
Abstract
Objective
Preventing cardiovascular events with lipid-lowering drugs has been established in several trials reported since 1994. Consequently national guidelines recommend statins for those with established cardiovascular disease (CVD) and those at high risk of developing CVD. We evaluated blood lipid levels, and compare treatment and control of dyslipidaemia in English and Scottish adults with national recommendations for lipid lowering.
Design and methods
In 1998 the nationally-representative Health Survey for England and the Scottish Health Survey included valid cholesterol results for 9631 (England) and 6065 (Scotland) adults aged 16–74. Mean blood levels of total, high-density lipoproteins (HDL-), and total: HDL-cholesterol ratio; prevalence of elevated total cholesterol levels, and total: HDL-cholesterol ratios; prevalence of use of lipid-lowering agents in high risk subgroups; and lipid levels of those on treatment were calculated.
Results
Levels of dyslipidaemia, treatment and control were not significantly different between Scotland and England. Combining these data, mean total cholesterol levels were 5.43 and 5.48mmol/l in men and women respectively; and mean HDL-cholesterol levels were 1.29 and 1.56 mmol/l. Overall 64.6% of adults had a total cholesterol ≥ 5 mmol/l, 24.6% had a total: HDL ratio ≥ 5 and 2.3% reported taking lipid-lowering drugs. Treatment rates among those with a total cholesterol > 5 mmol/l and a history of coronary heart disease or stroke, hypertension, or diabetes, were 27.3%, 15.4% and 17.8% respectively, and control rates (total cholesterol < 5 mmol/l) among those treated were 45.3%, 38.5% and 32.7%. Conclusions Low treatment rates with lipid-lowering drugs existed overall, among high-risk patients suitable for primary prevention, and among those with established cardiovascular disease.
Introduction
National guidelines recommend statins for those with established ischaemic vascular disease and those at high risk of developing it. Prevention of cardiovascular events by lipid-lowering drugs has been established by several trials reported since 1994 [1–9. Using data from the Health Survey for England (HSE) in 1998, we previously described levels of blood lipids, dyslipidaemia, and the limited use of lipid-lowering agents among a nationally representative sample of English adults [10]. Data from the second Scottish Health Survey [11] (SHS) which was also carried out in 1998 allows a comparison of the lipid related variables between England and Scotland, which has even higher coronary heart disease mortality rates than England [12].
Combining these datasets allows a more robust assessment of the contemporary use of lipid-lowering treatment in patients with established cardiovascular disease and in various subgroups of adults at increased risk of coronary heart disease due to hypertension or diabetes.
Methods
The HSE, an annual nationwide household survey, has been described in detail elsewhere [13]. Briefly, members of a stratified random sample (drawn from the Postcode Address File), socio-demographically representative of the English population are invited to participate. The annual household response rate is around 78% overall, but slightly lower in men and in inner cities. The focus of the investigation varies each year and in 1998 it was cardiovascular disease. Data are collected at two home visits: the first visit is by an interviewer who measures height and weight and administers a questionnaire, the second is by a nurse who records prescribed medicine use, measures blood pressure and draws a blood sample, among other investigations.
To date only two SHS's have taken place, in 1995 [14] and 1998 [11]. The design and response rate of the SHS is almost identical to the HSE, but the adult population sample was truncated at age 74 in 1998. The focus of the SHS in 1998 was cardiovascular disease and the same questionnaire and central laboratory was used as in the HSE.
Ethical approval for the HSE and the SHS was obtained from the relevant Multi-Centre Research Ethics Committee (North Thames and Scotland).
Smoking habits and any history of cardiovascular events and diabetes were recorded in the questionnaire. Informants who reported a history of angina or myocardial infarction diagnosed by a doctor were classified as having coronary heart disease. Total and high-density lipoprotein (HDL)-cholesterol were measured from a non-fasting blood sample using standard methods [15] at a certified central laboratory.
The most recent UK guidelines on lipid-lowering therapy for primary prevention recommend treating those whose 10-year coronary heart disease risk is 30% or greater [16]. To estimate 10-year coronary heart disease risk for this report, the Framingham-based risk equation was applied [17]. This equation has been shown to be acceptably accurate in Northern European countries [18] and includes: age, sex, smoking, systolic blood pressure, total and HDL-cholesterol, and diabetes. The equation was applied to persons aged 300–70 years, the range for which primary prevention risk assessment is recommended, and above which, prior to the Heart Protection Study [8] and the PROSPER trial [9] evidence on lipid-lowering drugs was limited.
Results
In the 1998 HSE, 13,586 adults (≥ 16 years) saw a nurse. Of the 13,586, a total of 10,569 (77.8%) also agreed to have their cholesterol measured and had their blood analysed and of these, 9631 were aged 16–74. In the 1998 SHS of the 7455 adults aged 16–74 who saw a nurse, 6065 also had a valid cholesterol measurement. All analyses were carried out separately for the HSE and SHS database, using SPSS version 10.1. Very small, nonsignificant differences between Scotland and England emerged when the data were compared, and so data are presented for the combined group.
Most analyses hereafter therefore relate to the 15,696 people aged 16–74 with a cholesterol measurement of whom 7713 were men (mean age 44.1; SE 0.17) and 7983 were women (mean age 44.6; SE 0.17).
Mean total cholesterol levels rose with age, continuously among women and until the ages of 54 in men (Fig. 1). Total cholesterol levels were higher among men than women from age 25–54 but not outside this range. High-density lipoprotein (HDL)-cholesterol levels were higher and mean total to HDL-cholesterol ratios (total: HDL) were lower in women than in men at all ages. Of those studied including the 355 patients on lipid-lowering therapy, 3.3%, 18.4% and 64.6% had total cholesterol levels of ≥ 7.8 mmol/l, ≥ 6.5 mmol/l and ≥ 5mmol/l respectively (Table 1). Among men, the highest proportions above all three cut-points were found among those aged 45–64, whereas among women the highest proportions were found in the oldest age group (Table 1). Similarly the proportion with a total: HDL ratio ≥ 5 including those on lipid-lowering drugs increased with age among women but not men and was always higher among men than women (Table 1). Overall 2.3% of adults reported using lipid-lowering drugs with age-related treatment rates reflecting age-related adverse lipid levels.
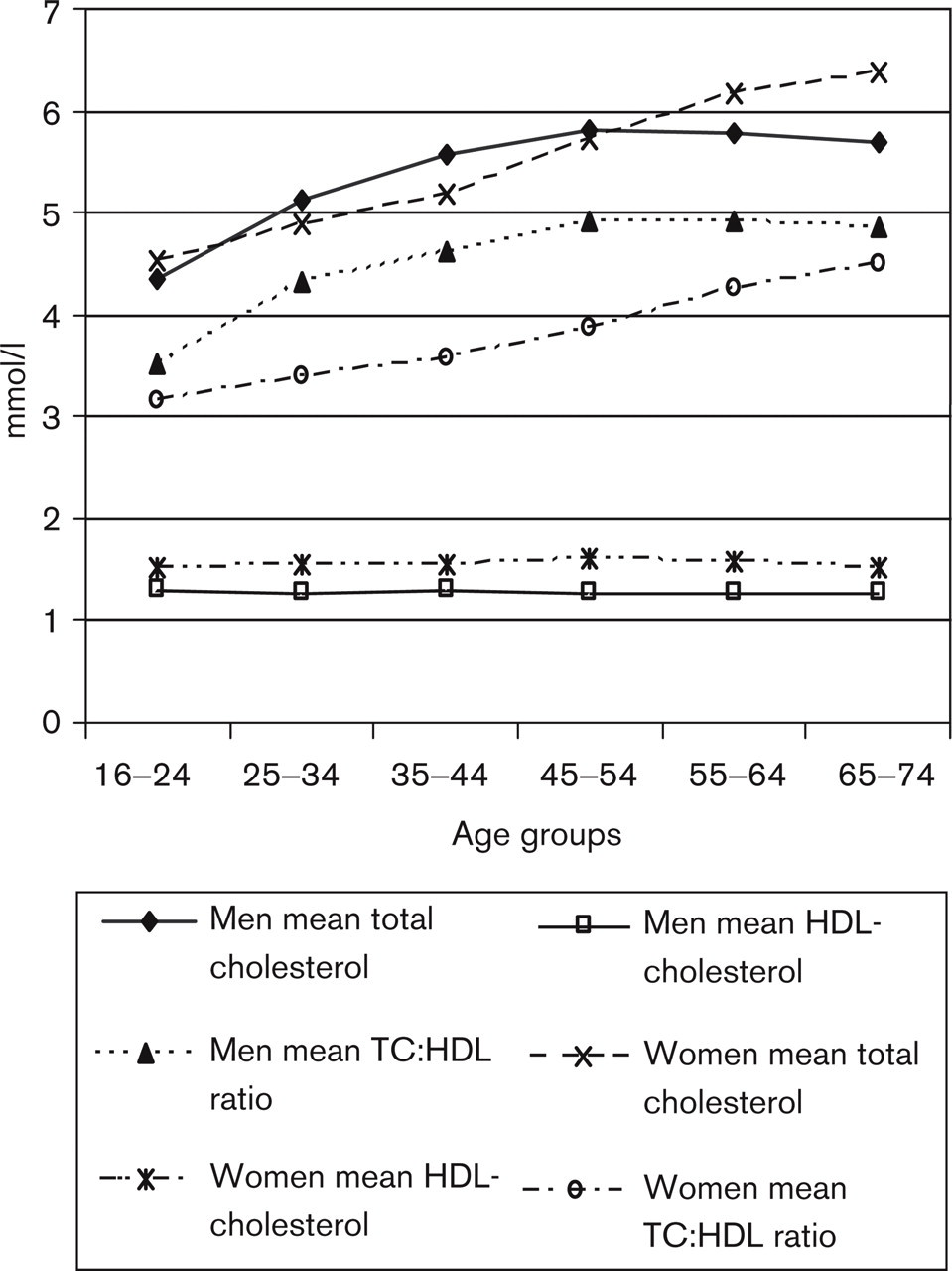
England and Scotland 1988. Total and HDL-cholesterol and total to HDL-cholesterol ratios by sex and age groups.
England and Scotland 1998. Prevalence of dyslipidaemia according to different definitions, and percentage on treatment

England and Scotland 1998. Lipid-lowering treatment and control rates in dyslipidaemic adults
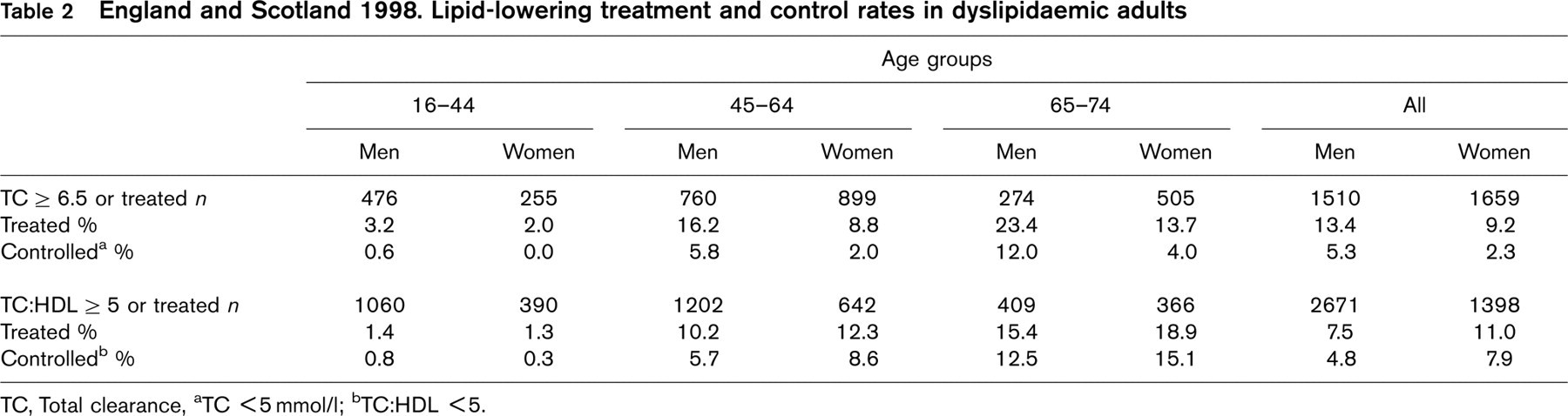
TC, Total clearance, aTC < 5mmol/l; bTC:HDL < 5.
Of those with total cholesterol levels ≥ 6.5 mmol/l or on lipid-lowering drugs, 13.4% of men and 9.2% of women were taking lipid-lowering drugs, with only 5.3% of men and 2.3% of women having their total cholesterol ‘controlled’ to < 5.0 mmol/l (Table 2). Hence 39.6% and 24.8% respectively of those on treatment reached this currently recommended target. Treatment and control rates increased with age. Of the 4069 adults with a total: HDL ratio < 5, or on lipid-lowering drugs, 7.5% of men and 11.0% of women were taking lipid-lowering drugs and 4.8% of men and 7.9% of women had their ratios ‘controlled’ to a total: HDL ratio < 5. Treatment and control rates increased with age.
Among the 11,261 adults aged 30–70 who reported no history of coronary heart disease or stroke, 10,115 (90%) had provided sufficient data to calculate a 10-year coronary heart disease risk. Of them, 168 men and 18 women had a 10-year risk of ≥ 30%. Of these 186 men and women, five men and two women were on lipid-lowering treatment and only one had his total cholesterol level lowered to < 5 mmol/l. Of the remaining 179 untreated adults only 10 (5.6%) had a total cholesterol level < 5mmol/l.
A history of coronary heart disease or stroke was reported by 866 participants (746 had coronary heart disease, 120 had a stroke) (Table 3). Of these adults, the majority, 735 people (84.9%), had a total cholesterol level > 5 mmol/l or were on treatment. Of these people, 29.6% of men and 24.1% of women were on treatment. Control rates (total cholesterol <5mmol/l) were 15.0% and 8.6% in men and women, respectively. Hence of those on treatment 50.8% and 35.6% respectively had a total cholesterol level of < 5 mmol/l. The highest treatment and control rates were observed in the 45–64 year age range.
In the whole population 1695 participants were receiving treatment for hypertension (Table 4), as ascertained by the nurse. Of these adults, the majority-1445 people (85.3%)-had a total cholesterol of > 5 mmol/l or were on lipid-lowering treatment. Of these people, 19.0% of men and 11.9% of women were on treatment. Control rates among those on lipid-lowering treatment (total cholesterol <5mmol/l) were 45.5% and 31.5% in men and women, respectively.
A diagnosis of diabetes was reported by 375 people (Table 5); of them 291 people (77.6%) had a total cholesterol of > 5 mmol/l or were on treatment. Of these people, 17.9% of men and 17.7% of women were on treatment. Control rates (total cholesterol < 5 mmol/l) among those treated were 36.7% in men and 27.3% in women.
England and Scotland 1998. Lipid-lowering treatment and control rates among those with CHD or stroke

TC, Total clearance, aTC < 5 mmol/l; ∗among those with TC > 5 mmol/l or on treatment.
England and Scotland 1998. Lipid-lowering treatment and control rates among those treated for hypertension
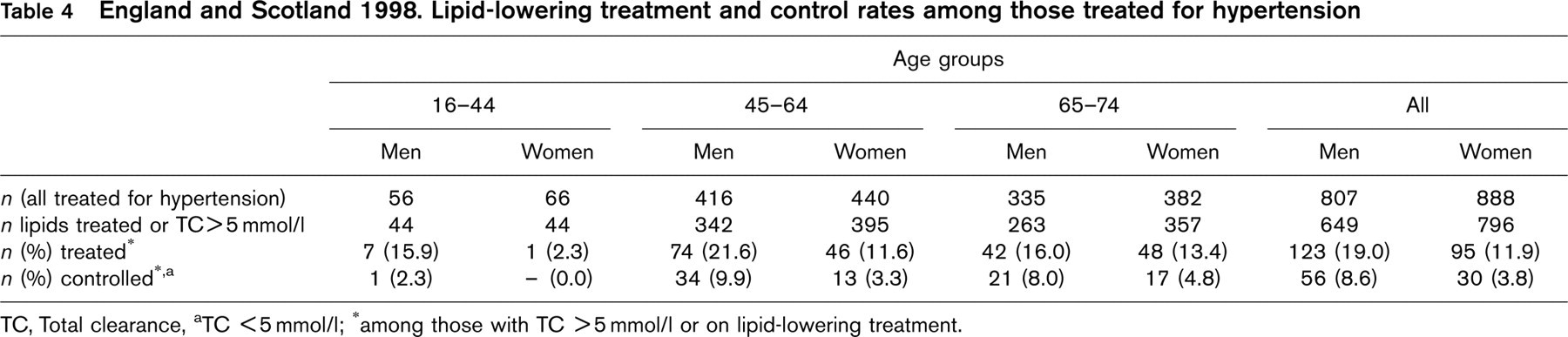
TC, Total clearance, aTC < 5 mmol/l; ∗among those with TC > 5 mmol/l or on lipid-lowering treatment.
England and Scotland 1998. Lipid-lowering treatment and control rates among those with diabetes

TC, Total clearance, aTC < 5 mmol/l; ∗among those with TC > 5 mmol/l or on treatment.
Discussion
From data on 1998 lipid levels, treatment and control rates among adults in England and Scotland were very similar. The combined database confirmed that the majority of adults had a total cholesterol of > 5 mmol/l and only 2.3% of adults were taking lipid-lowering therapy in the face of two of the highest national rates of CHD mortality and morbidity in the world [12]. The mean total to HDL-cholesterol ratio was 4.57 (SE 0.02) but was lower in men than women across the whole age range evaluated.
Guidelines for primary prevention in the UK recommend use of statins for those whose estimated 10-year coronary heart disease risk is ≥ 30% [16]. Among those aged 30–70 with no history of CHD or stroke, less than 2% of the population had an estimated 10-year CHD risk of ≥ 30%—although this may constitute an underestimate (from these data it is not possible to fully identify those who may have been at higher risk before treatment was undertaken). Only seven of these 186 adults were on treatment.
A minority (30% of men and 24% of women) of those with a history of CHD or stroke were taking lipid-lowering treatment and less than half of these had their cholesterols lowered to the current UK target of <5mmo/l [19].
In view of the high CHD event rates among patients with diabetes [20] and the high case fatality rates among diabetic subjects who suffer an acute myocardial infarction, [21] it has been recommended in recent American guidelines that patients with type II diabetes should be considered as ‘CHD risk equivalents’ and as such should be treated for secondary prevention [22]. Whilst this recommendation is controversial [23] it does seem reasonable that at least among those patients with a history of type II diabetes of 10 years or more, or those diabetic patients over the age of 50, cholesterol lowering should be seriously considered. We have shown that as of 1998 less than one in five diabetic adults were on lipid-lowering treatment in England and Scotland, and only about one third of those on treatment had their cholesterol lowered to < 5 mmol/l.
Among subjects with hypertension and a total cholesterol of > 5 mmol/l, the use of lipid-lowering therapy was even less common with only 19% of men and 12% of women on treatment. Whilst lipid-lowering is only currently recommended for those with an estimated 10-year CHD risk of 30% or more, in light of increasing evidence this risk threshold is likely to fall dramatically.
In summary, in 1998 the high rates of abnormal lipid levels and the low use rates of lipid-lowering agents were similar in England and Scotland-two countries that have some of the highest rates of CHD mortality in the world [12]. It is likely that improvements in the management of dyslipidaemia noted between 1994 and 1998 [10] have continued, as reflected by the increasing sales of lipid-lowering agents at a rate of 25–30% per year [24]. However increasing recent trial evidence [6–9 reaffirms earlier trial evidence [1–5 of the benefits of the use of statins in a wide range of patients in primary and secondary prevention. In light of these data it seems likely that recommended thresholds and targets for lipid management in the UK are likely to become more aggressive, in keeping with other international guidance [22]. The likely impact of increasing lipid-lowering drug therapy in line with current guidance for secondary prevention [19] would be expected to save around 11,000 deaths from circulatory disease in one year in England and Scotland.
Whilst the cost implications of such an increase in the use of lipid-lowering therapy are real and large—so too are the likely benefits.
Footnotes
Acknowledgements
The 1998 Health Survey for England and the 1998 Scottish Health Survey were carried out by the Joint Health Survey Unit of National Centre for Social Research (formerly SCPR) and Department of Epidemiology and Public Health at University College London. Bristol Myers-Squibb supplied an unconditional grant towards the cost of some of these analyses.