
Abstract
Aims
To compare health effects and risk reduction in two different strategies of nutritional counselling in primary health care for patients at high risk of ischaemic heart disease.
Methods
In a cluster-randomized trial 60 general practitioners (GPs) in the Copenhagen County were randomized to give nutritional counselling or to refer patients to a dietician. Patients were included after opportunistically screening (n = 503 patients), and received nutritional counselling by GP or dietician over 12 months. Health effects were measured by changes in weight, waist circumference and blood lipids. Risk of cardiovascular disease was calculated by The Copenhagen Risk Score. Data on use of medicine and primary health care was obtained from central registers.
Results
Altogether 339 (67%) patients completed the intervention. Weight loss was larger in the dietician group (mean 4.5 kg vs. 2.4kg), and increase of HDL-cholesterol was larger in the GP group (mean 0.13mmol/l vs. 0.03mmol/l). The reduction of the cardiovascular risk score was significantly larger in the GP group (P = 0.0005). Other health outcomes were not significantly different.
Conclusions
GPs were aware of substantial risk factors of cardiovascular disease and addressed these when counselling. The guidance from a GP was of significant importance for risk reduction in relation to IHD. However, a long-term lifestyle intervention by GP was difficult to implement. In the case of obesity it was effective to refer to long-term nutritional counselling by a dietician.
Introduction
Ischaemic heart disease (IHD) is still a main contributor to morbidity and mortality in most European countries [1, 2]. Risk factor modifications have been shown to reduce morbidity and mortality [3]. One of the modifiable risk factors for IHD is inappropriate diet, leading to an unfavourable lipid profile, high blood pressure and obesity [4]. Nutritional counselling for patients at risk of ischaemic heart disease is suggested prior to the initiation of medical treatment [5]. A sound diet reduces risk by weight reduction, lowering of blood pressure, effects on lipids, and control of glucose [3].
Danish GPs consider nutritional counselling important but lack time and knowledge about nutrition [6]. Similar results have been found in several international studies [7, 8]. A Cochrane review compared the effect on blood cholesterol of nutritional counselling provided by GP or dietician [9]. Dieticians had better short-term results but there was no difference in long-term effects. Very few studies have tried out different strategies for nutritional counselling in a randomized design [10].
The aim of this study was, using a randomized design, to compare the effect on weight, blood lipids and cardiovascular risk for two strategies of nutritional counselling for patients with high risk of IHD in general practice. Patients were counselled by a GP or a dietician. We also analyse the applicability of the interventions.
Method
The study took place in the Copenhagen County between April 2000 and December 2001. GPs in the locality were asked to participate in the study. Because of the need for geographic proximity to the practices of the two dieticians, only GPs in a restricted area were asked. Very few declined, but we aimed mainly at GPs whom we expected to be motivated. A total of 60 general practitioners accepted to be randomized either to give nutritional counselling or to refer patients to a dietician for counselling. GPs were randomized by computer-generated random numbers. The study employed two dieticians. Each GP was supposed to include or refer 10–15 patients within five months. Criteria for inclusion were one or more of the following:
high BMI (≥ 30 kg/m2)
large waist circumference (men >102 cm, women > 88 cm)
dyslipidaemia:
total cholesterol ≥ 7 or
total cholesterol ≥ 6 mmol/l and
HDL-cholesterol <0.9 mmol/l or
triglycerides ≥ 2.5 mmol/l or
blood pressure ≥ 140/80 or
familiar disposition for IHD or CVD
type 2 diabetes
Patients were opportunistically screened for the above-mentioned risk factors for IHD and if eligible invited to participate in the study. All patients were included by their GP. After inclusion the intervention consisted of five counselling sessions over 12 months by GP or dietician. Patients were not included in the study if they were mentally ill, intellectually handicapped, pregnant, needed an interpreter or were under 18 years old. At the start of the study and halfway during the intervention period, a day of nutritional and communicational education was provided for GPs and dieticians in order to maintain the interest of the GPs. GPs were reimbursed for participation in education and for all paper work related to the study.
The intervention
Intervention by GPs consisted of the usual treatment after one day of training in motivational interviewing. Counselling consisted of general advice and delivery of commercially available written information on healthy diet. The initial counselling session was assumed to be approximately 30 min and the following sessions approximately 12 min.
Intervention by the dietician consisted of individual counselling based on indication for referral, dietary history and habitual diet routines. Counselling focused on principles of good nutrition, advice on food shopping, cooking methods, meal planning and exercise. Recommendations included restriction of total dietary energy, reduction of the fat component and/or a cholesterol-lowering diet. The initial session was assumed to be approximately 1 h and later sessions approximately 30 min. The dietician briefed the GP on the phone after 6 and 12 months. GPs as well as dieticians could see patients for weight control between counselling sessions according to requirement.
The time used for intervention differed in the two groups. However, this was accepted as the norm for a realistic approach according to usual practice for GPs as well as dieticians. We expected the counselling sessions to be different in the two groups.
Collection of data
All patients answered a questionnaire about their cohabitation status, education, occupation, self-rated health, physical activity, smoking status, use of alcohol, and dietary habits. A food-frequency questionnaire was also completed. All questionnaires reached scientifically accepted standards. At the first session height was measured. Weight, waist circumference, and blood pressure were measured at each counselling session, and the BMI was calculated. LDL- and HDL-cholesterol, total cholesterol and triglycerides were measured at inclusion and at 6 and 12 months. Consumption of prescribed medicine [defined daily dose (DDD)] was obtained from the National Register of Medicinal Products Statistics and data on the use of primary health care was obtained from a local register. The data included that gathered one year prior to the intervention and the entire intervention period of 12 months regardless of dropout time. GPs and dieticians were supposed to give questionnaires to patients who refused to participate or dropped out, but very few questionnaires were returned from the GPs.
Ethics
The Regional Ethical Committee and The Danish Data Protection Agency approved the study. Patients were informed by their GP, received written information and gave written consent.
Statistical analysis
Binary data at baseline and follow-up, as well as dropout, were analysed using Alternating Logistic Regression [11] to compensate for the cluster-randomization and con-founders. Continuous data at baseline and follow-up were analysed with linear regression in the normal distribution applying a random intercept to adjust for cluster-randomization. We have used three different methods for the analyses of health effects:
analyses in the two patient groups separately to determine effect; the analyses were adjusted exclusively for cluster-randomization;
analyses to assess change during the entire intervention period of 12 months; to adjust for the effect of dropout these analyses were repeated using the last measured value for patients who dropped out prior to completion;
analyses to model change over time using random intercept and slopes to compensate for repeated measurements and cluster-randomization. These analyses were used to assess the difference between the two groups during the course of time.
All analyses were performed as intention to treat analyses (including all patients regardless of dropout time) as well as analyses including only completers.
Health effects were measured in all patients by changes in weight, BMI, waist circumference and blood lipids. The analyses were restricted to patients with the relevant inclusion criteria. Analyses on weight change included patients with BMI ≥ 30kg/m2 (n = 369), analyses on waist circumference included patients with large waist circumference (men >102 cm, women > 88 cm, n = 464) and analyses on blood lipids included patients with dyslipidaemia (n = 234).
The risk of cardiovascular disease was estimated using the Copenhagen Risk Score (CRS) [12], which is in essence the linear predictor from a Cox regression [13] of the age of event (IHD) on a set of risk factors (sex, HDL and total cholesterol, systolic blood pressure, smoking status, BMI, diabetes status, familial predisposition and previous heart disease). CRS is by definition independent of age. CRS > 0 indicates a higher risk than a woman with BMI = 25, total cholesterol = 5 mmol/l, HDL = 1.0 mmol/l, systolic blood pressure = 140, no disposition for or previous IHD, no diabetes and nonsmoking status. CRS is connected to predictions of absolute risk of IHD within a given time period at a given age. The connection between CRS and absolute 10 years risk at the age of 60 is given by R(CRS) = 1 — (1 — R(0)) EXP(CRS) where R(0) is found from a baseline table.
Data on consumption of medicine and use of primary health care were analysed using Pearson's χ2 test. These data were available on an aggregated level only and were analysed with no adjustments. All data were managed in the SAS system and tabulated and analysed in SAS and R [14]. A 5% significance level was used.
Results
After randomization one and eight GPs dropped out in the dietician group and in the GP group, respectively (Fig. 1). In total 503 patients were included, 312 for counselling by dietician and 191 for counselling by GP. To include as many patients as possible the period of inclusion for intervention by GP had to be extended by four months. GPs referred one to 17 patients per GP to a dietician (with a mean of 11 patients), and counselled two to 29 patients (with a mean of nine patients). Altogether 339 patients (67%) completed the intervention (Fig. 1). The response rates for patient questionnaires varied from 86% to 95% in both groups. The two patient groups did not differ with regard to odds for dropout (OR12 months= 0.82; CI: 0.45–1.49, reference GP group). Age was significantly and positively associated with odds for completing the intervention (data not shown).
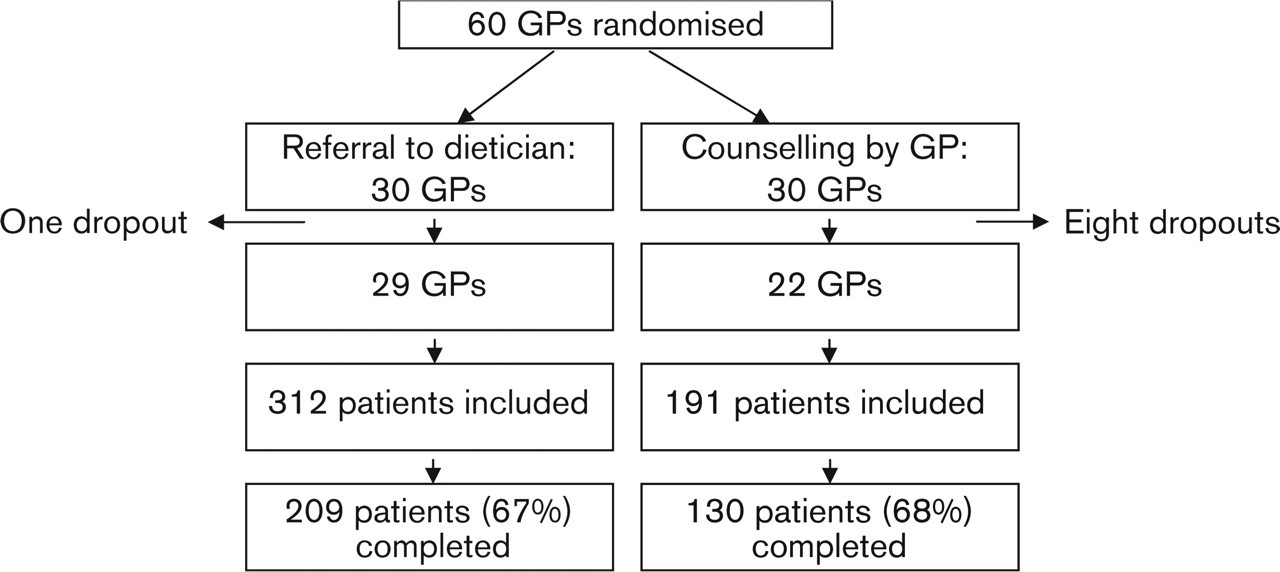
Flow chart of participation in the study.
Comparison at baseline
The baseline characteristics of the population are shown in Table 1. There were no significant differences in the two groups with regard to dietary habits, physical activity, socio-demographic variables, use of alcohol or cardiovascular risk. More patients in the dietician group had a history of dieting and attempts of weight loss. More patients in the GP group were smokers. There were no differences in motivation for changing lifestyle (data not shown).
Compared with the GP group significantly more patients in the dietician group were included with the inclusion criterion excessive waist circumference (OR = 2.8; CI: 1.5–5.6, adjusted for sex, age and cluster-randomization). Significantly fewer patients in the dietician group were included with dyslipidaemia (OR = 0.7; CI: 0.5–0.9, adjusted for sex, age and cluster-randomization).
Changes in weight and waist circumference
In intention to treat analyses both groups obtained a significant reduction of weight, waist circumference, and BMI (Table 2). Among the completers the GP group had a significantly larger weight loss than the dietician group during the first month of the intervention (P = 0.04), whereas the dietician group had a significantly larger weight loss during the rest of the intervention (P = 0.01). Intention to treat analyses showed no significant differences between the GP and the dietician group (Table 2). We found similar results in the reduction of BMI and waist circumference (Table 2).
Background and lifestyle characteristics at baseline/randomization
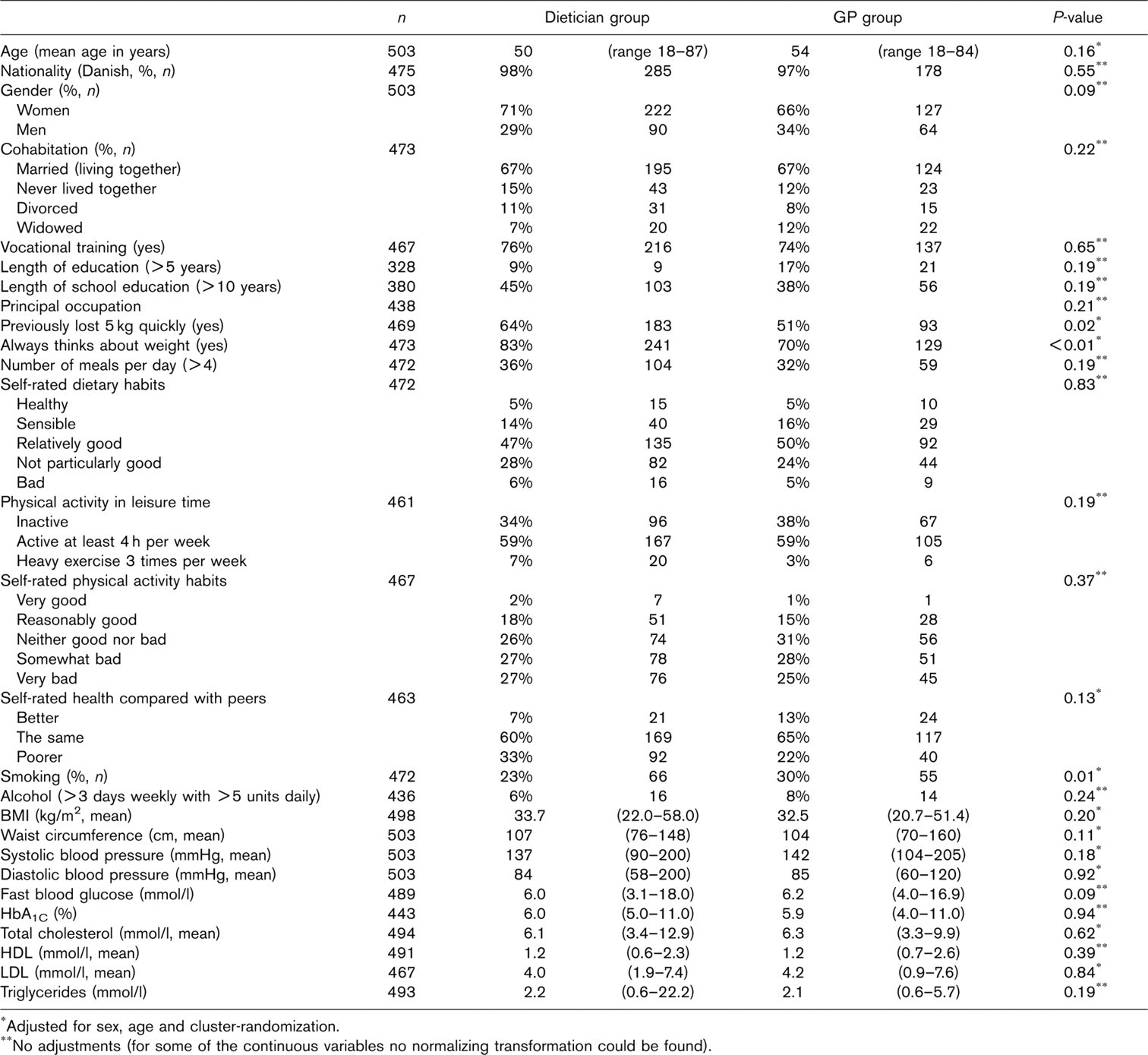
∗Adjusted for sex, age and cluster-randomization.
∗∗No adjustments (for some of the continuous variables no normalizing transformation could be found).
Changes in weight, blood lipids and absolute risk of IHD among patients counselled by GP or dietician. Analyses are performed for both ‘completers’ and according to intention to treat (sensitivity analyses). Figures are adjusted for sex, age and cluster-randomization
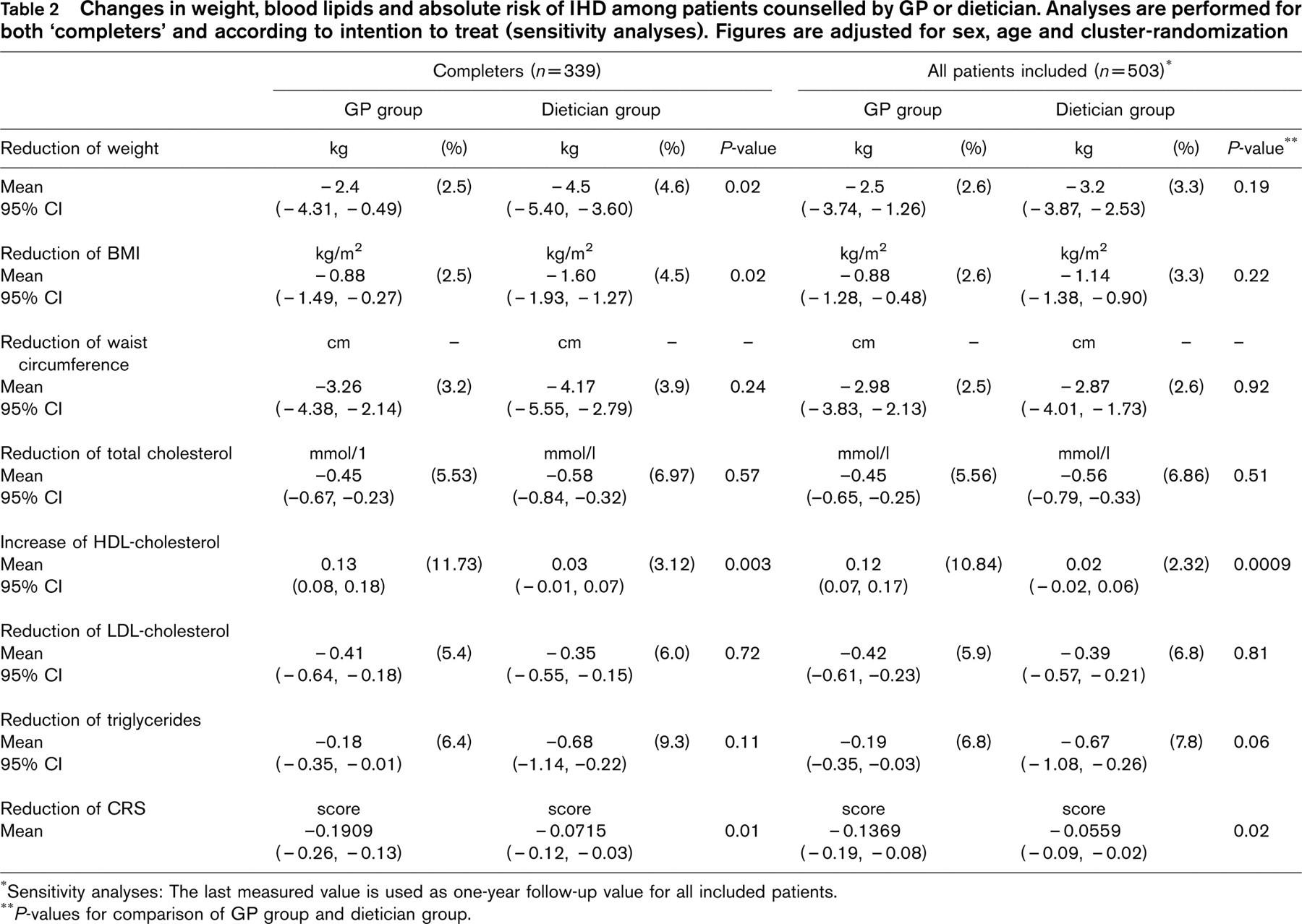
∗Sensitivity analyses: The last measured value is used as one-year follow-up value for all included patients.
∗∗P-values for comparison of GP group and dietician group.
Changes in blood lipids
Both groups obtained significant reductions of total cholesterol, LDL-cholesterol, and triglycerides. Only the GP group obtained a significant increase in HDL-cholesterol. The GP group increased HDL-cholesterol with 0.11 mmol/l more per year than the dietician group. Intention to treat analyses showed similar results. No baseline variables had significant influence on these results (Table 2). There were no other significant differences between the groups neither in analyses with patients who completed the intervention nor in sensitivity analyses with all patients.
Cardiovascular risk
There was a significant reduction in cardiovascular risk in both groups. The reduction of risk in the GP group was significantly larger than in the dietician group (Table 2). This effect is illustrated in terms of absolute 10-year risk at the age of 60 by plotting what the risk would be with the two types of intervention versus the risk without intervention (Fig. 2a). Figure 2b is a model of the median risk reduction in the two groups. On the x-axis the calculated 10 year risk of IHD at baseline is shown. The abscissa shows the risk reduction following the intervention. Patients with a low risk at baseline gained little, whereas patients with a higher risk at baseline had a larger reduction. The GP group had a significantly larger reduction and both groups obtained an effect significantly different from 0.
Consumption of medicine, self-reported changes in lifestyle and satisfaction with the intervention
Altogether 4.9% (n = 14) in the dietician group and 4.2% (n = 8) in the GP group used lipid-lowering medication prior to the intervention, which was not significantly different (P = 0.85). During the intervention 5.5% (n = 17) in the dietician group and 9.9% (n = 19) in the GP group used lipid-lowering medication (P = 0.08). During the intervention the GP group had a significantly larger increase of consumption of lipid-lowering medicine than the dietician group (P = 0.004). The two groups did not differ significantly with regard to total consumption of medicine, heart and blood pressure medicine or in use of primary health care neither before nor during the intervention (data not shown).
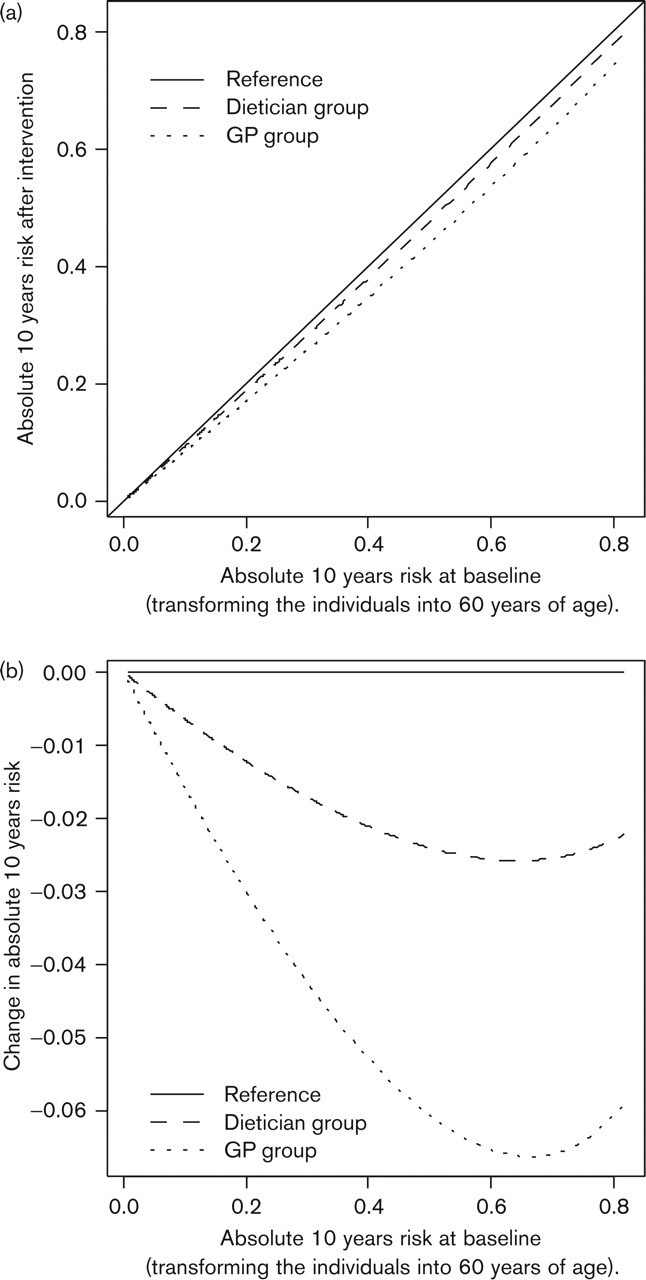
Risk reduction in the two patient groups using the Copenhagen Risk Score.
The dieticians performed the intervention throughout the intervention period with no interference needed from the investigators. Most GPs needed frequent reminders in order to counsel patients regularly, that is, at least three written reminders and for some GPs a number of telephone calls and five to 10 written reminders, especially at the end of the intervention period.
Discussion
We have tested two strategies for providing nutritional counselling in the primary care setting. Both strategies led to significant weight reduction, reduction of waist circumference and a change of the level of serum lipids. The cardiovascular risk reduction was significantly larger in the GP group, but it was very difficult to implement a 12-month intervention of nutritional counselling by a GP. Other endpoints were just slightly different in the two groups.
Both strategies have health outcomes at a level comparable to similar intervention studies [15–21. A systematic review found strong evidence that nutritional counselling provided over one year leads to a weight loss of 3–10 kg and can be provided by any health professional with nutritional knowledge [15]. The results in relation to weight loss in the present study may seem somewhat unimpressive, considering the efforts invested. It is, however, what is to be expected with this type of intervention [15] and there is no other treatment option for most of these patients in the Danish health care system.
According to studies on lipid-lowering medication, an increase of HDL-cholesterol at 6% is to be expected [22]. The intervention in this study results in an overall increase of 12%. This increase (0.01–0.13 mmol/l) is large compared with that reported in the literature (−0.16–0.08 mmol/l) [17, 19]. Reduction of total cholesterol in this study (0.3–0.8 mmol/l) is similar to or higher than reported in the literature (0–0.45 mmol/l) [17, 19–21]. Other studies show, as does the present study, that health screenings in general practice can reduce the cardiovascular risk in high-risk individuals [23, 24].
The larger increase of HDL-cholesterol in the GP group is the only significant difference between the two groups as to change of lipid profile. This difference could be partly due to a larger increase in the use of lipid-lowering medication in the GP group, but a very small number of patients were affected. The improved lipid profile and a larger increase in smoking cessation in the GP group might be the reasons for the observed improvement in risk score.
The recruitment thresholds may have been different in the two groups, which is a well-recognized design limitation of cluster trials. However, this study design illustrates the clinical world very well. It was probably harder to achieve weight loss in the dietician group, which had more previous attempts of weight loss compared with the GP group. The GPs randomized to referral to dietician may have seen this study as a new option for obese patients who had previously tried out other interventions. The GPs randomized to providing nutritional counselling may have avoided including similarly ‘difficult’ patients. Even then the dietician group achieved a significantly larger weight loss among patients who completed the intervention. Patients referred to a dietician received more time for intervention which might have affected this result. Patients in the GP group may have had more potential for improving the lipid profile since dyslipidaemia was more frequent in this group. The results should be interpreted with this possible bias in mind.
We did not find significant differences in motivation parameters in drop-outs and ‘completers'. However, it is possible that lack of motivation and/or a complex weight history could have influenced the tendency to drop out. The risk reduction was significantly larger in the GP group and the GPs seem to have focused on a diversity of risk factors including smoking although the focus of the study was nutritional counselling. So this study confirms that weight is a far less important risk factor than smoking and blood lipids in relation to cardiovascular risk. The study indicates that GPs are fully aware of the important risk factors, whereas the dieticians performed nutritional counselling strictly according to the guidelines for the study. An Australian study of nutritional counselling among obese patients in general practice found that patients counselled by a doctor as well as a dietician had a larger weight loss compared with patients counselled by a dietician alone [8].
Designing studies to evaluate GP practice is a very difficult undertaking. Although reimbursed for participating in the study GPs must be willing to participate. This is a general concern for studies such as this [25]. We do not consider our sample representative of Danish GPs in that the participating GPs were motivated and interested in the issue of nutrition, prevention and health promotion. However, the results suggest that even with highly motivated GPs effective nutritional counselling is difficult to implement in practice settings, as they are not designed to manage long-term programmes for behavioural changes. The relevant contribution of the GP seems to be to ascertain and address relevant risk factors for IHD and to motivate patients. Long-term nutritional counselling should realistically be taken care of by dieticians or other health professionals with skills in this area. The GP should attitudinally support the counselling provided.
The county in which the study took place has used the results in the decision-making process when planning preventive services in general practice. The GP patients can now - as part of the public health service - enter long-term prevention programmes lead by other health professionals employed by the GP.
Conclusion
A GP or a dietician could provide nutritional counselling in general practice with slightly different outcomes with regard to weight reduction and change in lipids. GPs more effectively obtained risk reduction in relation to risk of IHD. However, GPs needed thorough encouragement to maintain a treatment programme of 12 months. It seems relevant to suggest that the GP is responsible for addressing relevant risk factors, but in the case of obesity or other condition that requires long-term prevention the GP should have the possibility of referring to a dietician.
Footnotes
Acknowledgements
The Danish Centre of Evaluation and Health Technology Assessment and The Copenhagen County financially supported the work described in this paper.
In addition, we wish to thank all study participants, the two dieticians Annette Sejling and Inger Skovsbo, the GPs and the county officials John Sørensen, Aase Nissen, Helle Neel Jacobsen and Pernille Breum for their cooperation.