
Abstract
Background
There is substantial evidence that treatment with lipid-lowering agents can decrease cardiovascular morbidity and total mortality in patients with elevated serum lipid values and/or prior ischaemic heart disease. However, only a minority of these high-risk patients are believed to receive treatment, and among those who do receive pharmaceutical treatment the majority do not reach the therapeutic goal. Our goal was to investigate if this translates to a higher risk of cardiovascular events in real clinical practice.
Design
A retrospective cohort study using linkage of electronic medical records, the Swedish national inpatient registry and cause of death registry was performed, enrolling a total of 4976 patients who received treatment with a lipid-lowering agent at any time between 1 January 1993 and 1 December 2001.
Methods
Cox proportional hazards regression was used to evaluate the impact of goal attainment along with potential confounding factors.
Results
Patients who reached treatment goals were 24% less likely to suffer a cardiovascular event (relative risk: 0.76, 95% confidence interval: 0.60–0.96) than patients who did not reach treatment goals. A substantial proportion of patients treated with lipid-lowering agents do not achieve the treatment goals.
Conclusions
Failure to reach treatment goals translates into a higher risk of cardiovascular events, and it is thus of importance to ensure that patients reach goals.
Introduction
There is substantial evidence that treatment with lipid-lowering agents can decrease cardiovascular morbidity and total mortality in patients with elevated serum lipid values and/or prior ischaemic heart disease. However, only a minority of these high-risk patients are believed to receive treatment, and among those who do receive pharmaceutical treatment the majority do not reach the therapeutic goal. In a cross-sectional study from the UK, only 44% of patients receiving lipid-lowering treatment reached the goal of total cholesterol level <5.0 mmol/l [1]. Similarly, in a US study, only 14% in a sample of patients with cardiovascular disease had reached the target value of low-density lipoprotein cholesterol (LDL) levels < 2.58 mmol/l [2]. The EUROASPIRE I and II studies showed that the share of coronary heart disease patients with high total cholesterol (>5.0 mmol/l) decreased from 86.2 to 58.8% between 1996 and 2000 – a definite improvement but still indicating that the majority of patients do not achieve treatment goals [3]. Failure to achieve treatment goals has been shown to be associated with increased cardiovascular morbidity and mortality [4,5].
The Return on Expenditure Achieved for Lipid TherapY (REALITY) was a multi-centre retrospective population-based study of patients prescribed lipid-lowering drugs in a primary care clinical setting in nine European countries. The purpose of the REALITY study was threefold: (1) to investigate treatment patterns in patients treated for hypercholesterolaemia and how they affect the achievement of treatment goals; (2) to investigate how treatment and treatment goals affect costs; and (3) to investigate the association between goal attainment and frequency of subsequent cardiovascular disease events. In this paper, we report our findings with regard to cardiovascular outcomes.
Material and methods
The REALITY Sweden study had a population-based approach and included patients from all 27 primary care centres in the County of Uppsala in Sweden and two additional centres, one from the Västra Götaland region and one from the Stockholm metropolitan area were included, comprising 29 centres in all (centres listed in Acknowledgements). The use of the same electronic medical record system at all participating centres made it possible to identify patients eligible for the study.
Three electronic data sources were used to extract information: the electronic medical records at the primary health care centres, the Swedish national inpatient register and the Swedish cause of death register. The regional research ethics committees in the involved health care regions approved the study, before data extraction.
The electronic medical records contain information about all visits to primary health care providers, including the results from laboratory tests taken and information on what drugs are prescribed. Tests taken in a hospital setting are not included.
The Swedish national inpatient register is maintained by the Centre for Epidemiology at the National Board of Health and Welfare. It covers all public inpatient care since 1987 and includes the reasons for hospitalization and procedures performed (by ICD code) as well as date of admission and discharge. Registration is mandatory and is administrated by the county councils. While there is some underreporting, it is estimated to affect less than 2% of hospitalizations [6].
The Swedish cause of death register contains the cause of death for all deceased residents in Sweden based on death certificates. The register contains some demographic information and the underlying cause of death, defined as the disease, the injury that initiated the sequence of diseases that finally resulted in death, the circumstances surrounding the accident, or the act of violence that caused the lethal injury. The register is maintained by the Centre for Epidemiology at the National Board of Health and Welfare [7].
Patients older than 18 years of age prescribed a lipid-lowering drug (ATC class C10A) between 1 January 1993 and 1 December 2001 were included in the study. Data extraction commenced on 1 December 2002 using specially developed software to access the primary health care records. Inpatient care records of patients and date and cause of death (if applicable) were extracted from the inpatient care and cause of death registers by matching patients using their personal registration number. These numbers were replaced by an anonymous study ID to maintain patient confidentiality during the analysis.
Goal attainment was defined as having a total cholesterol level below 5.0 mmol/l and a LDL cholesterol level of below 3.0 mmol/l (according to recommendation from the Swedish Medical Products Agency), within a 12-month period following the index prescription [8]. In cases with only one of the two lipid parameters available, patients were considered to be at goal if it was below the goal value. If both LDL and total cholesterol measurements were available, both needed to be below the target values for the patient to be considered at goal. Patients without cholesterol measurements in the 12-month period were excluded from the analysis. Patients who were already at or below the treatment goal any time from 180 days prior to the index date to or 5 days after the index date were also excluded from the analysis.
A cardiovascular event was defined as a hospitalization with a primary or secondary diagnosis of acute myocardial infarction (AMI), acute stroke or a hospitalization with a revascularization procedure (coronary artery bypass graft [CABG] or percutaneous transluminal coronary angioplasty [PTCA]) or cardiovascular death. The following diagnosis codes were included: 410, 411, 431–437 according to ICD-9 (–1996) and 121–123, 161–165 according to ICD-10 (1997–). Operation codes were identified according to the current and previous version of the Swedish Classification of Surgical Procedures (KKÅ97). Included codes were 3066, 3068, 3080, 3092, 3105, 3127, 3158, FNA00, FNA10, FNA20, FNA96, FNB00, FNB20, FNB96, FNC00, FNC10, FNC20, FNC30, FNC40, FNC50, FNC60, FNC96, FNG00, FNG02 and FNG05. Cardiovascular death was defined as any death with an underlying cause of death belonging to ICD-9 chapter VII or ICD-10 chapter IX. Only the first event during the period was included in the analysis.
The following variables were considered potential confounding factors and extracted from the electronic medical records from the primary care centres: patient age (at index prescription), gender, diastolic blood pressure (DBP, the mean DBP between 180 days prior to and 90 days after the index prescription was used, we assumed that hypertensive patients would see their physician at least once during such an interval), systolic blood pressure (SBP, the mean SBP between 180 days prior to and 90 days after the index prescription was used), diabetes mellitus (defined as a diagnosis of diabetes mellitus at any contact during the study period), body mass index (BMI, using any measure of height during the study period and the weight measure closest to the index date), smoking status (ever smoker or never smoker) and previous cardiovascular disease (defined as a hospitalization for any of the cardiovascular outcomes described previously but also including angina pectoris, coronary insufficiency, chronic ischemia or post infarction or post stroke syndromes).
Data was analyzed using Kaplan–Meier and Cox proportional hazards survival models using plots and the Grambsch and Therneau test to verify the proportional hazards assumption.
Results
A total of 7795 patients were extracted from the primary care records. Of these, 4976 were uncontrolled or lacked cholesterol measurements at the index prescription and had at least one cholesterol measurement during the 12 months following the index date and were thus included in the analysis. A total of 2480 patients were excluded due to a lack of cholesterol measurement during the follow-up period post index prescription and 339 patients were excluded because their cholesterol levels at baseline were at or below the target levels. One patient lacked information on gender, and was therefore not included in the survival analysis but was retained for the other parts of the study.
Patient characteristics at the index prescription
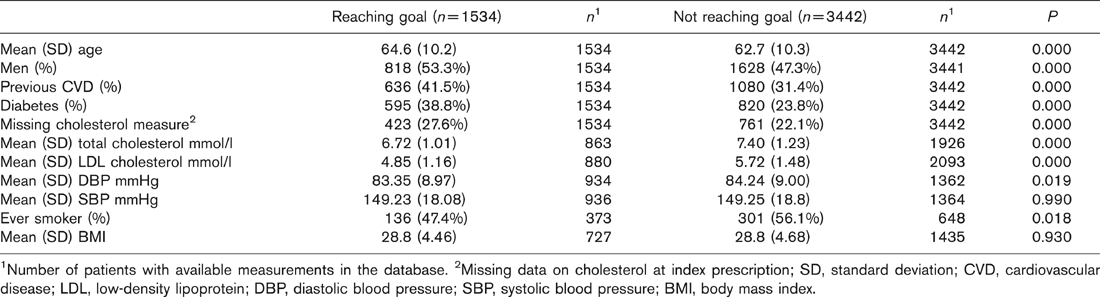
1 Number of patients with available measurements in the database.
2 Missing data on cholesterol at index prescription; SD, standard deviation; CVD, cardiovascular disease; LDL, low-density lipoprotein; DBP, diastolic blood pressure; SBP, systolic blood pressure; BMI, body mass index.
Table 1 shows the demographic characteristics for those who reached the treatment goal and those who did not. Patients who reached the treatment goal were on average older and the prevalence of cardiovascular disease and diabetes was higher in this group. Patients who did not reach the goals on the other hand had higher cholesterol levels at the index prescription and more patients in this group were smokers. Blood pressure and BMI were similar in the two groups.
A reduction in both total and LDL cholesterol can be observed in both groups during the 12 months after the index prescription. However, the reduction was larger among those who reach treatment goals, where total cholesterol was reduced by 2.41 mmol/l [95% confidence interval (CI): 2.34–2.47] and LDL cholesterol by 2.56 mmol/l (95% CI: 2.48–2.64). In the other group, total cholesterol was reduced by 1.51 mmol/l (95% CI: 1.45–1.56) and LDL cholesterol by 1.61 mmol/l (95% CI: 1.55–1.67).
Among the 4976 patients followed, there were 418 cardiovascular events (counting only the first event) during the study period after the index prescription. Figure 1 shows the Kaplan-Meier survival curves for time to cardiovascular events for patients who did and did not reach the treatment goals. As can be seen, the risk is slightly higher among patients who did not achieve the goals, but the difference is not very large.
Table 2 shows the results from the Cox proportional hazards model including variables with complete information for all patients. An alternative model with a dummy variable indicating if patients had a cholesterol measurement at their index prescription was also tested, but this had no impact on the results (relative risk: 0.993, 95% CI: 0.797–1.238). Male patients, patients with diabetes and patients with a history of cardiovascular disease had a higher risk of events. Increasing age was also associated with a higher risk of events. Patients who reached their treatment goals had a 24% reduction in the risk of suffering an event (a relative risk of 0.76 with 95% CI: 0.60–0.96).
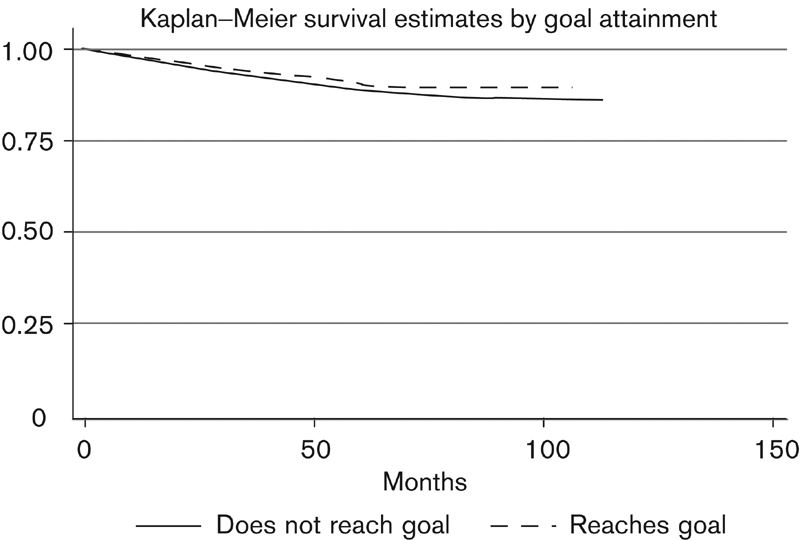
Kaplan–Meier survival estimate on the time to cardiovascular evens for patients reaching and not reaching treatment goals (n = 4974).
Results from Cox proportional hazards model (n = 4974) including all variables with complete information
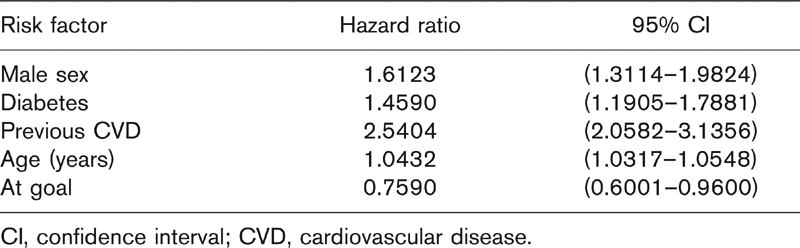
CI, confidence interval; CVD, cardiovascular disease.
Discussion
Our results show that patients who reach their treatment goals decrease their risk of cardiovascular events by 24% (a relative risk of 0.76). This is consistent with the findings of several clinical trials in both primary and secondary prevention [9–14. These trials demonstrated that cholesterol lowering reduces cardiovascular events in a clinical trial setting. However, none of the trials examined the difference in cardiovascular disease (CVD) events between patients who are on therapy and do or do not achieve goal.
The risk reduction is thus on par with what has been observed in clinical trials, but the confidence interval around the relative risk is quite wide, with the upper bound close to 1 (0.960). This may be due to insufficient power. Had more patients been included or the observational time been longer the confidence intervals would likely have been smaller, as this would lead to a larger number of events.
Since data were extracted from real-life medical records, the availability of information on possible confounders is limited by what tests the primary care physician decided to conduct. In our dataset, this resulted in limited data on blood pressure, BMI and smoking status. Blood pressure and BMI pose a minor problem since they are similarly distributed between the groups and it is likely that patients with high BMI or with suspected hypertension had been investigated by the physician and thus had available measures. The few recordings of smoking status may be of greater importance, since this factor is not often recorded and there appears to be more smokers among those who fail to reach the treatment goals. Smoking could thus be a potential confounding factor in our analysis; however, its impact is probably not very large, since the difference between the groups is not very large. There could also be differences in unobserved risk factors between the groups. Major known medical risk factors like prior CVD or diabetes mellitus are included but factors such as low socio-economic status, poor diet and physical inactivity, all intimately tied together, are not. It could be speculated that these risk factors are more prevalent among patients who do not attain treatment goals, and they should also be over-represented in patients with diabetes and previous cardiovascular disease. However, these factors are more prevalent among patients who reach their treatment goals.
The inpatient register only includes data from the hospitals run by the County Councils; private hospitals are thus excluded. Hospitalizations to these make up only a small fraction of all hospitalizations, and mainly elective surgery is performed, so this is probably of little consequence to our event classification.
Our study does not analyze patients treated with lifestyle interventions such as diet or exercise. Patients receiving lifestyle interventions are hard to identify in an automated fashion from the electronic medical records.
The biggest advantage of our study is its high external validity. These data represent the treatment patterns in actual clinical practice without the influence of a study protocol. In spite of this, we see a risk reduction similar to that observed in clinical trials. To our knowledge, this is the first study where the importance of goal attainment has been confirmed in this context. A follow-up study would be important to include more events over time and thus get more precise estimates of the benefits of goal attainment. This would also permit analyses of the effect of the increased use of statins over time.
Our findings underscore the importance of achieving treatment goals. Factors influencing the probability of goal attainment are also an important topic for future research.
Footnotes
Acknowledgements
Part of this work has been presented as abstracts at ACC 2004 and the Swedish Medical Association Meeting. This work was funded by a grant from Merck & Co., New Jersey, USA. Patients from the following primary care centres were included in the study: Alunda, Bålsta, Enköping, Eriksberg, Fjärdhundra, Flogsta, Gimo, Gottsunda, Heimdal, Knivsta, Knutby, Kungsgärdet, Liljeforstorg, Liljeholmen, Luthagen, Möllan, Nyby, Samariterhemmet, Skutskär, Storvreta, Svartbäcken, Sävja, Tierp, Årsta, Öregrund, Örsundsbro, Österbybruk and Östhammar.