
Abstract
Background Grown-ups with congenital heart disease (GUCH) constitute an increasing population. Some of them reach adulthood without intervention and may present with symptoms, some require first intervention or re-operation for various reasons. Although interventions become more and more frequent in these patients, limited knowledge exists on their quality of life (QoL). The aim of the present study was to analyze QoL in GUCH patients who underwent cardiac surgery after the age of 14 years.
Design A total of 296 patients with a mean age of 35±16 years (range 14–72 years) were operated on at our institution between July 1987 and December 2000, mainly for atrial septal defect (ASD), outflow tract lesion, Marfan syndrome and coarctation. Early mortality was 3.4%. During follow-up QoL was assessed with the short form 36 health survey questionnaire (SF-36) and an additional questionnaire focused on medical and psychosocial aspects. Results were analyzed for the total collective and in relation to the underlying congenital heart disease (CHD).
Results Quality of life was excellent and similar to an age- and gender-matched standard population, except in patients following repair of complete AV-canal. The main restrictions in this group were found in the emotional aspect (62.5±29.9) and physical role function (60.5±25.0) and reflected in limitations of daily activity.
Conclusion Outcome and QoL in adolescents and adults with CHD is excellent and similar to that of an age- and gender-matched standard population. In the future special attention should be focused more strongly on medical follow-up and psychosocial problems in this increasing group of patients. Eur J Cardiovasc Prev Rehabil 12: 138–143 © 2005 The European Society of Cardiology
Introduction
Grown-up congenital heart patients (GUCH) represent a growing medical community, due to long-term survival after successful treatment for congenital heart disease (CHD) in early childhood. Before the advent of surgical treatment for congenital cardiac malformations, less than one-fifth of children born with such a lesion reached adulthood [1] and most of the survivors had mild lesions. This poor prognosis has been reversed, so that by the 1980s 85% could be expected to reach adulthood and today most deaths occur in adults [2]. Knowledge and training in CHD, adult cardiology and general medicine are required for practitioners in this area [3]. Cardiovascular units providing care for these patients should meet the guidelines recently published [4].
In the present study we focus on adolescents and adults with CHD, who underwent cardiac surgery after the age of 14 years, many of whom required re-operations for various reasons such as residual defects, long-term sequel, degeneration or outgrow of implants and more rarely, terminal heart failure [5]. Surgery in these patients may be challenging, because of long-standing defects, the diversity of underlying pathologies, the presence of sequel and residual defects from previous operations and the multi-organic nature of the many complex cardiac malformations associated with congenital syndromes and cyanosis [5, 6]. Beside these medical aspects however, several socio-psychological problems and impairments in quality of life (QoL) have to be addressed in this special group of patients [7, 8].
A few studies have examined the psychosocial aspects in these children and adolescents but not specifically their QoL [9, 10]. Lane and co-workers [7] were the first to assess QoL in a large group of GUCH patients by using the SF-36, showing poor results in comparison with an age- and gender-matched general population. The present study aimed at evaluating QoL and psychosocial problems in patients with CHD, having undergone cardiac surgery after the age of 14 years.
Patients and methods
Patients
Out of 296 patients undergoing cardiac surgery for CHD between July 1987 and December 2000, 233 patients were included in this study, after excluding patients with Marfan syndrome and diseases of the ascending aorta. The mean age of the total collective was 35 ± 16 years (range 14–72 years). In-hospital mortality was 3.4%. Our group has previously reported surgical data on this collective [5]. A total of 233 patients fulfilled the inclusion criteria, as patients with Marfan syndrome and patients with diseases of the ascending aorta were not subject of the present study. Average follow-up was 87 ± 54 months. During the observation period 29 patients (13.2%) were lost and nine patients (3.8%) died. Clinical follow-up was complete in all 195 patients (100%) contacted. The QoL could be assessed in 154 patients (79%), and since we referred to the German version of the SF-36, 31 (15.9%) Italian and French speaking patients were excluded, four patients (2.1%) were not able to answer the questionnaire, all of whom were suffering from additional chromosomal aberrations and six patients (3.1%) refused to answer the questionnaire. As shown in a previous study, exclusion of Italian and French speaking patients, with similar pre-operative characteristics, does not bias QoL results.
Patients were divided into five groups, according to the underlying CHD; group 1: atrial septal defect (ASD; n = 125); group 2: aortic and/or pulmonary valve diseases (n = 34); group 3: co-arctation (n = 21); group 4: cyanotic CHD (tetralogy of fallot (TOF) and transposition of the great arteries (TGA); n = 17); and group 5: complete AV-canal defect (CAVC; n = 7).
Methods
All pre-, intra- and post-operative data were assessed. Follow-up focused on survival, psychosocial problems and QoL.
The QoL was assessed with the short form health survey questionnaire (SF-36) [11, 12]. The SF-36 consists of 36 short questions mirroring health and QoL in eight different aspects: bodily pain (BP, two items); mental health (MH, five items); vitality (VT, four items); social functioning (SF, two items); general health (GH, five items); physical functioning (PF, 10 items); and role functioning, both emotional (RE, three items) and physical (RP, four items). Role functioning reflects the impact of emotional and physical disability on work and regular activity (the individual's normal everyday role). Raw points were transformed, generating a score for each dimension ranging from 0–100, with 100 reflecting best functioning. Swedish normal population (n = 8930) scores were used as a standard population for comparison (range 85–115). All the data were analyzed for the total collective, as well as for the different types of CHD (groups 1–5).
An additional disease-specific questionnaire was sent to all patients, focusing on medical follow-up, vocational training, problems with insurances and aspects of pregnancy.
Statistical analysis
Data are presented as mean values ± their first standard deviation. A Mann–Whitney U-test or χ2 test was used for between-groups comparison of continuous and nominal variables, respectively. A P-value of less than 0.05 was considered significant. The SF-36 questionnaire was analyzed in accordance with the SF-36 manual, replacing missing values using the described algorithm [11]. Scores were adjusted for sex and age in order to be comparable with normal population. Data were analyzed using the StatView 4.1 statistical package (Abacus Concepts, Berkley, California, USA).
Results
Collective
Overall QoL was fairly good and similar to an age- and gender-matched standard population, which scores between 85 and 115 (Fig. 1).
A total of 161 disease-specific questionnaires (82.6%) were correctly filled-out. Only 87 patients (54%) had a cardiological follow-up, usually once a year. Thirty-three patients (20.5%) were treated for arrhythmias, 22 (66.7%) of them being under anti-arrhythmic medication and five patients having required a pacemaker. Seventy-three children were born from 48 parents suffering from CHD, five of whom children had a CHD (6.9%). Of the 81 women who filled-out the questionnaire six (7.4%) decided against pregnancy due to their CHD. Problems with insurance were reported in 40 patients (24.8%), most of which (60%) related to the presence of the CHD (Fig. 2, Table 1).
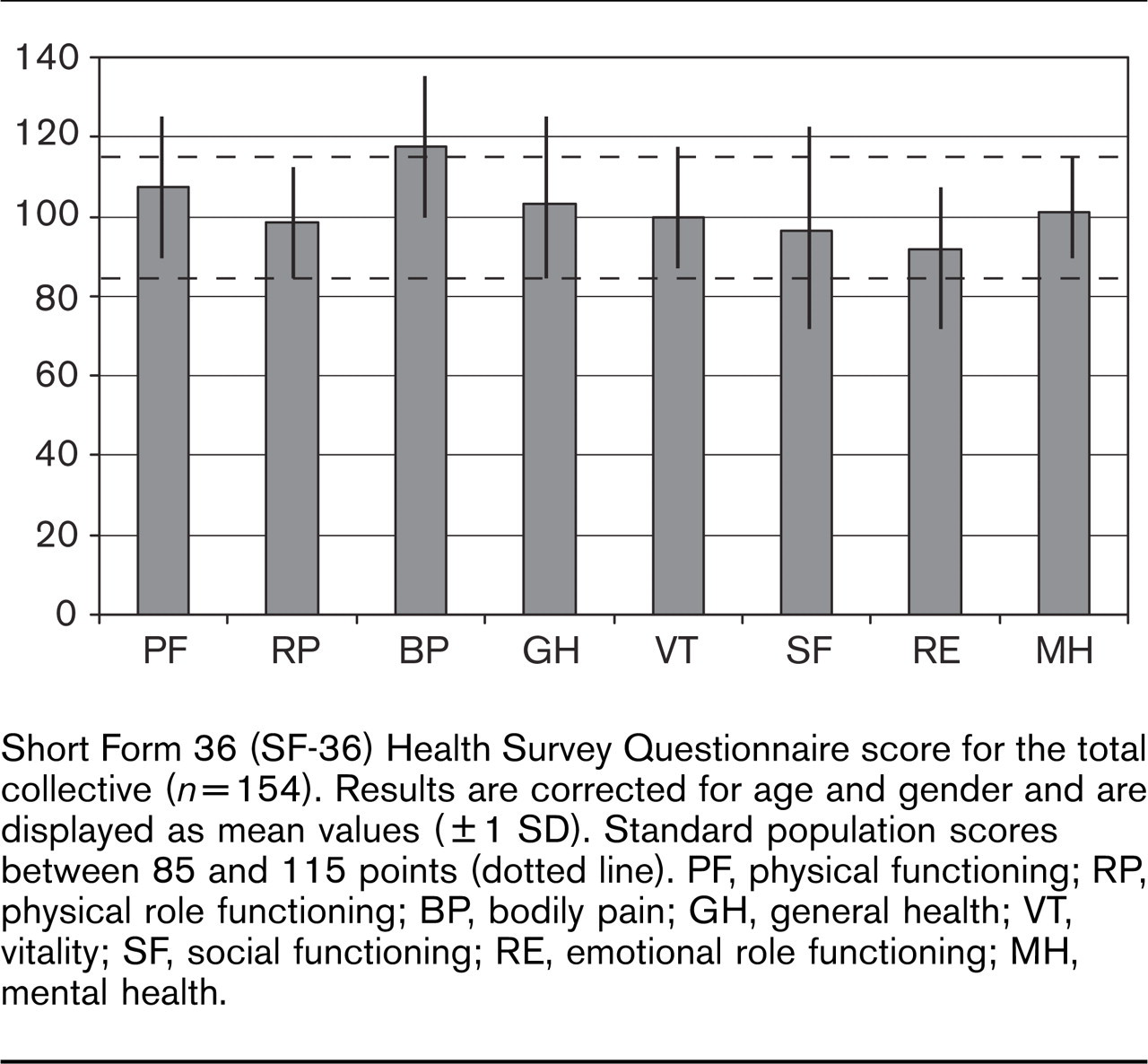
Short Form 36 (SF-36) Health Survey Questionnaire score for the total collective (n = 154). Results are corrected for age and gender and are displayed as mean values (±1 SD). Standard population scores between 85 and 115 points (dotted line). PF, physical functioning; RP, physical role functioning; BP, bodily pain; GH, general health; VT, vitality; SF, social functioning; RE, emotional role functioning; MH, mental health.
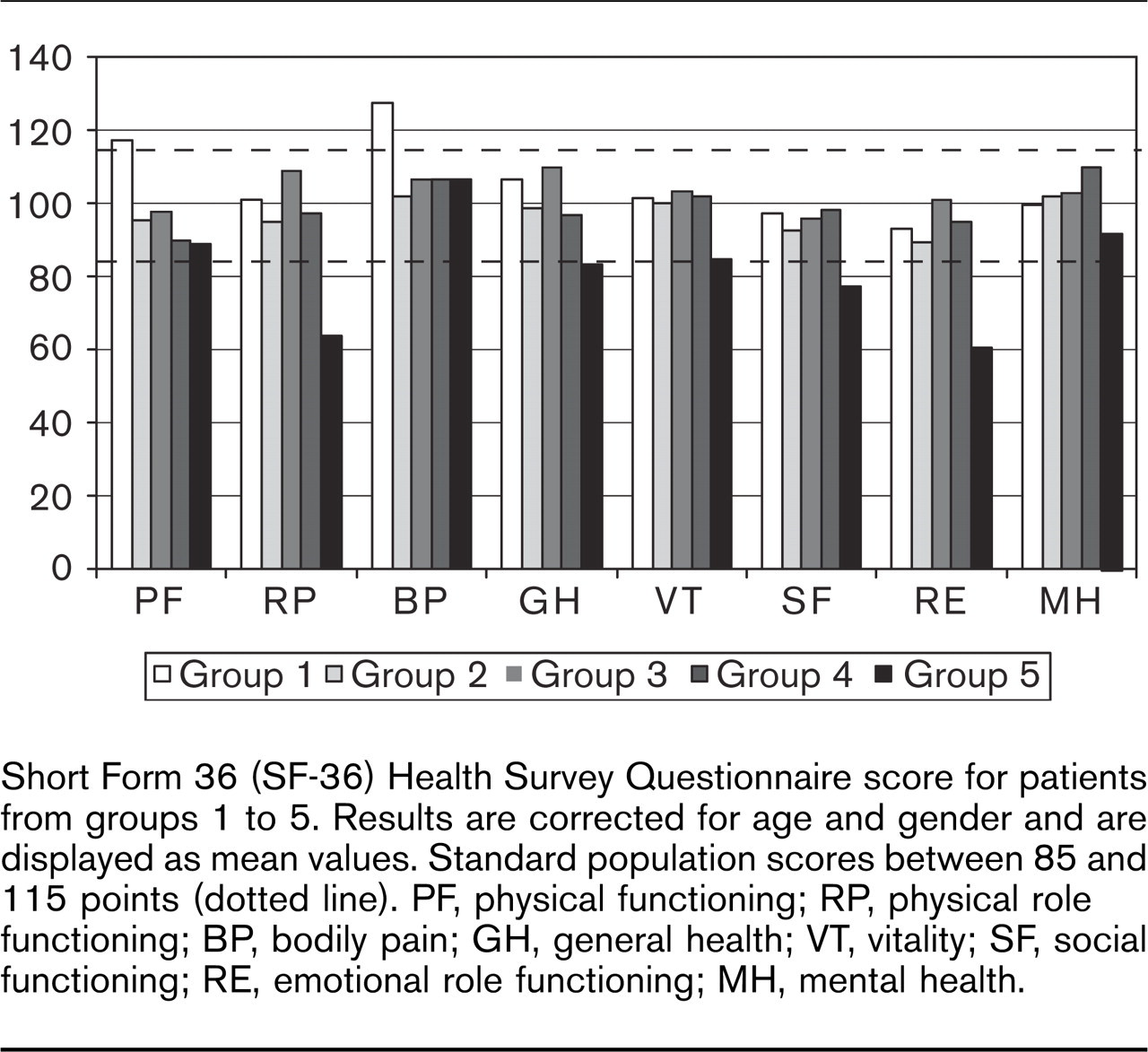
Short Form 36 (SF-36) Health Survey Questionnaire score for patients from groups 1 to 5. Results are corrected for age and gender and are displayed as mean values. Standard population scores between 85 and 115 points (dotted line). PF, physical functioning; RP, physical role functioning; BP, bodily pain; GH, general health; VT, vitality; SF, social functioning; RE, emotional role functioning; MH, mental health.
Comparison between groups
When analyzing QoL, all groups (except patients from group 5 suffering from CAVC), scored similar or even better than an age- and gender-matched standard population. Group 5 however reported poor results in two of eight aspects in the SF-36. The main restrictions in this group were found in the emotional aspect (62.5 ± 29.9) and physical role function (60.5 ± 25.0), which are reflected in a limitation of daily activity (standard population scores between 85 and 115).
A cardiologist followed most patients from groups 2, 3 and 4. Arrhythmias were frequently reported in the cyanotic group (23%). Difficulty in getting health and life insurance were mainly encountered in groups 2 (50%) and 4 (30.8%). A total of 65% of our patients answered that they do 1 h of sport at least once a week, in comparison to 58% in the standard population. Physically active patients, doing competitive sports, are mainly found in patients suffering from cyanotic CHD and valve diseases. Out of the 25 patients doing competitive sports, 13 were participating in a collective competitive sport (soccer, eight; volleyball, four; ice hockey, one) and 12 were engaged in an individual sport (tennis, six; squash, three; equitation, two; skiing, one).
Discussion
Quality of life
Quality of life in GUCH patients who underwent cardiac surgery after the age of 14 years is fairly good. We found no limitations in QoL in the total collective of GUCH-patients in comparison with an age- and gender-matched standard population. These findings are not similar to the results published by Lane [7], who described that patients with cyanotic CHD and paradoxically also patients deemed surgically cured, had significantly poorer physical functioning and overall general health perception than the general population. The explanation for this difference may be due to the aspect that Lane did not transform the raw SF-36 values, allowing an age- and gender-matched comparison and just compared the results to a standard population with an age between 30 and 34 years. This modification of the raw SF-36 values is crucial to allow comparison, as QoL is poorer in older patients and in females. We found that only in patients who had undergone a repaired CAVC were there significant impairments in emotional and physical function when compared with an age- and gender-matched standard population. However, only six patients answered the questionnaire and three of them had additional mental impairments due to chromosomal aberrations (trisomy 21), which certainly affected the results. Nevertheless patients suffering from CAVC without chromosomal aberrations scored significantly lower, compared to an age- and gender matched standard population. However, one may assume that patients suffering from complex congenital heart diseases, as well as patients who have undergone palliative cardiac surgical procedures or have been operated on many years ago may experience limitations in QoL, as reported by Kamphuis and colleagues [13]. They found limitations in the physical dimensions of health-related quality of life in 78 patients with previously operated complex congenital heart diseases.
Medical follow-up
A cardiologist followed only 54% of the patients in the total collective. This was due to the large number of patients with closure of an ASD, of which only 6% were followed by a cardiologist. However, follow-up by a cardiologist was much better in the other patients: 92% with cyanotic CHD, 89% with valve diseases, 88% with co-arctation syndrome and 83% of the patients suffering from CAVC. Usually cardiological controls take place once a year. Only 9% of the patients are followed by a University Hospital. According to the guidelines from the British Cardiac Society [4], GUCH patients should be followed by a specialist unit, which should be located in an adult medical environment, ideally with a multi-disciplinary specialist provision.
Results of the additional questionnaire for groups 1 to 5
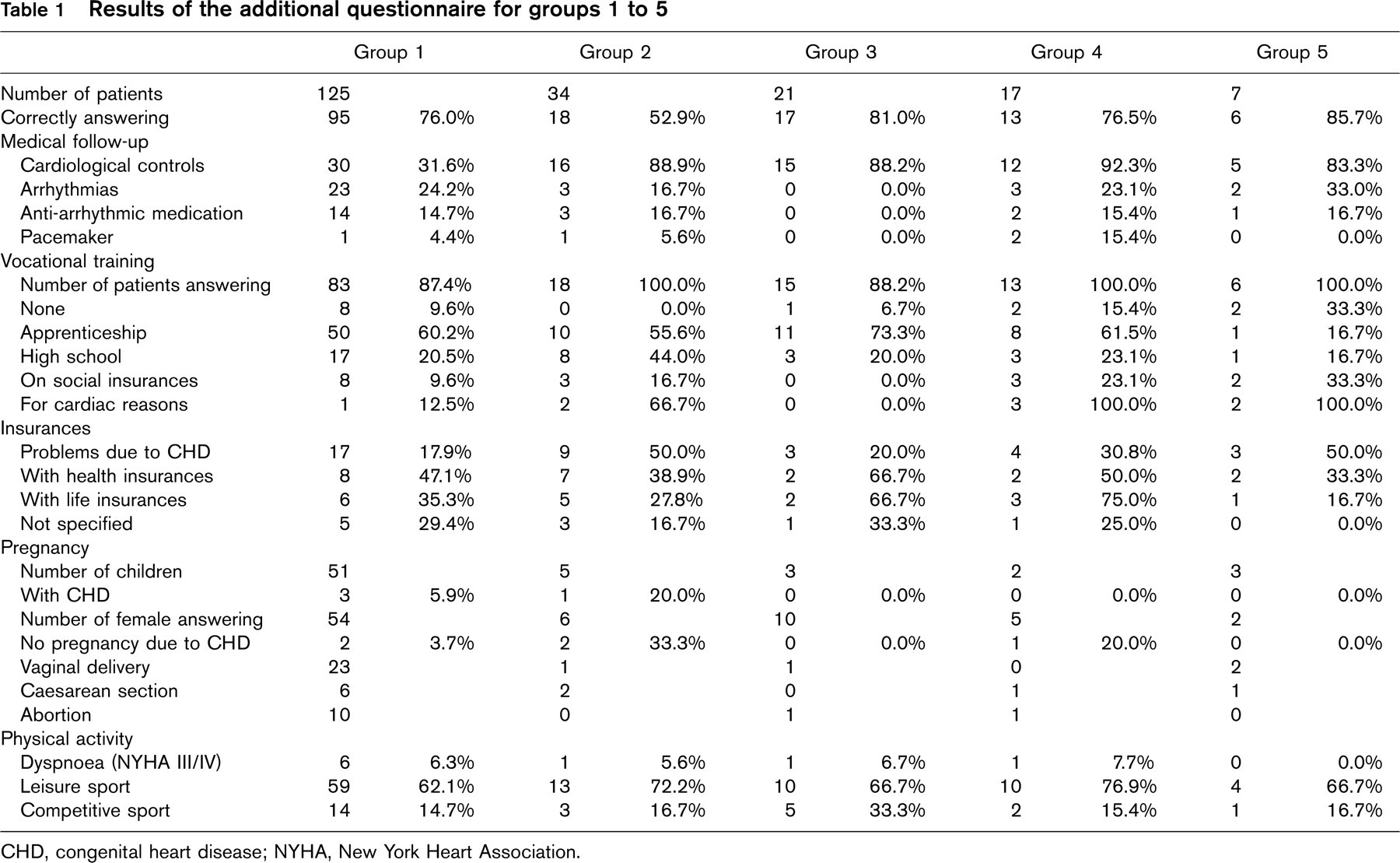
CHD, congenital heart disease; NYHA, New York Heart Association.
Twenty percent of the patients complained about arrhythmias. Arrhythmias were mainly encountered in patients suffering from CAVC (33%), in cyanotic CHD (23%) and after surgical closure of an ASD (24%). Seventy-five percent of the arrhythmias in GUCH patients were found in patients with single heart, atrial septal defect and cyanotic CHD [4, 14]. Only a few of these patients had additional investigations. No electrophysiological mapping or ablation has been performed in this collective. It is very important that whenever cardiac surgery in the GUCH patient is undertaken, the electrophysiological consequences of the defect and the operation should be considered, and surgical ablation may be appropriate. In patients with single ventricle physiology, complex cardiac malformations and cyanotic defects in particular, the onset of arrhythmias are usually an ominous sign of underlying haemodynamic deterioration, therefore aggressive assessment of these patients is currently advocated.
Vocational training
Overall vocational training in GUCH patients is quite similar in comparison with a standard population. Limitations are found in patients suffering from cyanotic CHD and from CAVC. In the CAVC-group additional non-cardiac malformations, usually due to chromosomal aberrations, are major limitations when trying to learn a profession. Of those being medically able to work only 3.7% were unemployed, which is similar to the unemployment rate of 4.2% in the Swiss population. However an additional 10.5% of the patients were on social insurances and therefore medically unable to perform a profession – the majority of these patients are found in the cyanotic group (23%) and in the group of patients suffering from CAVC (33%). Additional non-cardiac malformations (three-quarters being chromosomal aberrations) are found in more than 60%.
Insurances
Forty patients (28.4%) out of our study population complained about having problems with insurances, due to their CHD. Problems were mainly encountered with health insurances – astonishingly there were no big differences between the five groups of CHD. In Switzerland everybody has health insurance, and the problems reported by GUCH patients were mainly related in getting private health insurance. These findings are not unexpected – Celermajer and Deanfield [15] reported on the difficulties encountered by GUCH patients trying to obtain health and life insurance, and how the actuarial risk quoted by the insurance companies usually bore little relation to the long-term outcome.
Pregnancy
A total of 27% of the patients answered that they were anxious about transmitting some form of CHD to their offspring. Six out of 81 women (7.4%) decided against ever becoming pregnant because of their CHD. Anxiety concerning genetic issues, sudden death and fertility must be recognized in this collective of patients and sensitive counselling and support are necessary [4].
Only nine women (11.1%) were seen by a cardiologist before or during pregnancy—and these were mainly women who were followed regularly by a cardiologist once or even twice a year. According to the recommendations [4] it is of great importance that women suffering from CHD, should have a cardiological check-up and counselling before and during pregnancy. In many of these patients, pregnancy is uneventful and any problems that do occur are usually not related to CHD [4]. Cardiovascular problems during pregnancy were minor and reported in only 12% of the women, which is in accordance with the guidelines published by Pyeritz [16] and revised by our group [17], that patients with minor cardiovascular diseases and an aortic annulus smaller than 4.5 cm can be considered as having a low cardiovascular risk during pregnancy. Only in a small group with complex cyanotic CHD, pulmonary hypertension (Eisenmenger syndrome) and aortic disease, is pregnancy dangerous and not recommended [16–19].
In our study 73 children were born and five (6.9%) suffered from a CHD. As the incidence of CHD is much higher in GUCH parents than in the standard population, expert foetal echocardiography must be available in these patients and its potential consequences regarding abortion have to be discussed early with the parents [4]. Peri-conceptual use of multivitamins, especially folic acid, may reduce the occurrence of certain lesions and should therefore be recommended [20].
Physical activity
Physical activity in adult patients with CHD is quite similar to the data reported in a standard population. These findings are not unexpected and confirm the findings from previous studies [8, 21].
Limitations
The main limitation of the study is the heterogeneity of the study population. However, the answers were quite similar, irrespective of whether the patients had multiple cardiac surgeries or just the one intervention. Psychosocial problems were only partly related to the type of disease. However the patient's aspect is important – and that is that patients undergoing cardiac surgery for CHD after the age of 14 years may expect a normal QoL after recovery from surgery. Impairment in QoL in this surgical collective was mostly related to additional non-cardiac malformations, as described above for patients with CAVC. Early surgery, as it is currently performed, may additionally improve the long-term outcome in this collective of patients.
Conclusions
Outcome and QoL following cardiac surgery in adolescents and adults with CHD after the age of 14 years are excellent and similar with an age- and gender-matched standard population. Limitations are mainly found in patients suffering from additional non-cardiac malformations. In the future we have to focus more on the medical follow-up and psychosocial problems in this increasing group of patients. More specialist units within cardiology departments are mandatory in order to manage problems in any grown-up patient with CHD and to enable education and training of the profession and facilitate innovative research.