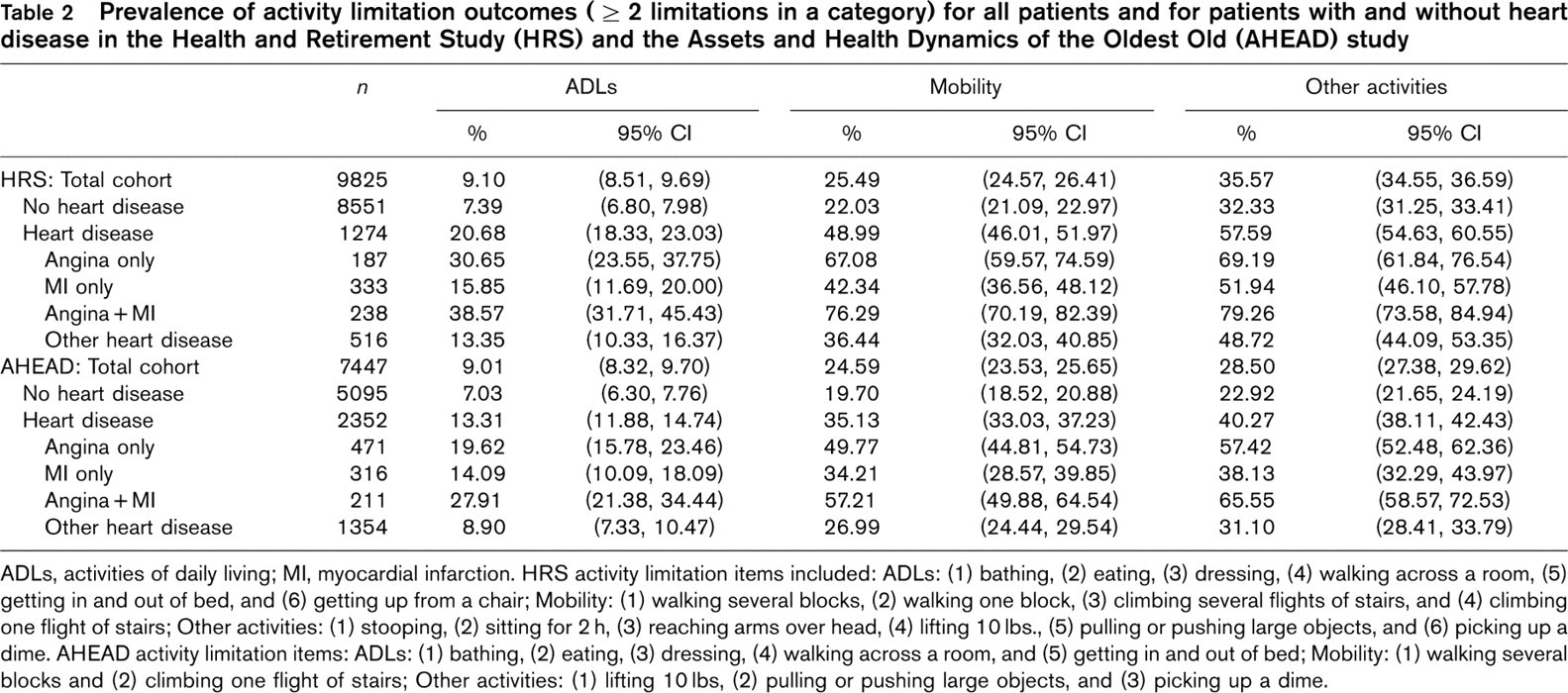
ADLs, activities of daily living; MI, myocardial infarction. HRS activity limitation items included: ADLs: (1) bathing, (2) eating, (3) dressing, (4) walking across a room, (5) getting in and out of bed, and (6) getting up from a chair; Mobility: (1) walking several blocks, (2) walking one block, (3) climbing several flights of stairs, and (4) climbing one flight of stairs; Other activities: (1) stooping, (2) sitting for 2h, (3) reaching arms over head, (4) lifting 10 lbs., (5) pulling or pushing large objects, and (6) picking up a dime. AHEAD activity limitation items: ADLs: (1) bathing, (2) eating, (3) dressing, (4) walking across a room, and (5) getting in and out of bed; Mobility: (1) walking several blocks and (2) climbing one flight of stairs; Other activities: (1) lifting 10 lbs, (2) pulling or pushing large objects, and (3) picking up a dime.
Odds ratios (OR) and 95% confidence intervals (CI) for respondents in the Health and Retirement Study with heart disease and comorbid conditions and perceived health status (a) among all respondents (n = 9825) with reference to those without the condition and (b) among those reporting heart disease (n = 1274) with reference to those with heart disease only
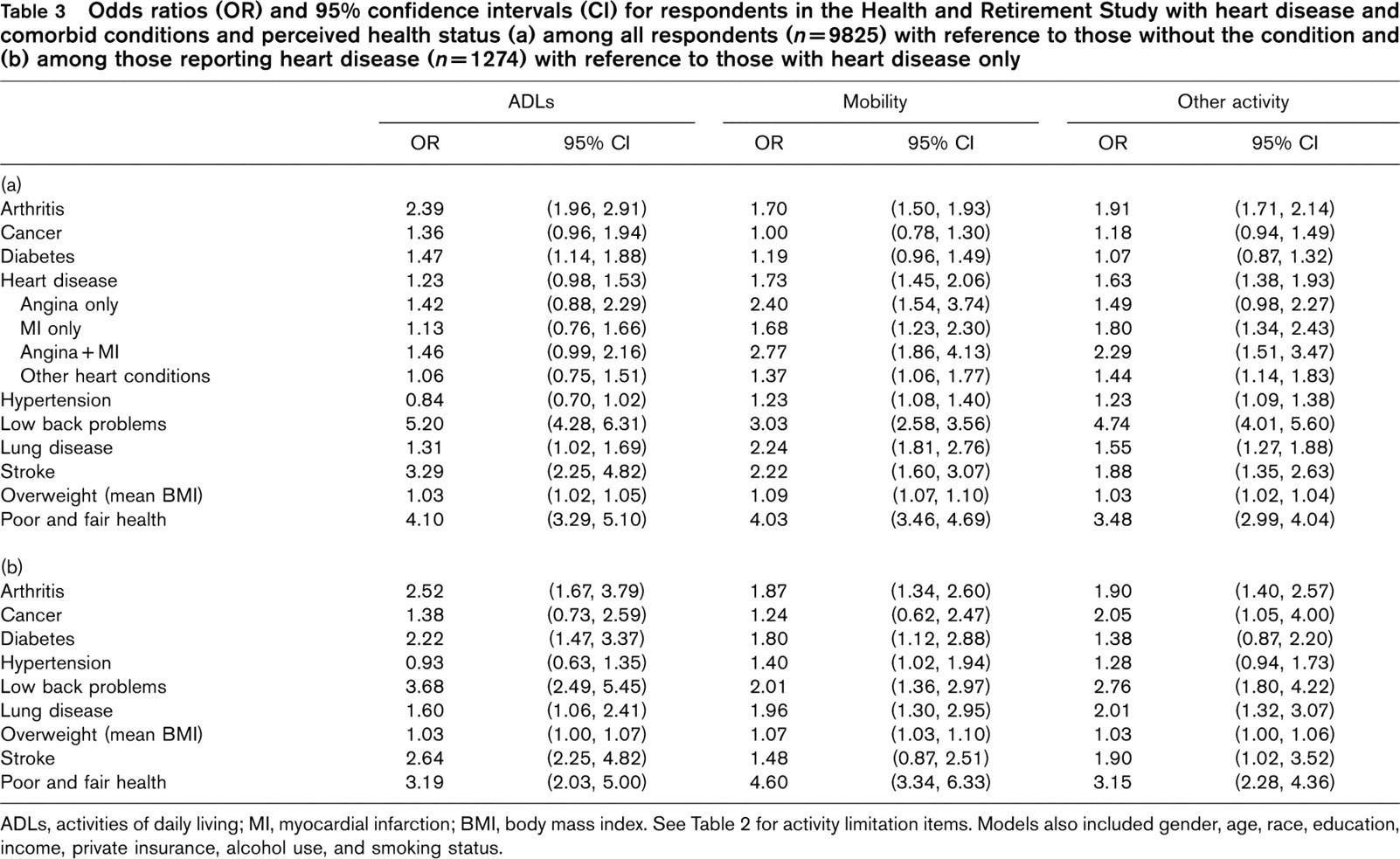
ADLs, activities of daily living; MI, myocardial infarction; BMI, body mass index. See Table 2 for activity limitation items. Models also included gender, age, race, education, income, private insurance, alcohol use, and smoking status.
Odds ratios (OR) and 95% confidence intervals (CI) for respondents in the Assets and Health Dynamics of the Oldest Old study with heart disease and comorbid conditions and perceived health status (a) among all respondents (n = 7447) with reference to those without the condition and (b) among those reporting heart disease (n = 2352) with reference to those heart disease only
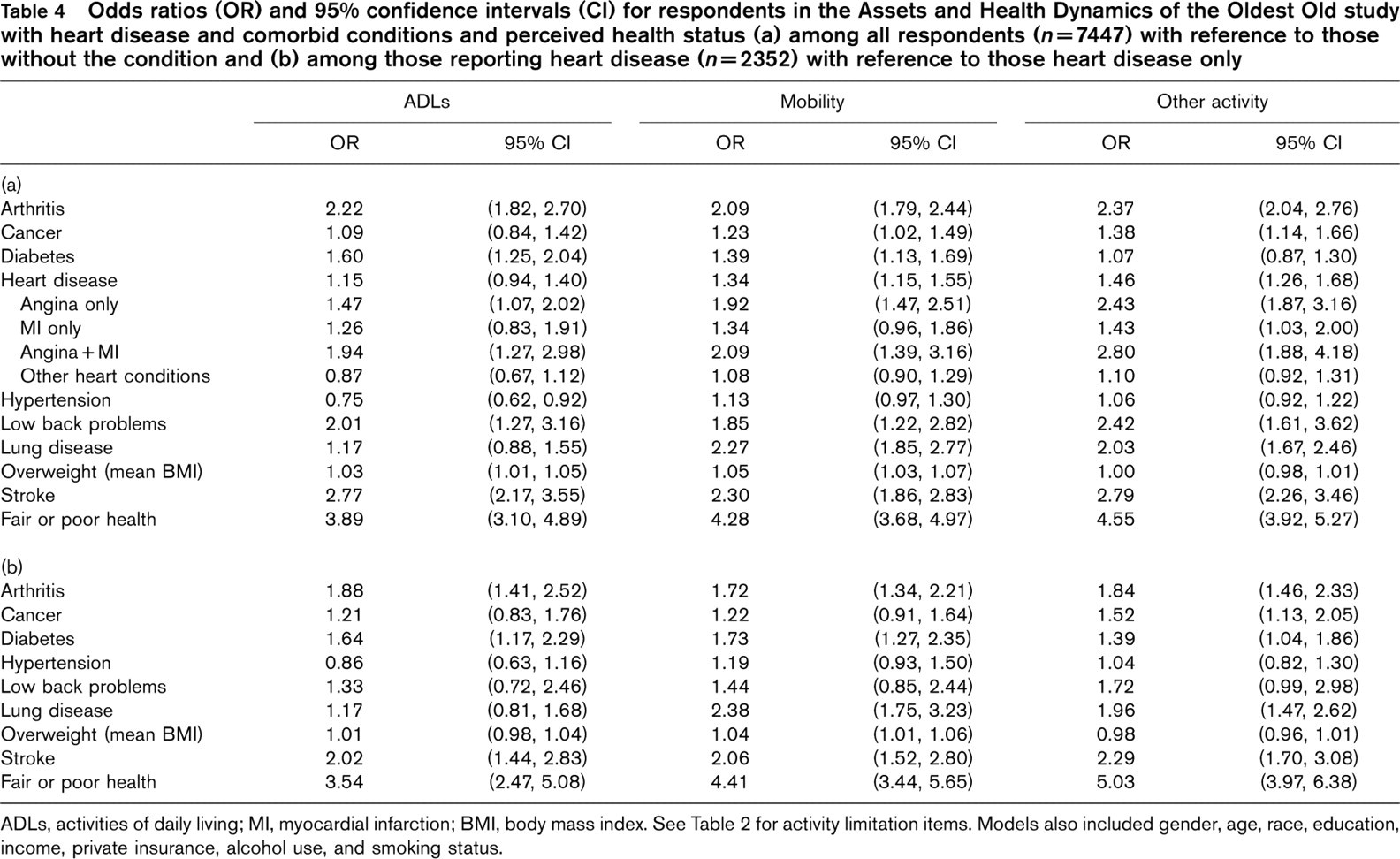
ADLs, activities of daily living; MI, myocardial infarction; BMI, body mass index. See Table 2 for activity limitation items. Models also included gender, age, race, education, income, private insurance, alcohol use, and smoking status.
Discussion
Activity limitation prevalence increased significantly across the spectrum of activity limitation categories from activities of daily living to mobility to other activities among both the 9825 middle-age (51 to 61 years) respondents in the 1992 Health and Retirement Survey and the 7447 older respondents (70 years and over) in the 1993 Assets and Health Dynamics of the Oldest Old study. Significantly more respondents with self-report heart disease than those without heart disease had an increased likelihood of activity limitation in both surveys. Among the respondents with heart disease (>12% of HRS respondents between 51 and 61 years of age and > 31% of AHEAD respondents 70 years of age and older), the likelihood of self-report activity limitation was always greater among those who reported either angina or angina plus MI than in those who reported MI only or other heart conditions. These observations substantiate an earlier report from the Framingham study [10] and a recent report from the UK [26] and reinforce the relationship between heart disease and activity limitation. It is clear from the results of this study that the impact of comorbidity on activity limitation in older community-dwelling persons with heart disease is considerable in both age cohorts.
A majority of each of the comorbid conditions examined is associated with a significantly increased likelihood of ADL, mobility, and other activities limitation among the HRS respondents. This is also true for a significantly increased likelihood of activity limitation in both mobility and other activities among the AHEAD respondents. The likelihood of activity limitation in someone 51 to 61 years of age with heart disease plus, for example, comorbid low back pain is 2.01 for mobility and 2.76 for other activities compared to a similar-aged individual with heart disease only; in persons 70 years and older with heart disease plus lung disease, the likelihood of mobility and other activity limitations in 2.38 and 1.96 respectively. Thus, patients with heart disease and other comorbidities may be at increased risk for activity limitations and perhaps loss of independence and it is likely that many of the respondents with heart disease and activity-limiting comorbidities in these two cohorts would not have been considered eligible for cardiac rehabilitation. But when the comorbidity is fully recognized and the exercise prescription is appropriately modified, the presence of activity limitation may be associated with a greater potential for benefit with rehabilitation than with no activity limitation and referral to exercise-based cardiac rehabilitation should be encouraged. It has been suggested that physicians may hesitate to refer elderly patients to cardiac rehabilitation [5] and the relatively low referral rates to cardiac rehabilitation may reflect this concern. The referral rate of eligible patients of all ages to cardiac rehabilitation programs is estimated to be < 20% among the > 12 million persons with established coronary heart disease in the USA [27,28] although encouragingly it is reported to be > 40% according to more recent EuroAspire data [29]. Even in randomized trials of treatment of heart disease where the investigational treatment regimen included referral to cardiac rehabilitation, the referral rate was reported to be only 38% [30]. The associations between heart disease, comorbidity, and activity limitations in older persons demonstrated in this study have been inadequately addressed in the cardiac rehabilitation literature and this may well be an important but unsubstantiated factor limiting referral to outpatient cardiac rehabilitation.
Outpatient exercise-based cardiac rehabilitation has been shown to be associated with improved health outcomes including a reduction in activity limitations [6,31]. Therefore, older patients, even with activity-limiting comorbidities, should be considered for referral to outpatient cardiac rehabilitation programs and encouraged to participate when appropriate. This reinforces both the observation that age is a poor proxy for disease and activity limitation and the importance of a careful evaluation of functional status by the referring physician in addition to the routine cardiovascular assessment of persons with heart disease suggesting consultation with a physiatrist, geriatrician, or occupational therapist. It also suggests that careful consideration be given to the provision of transportation in order to combine clinic and home rehabilitation with visits from a visiting clinician such as nurse or physical or occupational therapist [4]. As the cardiac rehabilitation literature has tended to focus on the single disease and age of patient approach, the cardiac rehabilitation professional may have concerns about how to respond to a new matrix of risk stratification. As the development of the exercise prescription may well be dictated by factors other than the underlying heart disease, the implications that other activity-limiting comorbidities bring to the development of the exercise prescription and the rehabilitation program must be recognized. For example, when someone with a MI and painful arthritis of the knee is referred to cardiac rehabilitation, the exercise prescription probably initially will be driven by the arthritis pain with an objective of reducing activity limitation rather than a heart rate calculated to improve aerobic condition.
Ades and colleagues have reported a strong association between activity limitation and a range of patient-reported depression scores from clinically depressed to not depressed in patients with heart disease suggesting that mood state plays an independent role in activity limitation [32]. There is an increasing recognition that one of the more important developments in health care outcome evaluation in the past two decades may be the importance of the patient's perspective when assessing treatment outcome [33,34] as well as when making recommendations about therapy [35]. In both cohorts in this study, the highest likelihood for five of the six activity limitation categories was associated with poor or fair perceived health among respondents with heart disease. A possible explanation for this strong association between perceived health status and activity limitation observed in this study is that perception of poor or fair health is a proxy summary of the respondent's perception of his or her spectrum of illness severity, any associated dysfunction, and external support.
A limitation of this study is the lack of published data demonstrating that comorbidities are a major reason for non-referral of patients with heart disease and comorbidity-associated activity limitations to cardiac rehabilitation. Activity-limiting comorbidity may be a reason for some clinicians to decide not to consider referring older patients with activity limitations to cardiac rehabilitation. If so, the strong associations between poor self-report health status, comorbid conditions, and increased activity limitation together with the potential for improvement of the activity limitation with exercise-training cardiac rehabilitation should encourage referral of appropriate patients to cardiac rehabilitation programs where the importance of comorbidities in the development of the exercise prescription is recognized by the cardiac rehabilitation professional. The impact of comorbidity and perceived health on activity limitation among otherwise similar-looking older respondents with heart disease in this study strongly reinforces the need for research investigating the real-world spectrum of comorbidity and activity limitation among persons with heart disease and the potential benefits associated with outpatient exercise-based cardiac rehabilitation.
Footnotes
Acknowledgements
We would like to acknowledge the comments from Chris Callahan, Bill Haskell, Michael Jelinek, and Terry Kavanagh and recognize their insights which have made this manuscript more relevant to those who refer patients to cardiac rehabilitation and to those who manage the programs.