
Abstract
Background
Recent guidelines target individuals at highest risk as a priority. However, implementation of guidelines even in this group is sub-optimal.
Design
A multicenter, observational follow-up study.
Methods
A total of 5600 consecutive patients ≥55 year with high risk of vascular events were evaluated for risk factors and medication usage and followed for 1 year for primary end-points (death, myocardial infarction, stroke), and secondary end-points (revascularization, hospitalization).
Results
The patients were divided into two groups: those without and with vascular disease. In the first group, mortality at 1 year was significantly higher in those with end organ damage (5.8 versus 2.7%, P= 0.005). Similarly, the mortality in patients with known vascular disease (CAD, peripheral vascular disease, ischaemic stroke) was higher in the presence of a previous vascular event (7.8 versus 5.3%, P=0.055, vascular event: non-fatal MI/stroke). The use of antiplatelets, statins, beta-blockers and angiotensin-converting enzyme inhibitors was low and did not improve in the follow-up period. The most important predictors of cardiovascular mortality were the presence of end organ damage [odds ratio (OR) 1.65, P= 0.001], pre-existing vascular disease (OR 1.49, P= 0.023) and protectively, the consistent use of angiotensin-converting enzyme inhibitors (OR 0.49, P= 0.001).
Conclusion
In a high-risk Turkish population, the early mortality and morbidity due to cardiovascular events was unacceptably high and medical treatment inadequate. The presence of end organ damage and a previous vascular event increased the risk even further and should be vigorously questioned. Aggressive lifestyle modification and medical therapy should be instituted in these patients.
Introduction
Atherosclerotic vascular disease, which encompasses coronary artery disease, cerebrovascular disease and peripheral arterial disease, is responsible for the majority of deaths in most European countries including Turkey [1]. The Turkish population has a high coronary mortality despite being a young population. This is caused by a high prevalence of smoking, remarkably low high-density lipoprotein (HDL) cholesterol levels and increasingly unhealthy habits of food consumption since the 1990s leading to an increase in plasma triglyceride levels as well as the incidence of obesity, diabetes and hypertension [2–4]. The clustering of these risk factors in the population has necessitated serious preventive measures and implementation of guidelines. All the recent guidelines including the Third Joint Task Force of European and other Societies on Cardiovascular Disease Prevention in Clinical Practice target those at highest cardiovascular risk as a priority [5].
The definition of high-risk individuals according to the NCEP ATP III report are those with coronary or other forms of atherosclerotic vascular disease, diabetes or the presence of multiple risk factors that confer a 10-year risk for coronary heart disease over 20%. The strategy that is currently recommended is to address all the risk factors and provide total risk management in these patients. Targeting these high-risk patients will lead to the greatest benefits and most cost effective use of medical resources. Within the group of patients at high risk for cardiovascular events, identifying the subset of patients at highest risk for early events will be very useful for the effective use of limited resources. Furthermore, the recent NCEP report defined more aggressive low-density lipoprotein (LDL) cholesterol goals for patients at very high risk.
The aim of this study was to study the high atherosclerotic vascular risk patient profile in the country, evaluate the early event rates in these patients and identify the highest risk subset of these patients who experience cardiovascular morbidity and mortality within the first year of follow-up. Since there is considerable discrepancy between guidelines and what is actually being practised in the real world, we also sought to determine the use of optimal medical treatment in these patients.
Methods
This was a multicentre, observational, follow-up study with clinical end-points at 1 year. The study was conducted in 10 representative cities from different geographical regions of the country. There were 305 investigators from cardiology, internal medicine, endocrinology and primary care clinics who participated in the study. Consecutive patients who presented to these outpatient clinics and satisfied the inclusion criteria were enrolled in the study. After baseline evaluation, the patients were assessed again in 3, 6 and 12 months. This was an observational study and no intervention was performed on the patients besides usual care. A total of 5600 high-risk individuals who satisfied the inclusion criteria were enrolled in the study. The inclusion criteria were: being above the age of 55 and having a high risk of cardiovascular events according to the following definition that high risk was defined as having coronary artery disease, stroke, peripheral vascular disease, diabetes mellitus and hypertension. All these patients were evaluated by a detailed history, physical examination including height and weight measurements, electrocardiogram and laboratory measurements after a 12 h fasting at baseline and following visits. The parameters that were recorded were the conventional cardiovascular risk factors (hypercholesterolaemia above 200 mg/dl, low HDL cholesterol below 40 mg/dl, hypertension, family history of premature coronary heart disease, diabetes, smoking, obesity) the presence of end organ damage (left ventricular hypertrophy, heart failure, microalbuminuria, renal failure), and the presence of atrial fibrillation, which by itself increases risk. The total cholesterol and HDL cholesterol measurements were performed by enzymatic methods. The height and weight were measured by a mechanical scale and ruler (Nan tarti A.Ş.). The blood pressure measurements were performed with a mercury sphygmomanometer that was calibrated monthly (Erka; Kallmeyer Medizintechnik GmbH, Germany). Patients who currently smoked were categorized as smokers. In patients with known vascular disease, the presence of a previous vascular event in the form of MI or stroke was also noted. The medical treatment regimen of each patient was also recorded at each visit. A total of 5600 consecutive patients were enrolled in the study and 3331 consenting patients were followed up for 1 year.
The patients were divided into five major groups according to the presence of vascular disease, diabetes and or hypertension.
Diabetes present, no vascular disease.
Hypertension present, no vascular disease.
Diabetes and hypertension present, no vascular disease.
Vascular disease without diabetes or hypertension.
Vascular disease with diabetes and or hypertension.
The presence of vascular disease was defined as having angiographically documented coronary artery disease, a history of well-documented myocardial infarction, percutaneous intervention, bypass surgery, ultrasonographically or angiographically documented carotid or peripheral artery disease, and a history of stroke.
The primary end-points of the study were death, non-fatal myocardial infarction (MI) or stroke. The secondary end-points were revascularization defined as a percutaneous intervention or coronary bypass surgery and hospitalization due to cardiovascular causes.
The nucleus members of the vascular risk study formed the steering committee responsible for data, safety and review. Data storage and statistical analysis of the study were performed by an independent contract research organization. Interim analysis reports of the data were presented to the investigators every 3 months by the contract research organization.
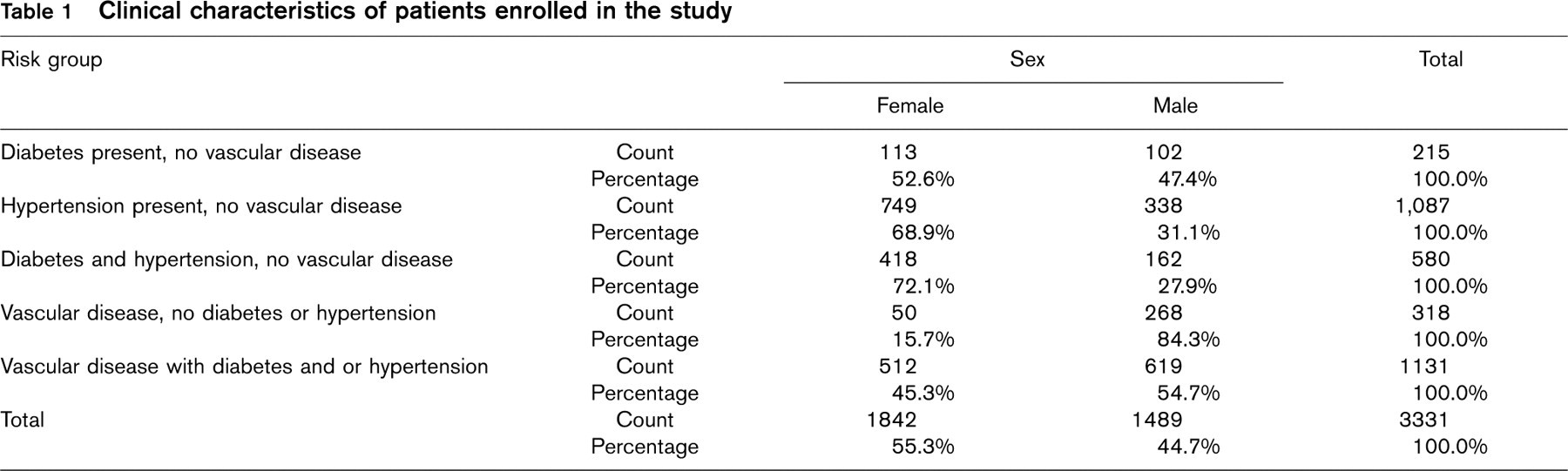
Clinical characteristics of patients enrolled in the study
Statistical analysis
A sample size of at least 425 subjects per comparison group was calculated to be necessary to detect a significant difference based on the assumption of incidence of end-point events of 12% in one group and 7% in another one to achieve a power of 80% on a significance level of 10%. Since with greater differences, which are expected for our study groups, lesser group sizes are enough and a sample size of 2125 is calculated as optimum. But a loss to follow-up rate of 50% and differences in prevalence of study group types were expected. The large sample size of a minimum of 5500 subjects was chosen in order to obtain more reliable results regarding these limitations.
For univariate evaluation of demographic, clinical baseline characteristics and end-point results, ANOVA with Tukey's HSD for post hoc analysis, chi-square test or Student's t-test are used according to the type of variable and number of groups.
Given the limited length of the observational period and since end-point data were collected for only specific times (3, 6 and 12 months), time-to-event dates are generally not well identified. For these reasons, logistic regression analysis is preferred as an approximation of Cox proportional hazards model. Following the results of univariate analysis for end-point events (MACE) within 1 year of follow-up, all appropriate variables are included in a logistic regression evaluation. Odds ratios (OR) and 95% confidence intervals (CI) are given from the results of this analysis. A P-value of < 0.05 was considered statistically significant.
Results
A total of 3331 (59%) of the patients were followed-up for 1 year and completed the study. The characteristics of these patients are outlined in Table 1. There were 3176 female (56.7%) and 2424 male patients (43.3%) enrolled in the study. The mean age was 64 (65 for women and 64 for men). Of these patients, 2236 (39.9%) had vascular disease, 404 had diabetes only (7.2%), 1910 had hypertension only (34.1%) and 1050 (18.8%) had both diabetes and hypertension. The vascular disease was coronary artery disease in 35.7%, ischaemic stroke in 4.5% and peripheral vascular disease in 3.7% of the patients. There was a coexistence of coronary artery disease and stroke in 4.38%, coronary artery disease and peripheral vascular disease in 5.23% and peripheral vascular disease and stroke in 0.67% of these patients. All three vascular systems were involved in 0.31% of these patients. The presence of different cardiac risk factors is shown in Table 2. In this population with high risk, hypercholesterolaemia (51.4%), low HDL (37.7%) and obesity (28.7%) were the most prevalent risk factors. The medications these patients with high risk were receiving at the baseline visit were also documented. Antiplatelet use was 41.3%, angiotensin-converting enzyme inhibitor use was 50.5%, statin use was 25.8% and beta-blocker use was 20.9% in these patients.
Distribution of cardiac risk factors
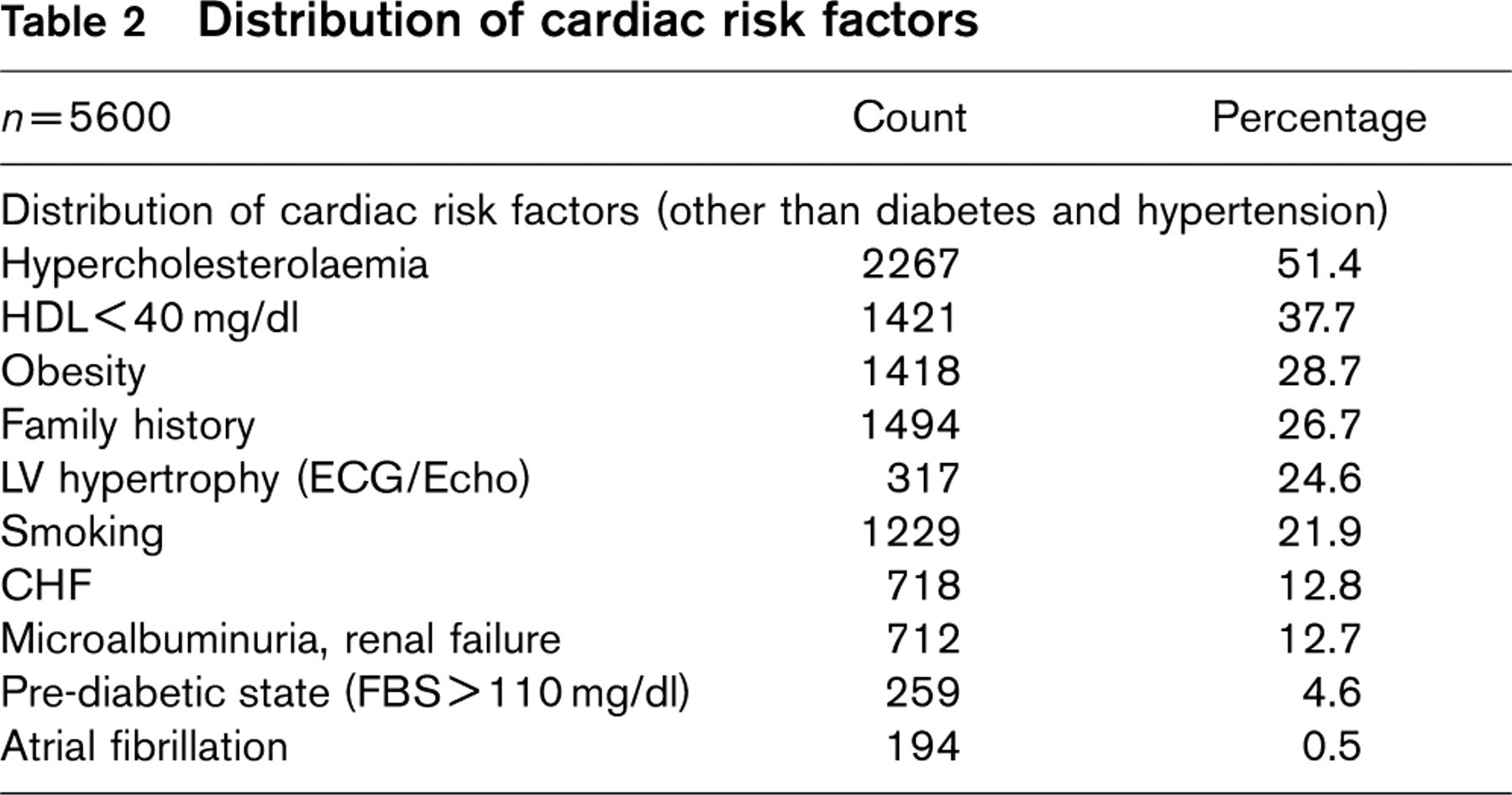
HDL, high-density lipoprotein cholesterol; LV, left ventricular; ECG, electrocardiogram; CHF, chronic heart failure.
Primary end-points
The primary end-points of death, non-fatal MI or stroke were met in a large number of patients. At the end of one year, 156 (4.7%) patients had died, and 129 (3.9%) of these deaths were due to cardiac causes. In patients without known vascular disease, the highest mortality rate was seen in diabetics with organ damage, which was 11.5%. The 1-year mortality was 3.2% in diabetics without end organ damage. Hypertensive patients without organ damage had a mortality of 2.6% whereas those with organ damage had a 5.8% mortality. Diabetic (P = 0.046) or hypertensive patients (P = 0.027) had significantly higher mortality if they had accompanying end organ damage. The mortality was also high in patients with known vascular disease at the end of 1 year reaching 5.3% in those without a previous vascular event and 7.8% in patients with a previous vascular event (P = 0.055). The presence of diabetes or hypertension in addition to having vascular disease affected overall mortality significantly (9.1 versus 5.9%, P = 0.043). Likewise, primary end-points were affected significantly with the presence or absence of diabetes or hypertension in addition to vascular disease (13.8 versus 9.9%, P=0.046).
Primary, secondary and combined end-points according to the presence of vascular disease and organ damage
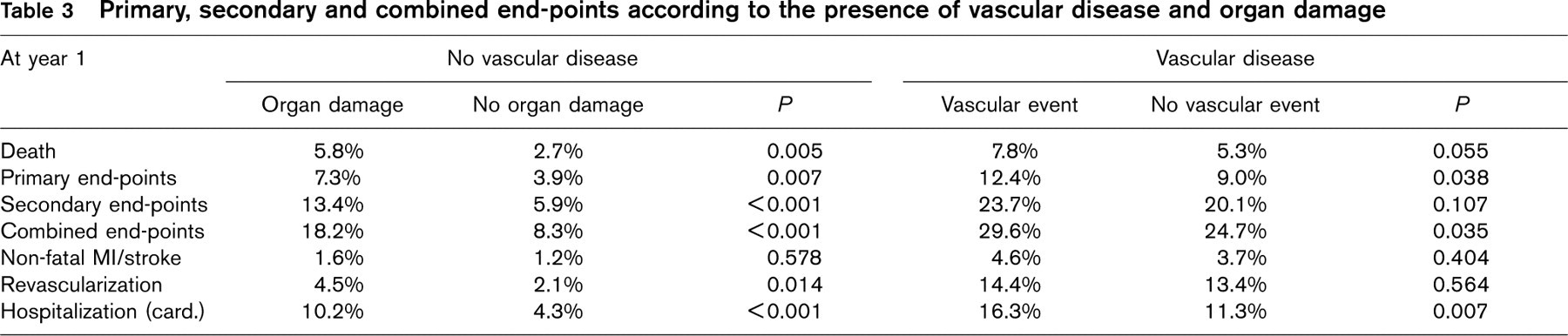
MI, myocardial infarction.
Non-fatal MI or stroke was seen in 1.6% of the patients having end organ damage either due to diabetes or hypertension versus 1.2% of those without end organ damage (P = 0.578). In patients with vascular disease, non-fatal MI or stroke were seen slightly more frequently in patients with a history of previous MI or stroke (4.6 versus 3.7%, P = 0.404).
In patients with known vascular disease, the combined primary end-point was significantly higher in those with a previous event compared to those without (12.4 versus 9%, P=0.038).
Secondary end-points
The secondary end-points of revascularization were met in 249 (7.5%) and hospitalization for cardiovascular causes were seen in 301 (9%) of patients.
Revascularization was performed in 2.1% of the diabetics, 3.6% of the hypertensives (2.9% of this was hypertensives with end organ damage) and 3% of patients with both diabetes and hypertension. Hospitalizations for cardiac causes were even higher: 11.9% of diabetics, 9.7% of hypertensives and 22.7% of patients with both diabetes and hypertension were hospitalized for cardiac reasons during the year. The combined secondary end-points were almost twice as high in patients with end organ damage (20.8%) than those without (11.5%) (P<0.001).
As for patients with vascular disease, revascularization was performed in 13.4% of those without a previous vascular event and 14.4% of those with a previous event (P = 0.564). Hospitalization for cardiac causes was higher in patients with vascular disease who had a previous vascular event (11.3 versus 16.3%, P = 0.007).
Combined primary and secondary end-points
When all end-points were combined, in patients with diabetes and/or hypertension without known vascular disease, patients with end organ damage had a significantly higher percentage of all events compared to those without end organ damage (18.2 versus 8.3%, P < 0.001). In patients with vascular disease, combined end-points were significantly higher in patients with previous cardiovascular events compared to those without (29.6 versus 24.7%, P = 0.035). Of all the patients in the study group, patients with vascular disease and previous events did the worst in terms of combined end-points (Table 3).
Medication use
The use of antiplatelets, statins, beta-blockers and angiotensin-converting enzyme inhibitors was low in most patients and did not improve in the follow-up period (Table 4).
Multivariate analysis was performed in order to determine the predictors of cardiovascular mortality. The most important predictors of cardiovascular mortality were the presence of end organ damage (OR 1.65, 95% CI 1.29–2.12, P = 0.001), pre-existing vascular disease (OR 1.49, 95% CI 1.06–2.09, P = 0.023) and protectively the consistent use of angiotensin-converting enzyme inhibitor use (OR 0.49, 95% CI 0.35–0.68, P=0.001)(Table 5, Figure 1).
Discussion
In this population at high risk, conventional risk factors like hypercholesterolaemia, low HDL cholesterol levels, obesity and smoking were prevalent showing once again that the risk factors tend to cluster and explaining the high morbidity and mortality rates we saw at the end of 1 year. Recent evidence from 14 randomized trials and three observational studies following 386 915 patients confirms that more than 95% of patients who experience a fatal coronary event have at least one major risk factor [6, 7]. These studies have re-emphasized that severe public health measures need to be taken to fight with modifiable risk factors and have debunked the myth that only half the patients with cardiovascular events have conventional risk factors [8].
Medication use in different groups at baseline and at 12 months
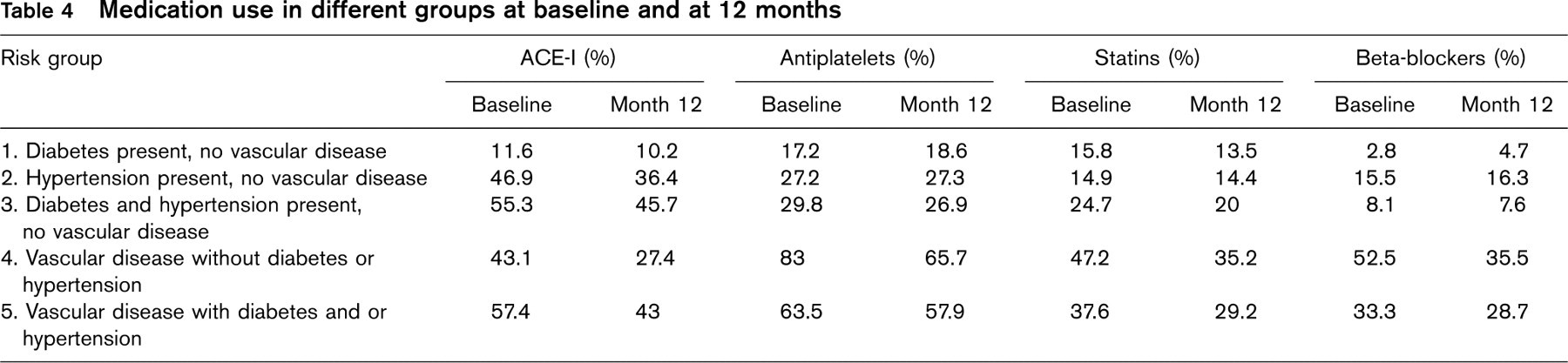
ACE-I, angiotensin-converting enzyme inhibitor.
Predictors of cardiovascular death on multivariate analysis
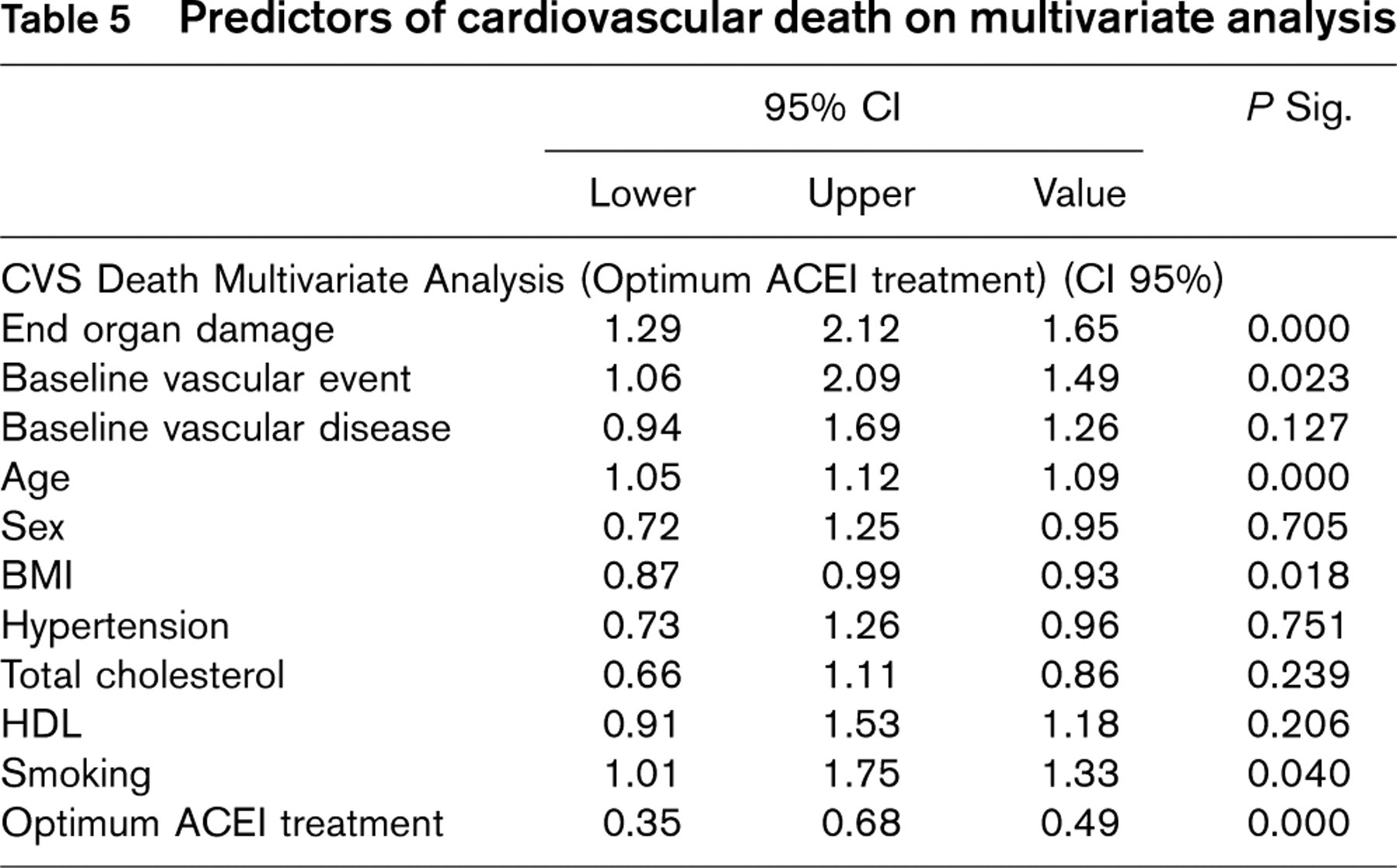
ACEI, angiotensin-converting enzyme inhibitor, CI, confidence interval; BMI, body mass index; HDL, high density lipoprotein.
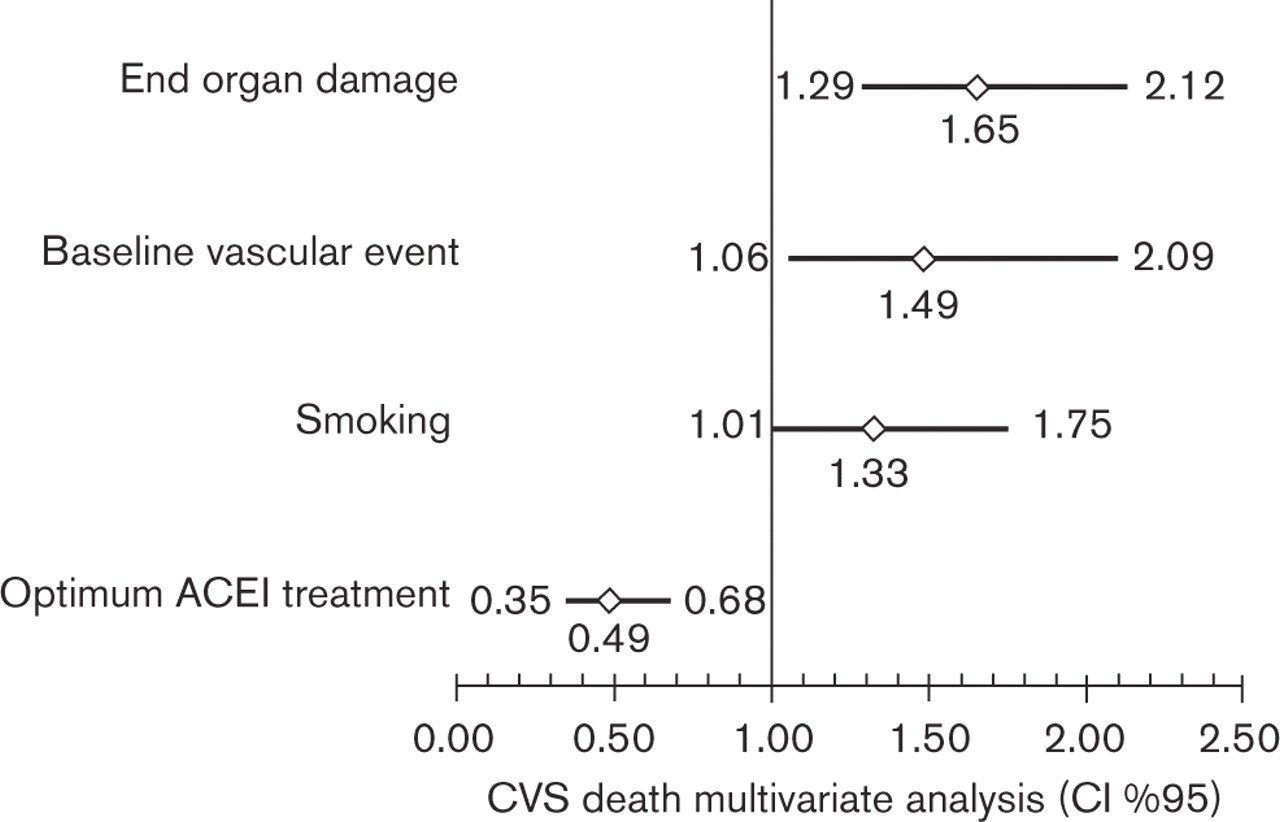
Significant predictors of cardiovascular death in multivariate analysis. ACEI, angiotensin-converting enzyme inhibitor; CI, confidence interval.
Although the follow-up was only for 1 year, we saw an alarmingly high rate of primary and secondary end-points in the study population. Our study population already had a high-risk profile for early events. We sought to find the subgroup with even higher risk in this population. We found that patients with pre-existing disease in the vascular bed had the worst prognosis as expected. In this group, those with a previous myocardial infarction or stroke significantly had a higher chance of recurrent events. Secondary end-points of revascularization and hospitalization were also higher in these patients. These results are in concordance with previous studies that show that a history of stroke or myocardial infarction increases the risk of a recurrent event two- to nine-fold [9]. In the patients without pre-existing vascular disease, those with end organ damage had significantly more events than those without organ damage, whether the damage was due to hypertension or diabetes. The highest number of events was in the group with diabetes and end organ damage. The event rates here were comparable to those with pre-existing vascular disease. These results once again confirm the guidelines that rank diabetes in the high-risk category [10, 11]. Similar results were found for secondary end-points of revascularization and hospitalization. Overall, when all end-points were combined, half the patients with end organ damage and those with known vascular disease experienced some unfavourable event during the very short period of 1 year, once again confirming the severity of the situation of these patients. Therefore, we propose that the presence of a previous vascular event and end organ damage are important additive predictors of increased risk in those patients with an already high risk and should be considered in the evaluation of these patients.
The Joint European Societies has recommended the use of antiplatelets, beta-blockers, angiotensin-converting enzyme inhibitors and lipid-lowering therapies in addition to lifestyle modification for the purpose of lowering morbidity and mortality. In our patients, the respective uses of these drugs were inappropriately low in these extremely high-risk patients. The fact that less than half these patients were on aspirin shows us that there is a lot of room for improvement for the implementation of guidelines. Similarly, in EUROASPIRE II, the use of these medications was sub-optimal on admission and increased after discharge [12]. The results of EUROASPIRE II and our study show that integration of vascular prevention into daily practice is inadequate.
In conclusion, in this high-risk middle-aged Turkish population with adequate representation of both genders, the early mortality and morbidity due to cardiovascular events was unacceptably high and medical treatment inadequate. The presence of end organ damage and a previous vascular event increased the risk even further. We recommend that in the evaluation of these patients, end organ damage and a previous event should be vigorously questioned. Aggressive lifestyle modification and medical therapy should be instituted in these patients. Better implementation of pre-existing guidelines, and training the physicians and patients are necessary to close the gap between evidence-based medicine and daily practice.
Footnotes
Acknowledgements
This study was supported by a grant from Aventis Pharma, Turkey.