
Abstract
Background Gender differences in presentation and management of acute coronary syndromes (ACS) are well established internationally. This study investigated differences in a national Irish sample.
Design Cross-sectional survey.
Methods All centres (n = 39) admitting cardiac patients to intensive/coronary care provided information on 25 consecutive acute myocardial infarction patients and other ACS patients admitted concurrently (n = 1365 episodes). Patient data was analyzed in terms of those with prior ACS/revascularization, and those without.
Results Men with prior established ACS/revascularization were twice as likely to have received revascularization procedures (coronary artery bypass graft or percutaneous coronary intervention) prior to admission when controlling for age, total cholesterol and insurance status [odds ratio (OR) 1.97, 95% confidence interval (CI) 1.18–3.29, P=0.011]. No gender differences were seen in acute-phase reperfusion (OR 0.96, 95% CI 0.76–1.24, P>0.05) or antiplatelet therapy (OR 0.99, 95% CI 0.69–1.41, P>0.05). For patients with prior ACS/revascularization, men were twice as likely to receive statins on discharge after adjustment for age and total cholesterol (OR 1.94, 95% CI 1.02–3.71, P=0.045).
Conclusions Women were treated differently to men. Fewer women with a positive history of ACS received revascularization prior to current admission and fewer women were prescribed lipid-lowering medications on discharge. Acute phase hospital treatment was not gender determined. These findings have implications for secondary prevention in Ireland.
Introduction
Gender differences in the presentation and management of acute coronary syndromes (ACS) are well established internationally [1–3]. Previous research has reported that women present with different symptomatology and may subsequently be diagnosed differently [1, 4]. Women admitted for ACS also have lower rates of prior revascularization, both bypass surgery and percutaneous coronary intervention (PCI) [2, 5]. During the acute phase of hospitalization, there is evidence that women receive less reperfusion therapy [1]. The medications prescribed on discharge may vary by gender. The Euro Heart Survey of ACS demonstrated that women were less likely to receive antiplatelets, beta-blockers and statins on discharge, but more likely to receive diuretic medication [3].
Little is known about the current gender profile of treatment of ACS in Ireland. This study analyzed gender differences in the presentation and management of a national cohort of suspected ACS patients admitted to intensive or coronary care units in all 39 Republic of Ireland hospitals providing such care.
Method
Sample/Participants
All Irish centres admitting suspected acute myocardial infarction patients to intensive/coronary care units (I/CCU) were invited and agreed to participate in the survey (n = 39). Ethics committee approval was obtained from individual centres/areas as appropriate [6]. Data were collected in 2003.
Participants and procedure
Suspected ACS patients admitted to intensive/coronary care were recruited. This included patients with an admission diagnosis of either acute myocardial infarction or unstable angina. All relevant staff were supplied with the consensus definition of ACS, which uses enzyme change as a marker for necrosis [7]. Participating hospitals audited hospital charts of all consecutive suspected ACS patients, until 25 suspected cases of acute myocardial infarction had been admitted to intensive/coronary care. A total of 1365 episodes were recruited for this survey (935 suspected acute myocardial infarction and 430 contemporaneously admitted suspected other ACS). Data were collected on demographic and past clinical history, risk factors, admission details, acute treatments given and discharge status. Data were also collected on time to treatment, and data collectors approached eligible patients for consent to participate in a follow-up survey [13].
Statistical analysis
Data were analyzed using robust variance estimation methods with STATA/SE 8.0 to account for the clustering of patients within hospitals. Patients were grouped into two broad categories: those with a prior positive history of ACS or revascularization (acute myocardial infarction, unstable angina or previous coronary artery bypass surgery or PCI—ACS/revascularization group) (39%), and those without (61%). Logistic regression was conducted on each group to determine odds ratios (OR) for each event. Control variables were gender, age, having private health insurance, and total cholesterol. Insurance was originally analyzed as completely private cover, State-provided secondary care cover, or State-provided primary and secondary care cover. However, Wald test analysis after logistic regression determined that both State-provided insurance groups were similar, and insurance was subsequently analyzed as a dichotomous variable (i.e., having private health insurance or not). Due to significant gender differences in age, all data was age-adjusted, and data presented in tables was adjusted to age 65 years (to portray a ‘typical’ coronary patient).
Results
Baseline characteristics
Of the 1365 suspected ACS episodes, 386 (28%) were women. Mean age for men on intensive/coronary care admission was 63 years (SD = 13; range 20–100). Mean age for women, at 69 years (SD = 13, range 23–94) was significantly higher than that of men (t = 8.7, P < 0.001). Baseline characteristics of the sample are shown in Table 1.
Baseline characteristics of sample (age-adjusted to 65 years) (% unless otherwise stated)
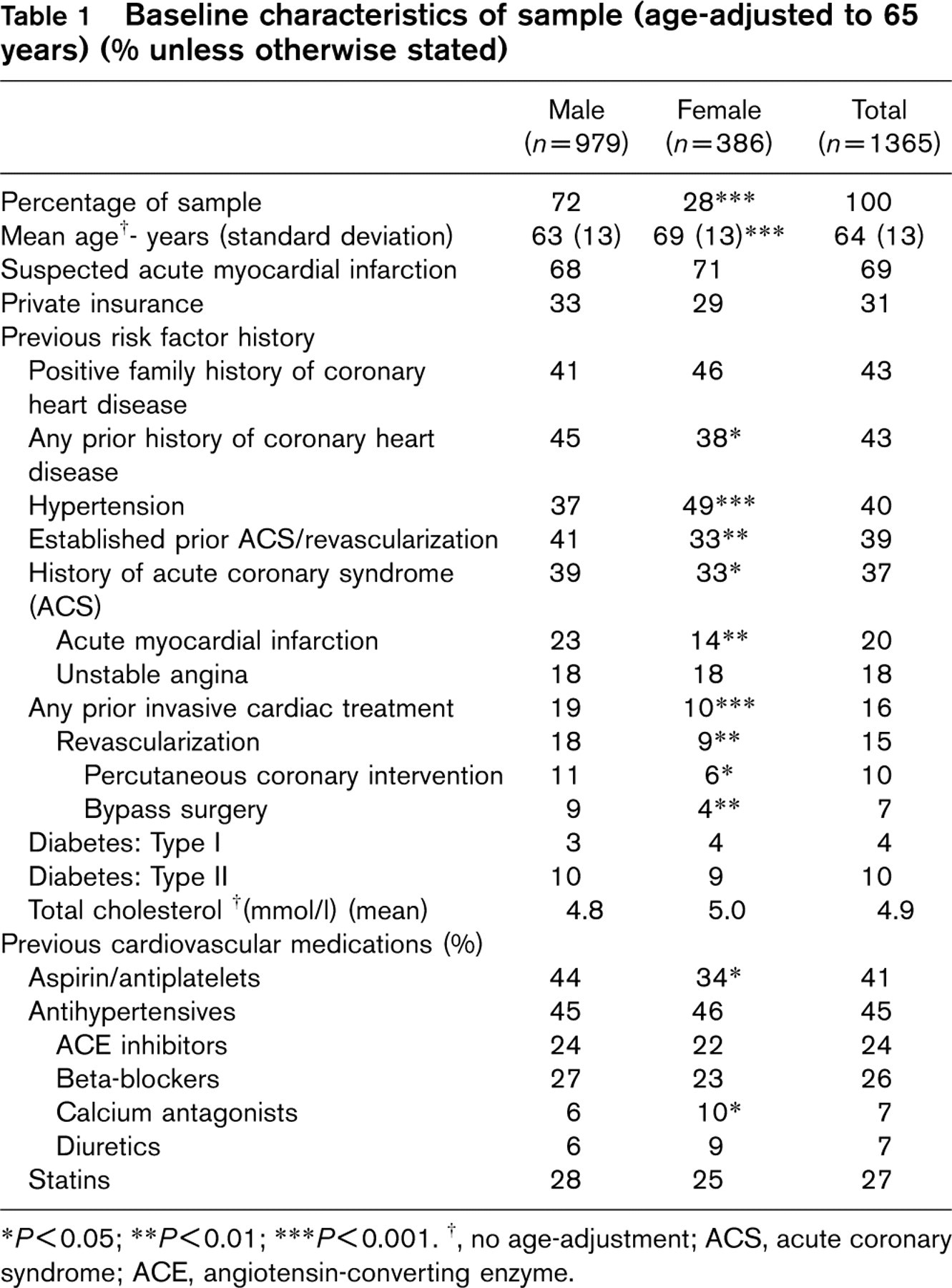
∗ P<0.05; ∗∗ P<0.01; ∗∗∗ P<0.001. †, no age-adjustment; ACS, acute coronary syndrome; ACE, angiotensin-converting enzyme.
A higher total cholesterol [OR = 1.30, 95% confidence interval (CI) 1.12–1.51] and older age of admission (OR = 1.03, 95% CI 1.02–1.05) were significant predictors of being admitted with suspected acute myocardial infarction as opposed to other ACS for men, but only age (OR = 1.04, 95% CI 1.02–1.06) was a significant predictor of admission with suspected acute myocardial infarction for women.
In terms of past history, women had a higher prevalence of hypertension (49 versus 37%), lower prevalence of any type of coronary heart disease (38 versus 45%), lower prevalence of prior acute myocardial infarction or prior ACS (14 versus 23% and 33 versus 39% respectively), and lower rates of prior revascularization (10 versus 19%) (i.e., significantly lower levels of bypass surgery [4 versus 9%] and PCI [6 versus 11%]). Overall, women were less likely to have established prior ACS/revascularization (33 versus 41%), and were less likely to be taking antiplatelet medication on index admission (34 versus 44%).
Although women had a significantly lower prevalence of prior ACS, this did not account for all the variation in prevalence of prior revascularization (PCI or bypass surgery). Using data from patients with prior ACS/vascularization (39%), a logistic regression model showed that the odds of having had revascularization prior to the current admission were statistically related to gender, age, private insurance status and total cholesterol level. Men with a history of ACS/revascularization were almost twice as likely as women to have had a previous revascularization when controlling for these other variables (OR 1.97, 95% CI 1.18–3.29, P = 0.011). For every year increase in age, a 4% decrease in the likelihood of having prior revascularization was seen (OR 0.96, 95% CI 0.93–0.98, P = 0.001). For every mmol/l unit increase in total cholesterol, patients were 27% less likely to have had revascularization (OR 0.73, 95% CI 0.58–0.93, P = 0.011). Patients with private health insurance were over twice as likely to receive revascularization than those without (OR = 2.02, 95% CI 1.29–3.19, P = 0.003). Results were similar when data for all invasive cardiac procedures were analyzed (data not shown).
Overall, no gender differences were seen for prior anti-hypertensive medication use (OR 0.95, 95% CI 0.71–1.3, P > 0.05) or for prior statin prescription (OR 1.18, 95% CI 0.93–1.48, P > 0.05). For patients with prior ACS/revascularization this finding was repeated: no differences for anti-hypertensive medication use (OR 1.03, 95% CI 0.61–1.74, P > 0.05) or statin use (OR 1.02, 95% CI 0.69–1.49, P > 0.05) by gender were seen on index admission.
Process of care and discharge details
The process of care received by gender is shown in Table 2. No gender differences were seen in acute-phase reperfusion (thrombolysis or direct PCI) (OR 0.96, 95% CI 0.76–1.24, P > 0.05) or acute antiplatelet therapy (OR 0.99, 95% CI 0.69–1.41, P > 0.05).
There was no gender difference in age-adjusted mortality rates (OR 0.85, 95% CI 0.59–1.24, P > 0.05). Similar percentages of men and women were discharged on anti-platelet (OR 1.04, 95% CI 0.76–1.43, P > 0.05) and anti-hypertensive medications (OR 1.09, 95% CI 0.76–1.57, P > 0.05). There were however, gender differences for lipid-lowering medication. The odds of being prescribed statins were 34% higher for men when controlling for age (OR 1.34, 95% CI 1.03–1.72, P = 0.027), and 35% higher when controlling for both age and total cholesterol (OR 1.35, 95% CI 1.01–1.81, P = 0.043). Translating these findings into a clinical example: a 65-year-old woman with a total cholesterol level of 5 mmol/l had a 76% chance of being prescribed a statin on intensive/coronary care discharge. A man of the same age and cholesterol level had an 81% (a 5% higher) chance of being prescribed a statin on discharge.
In-hospital process of care by gender for total sample (age-adjusted to 65 years) (%)
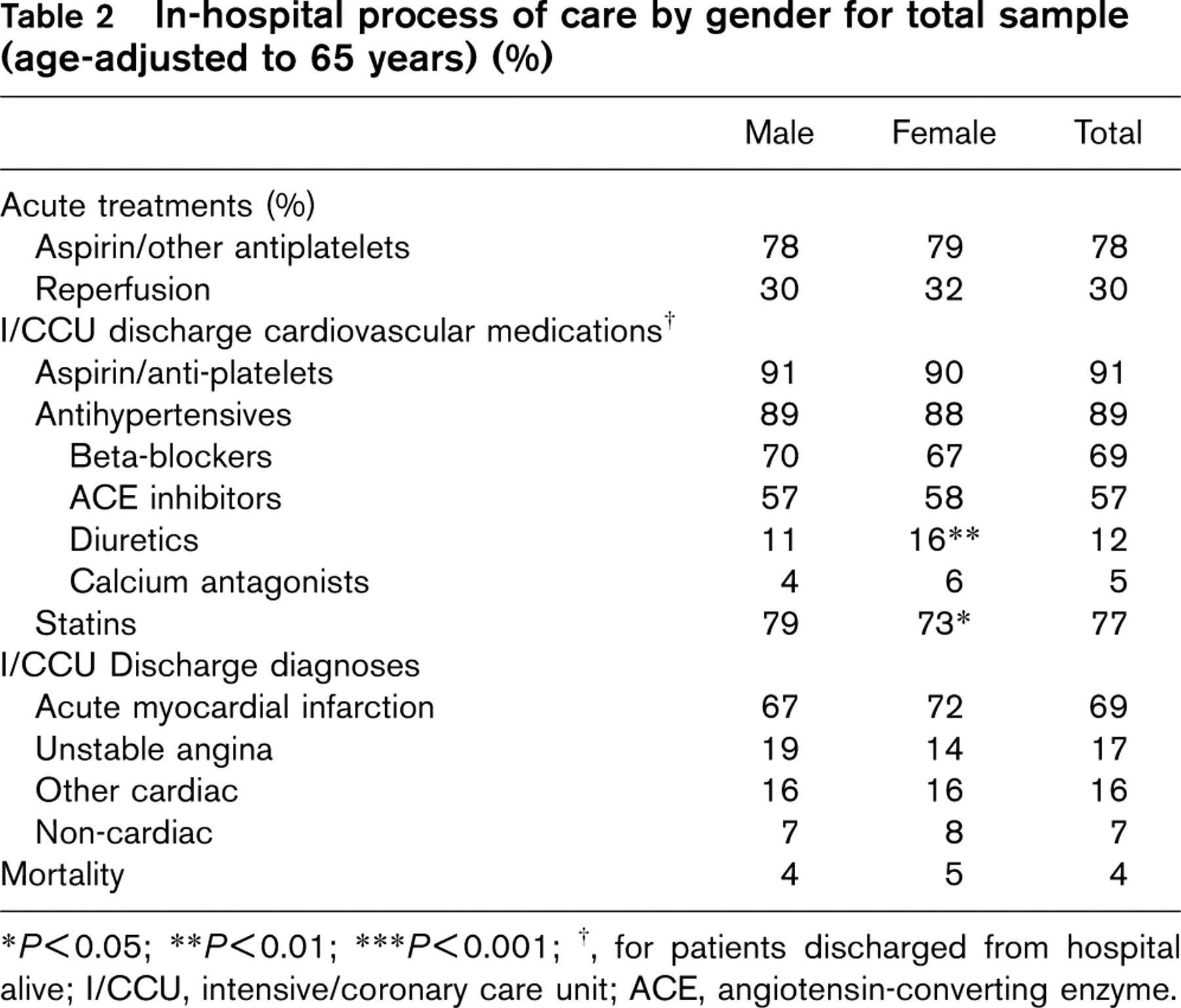
∗ P<0.05; ∗∗ P<0.01; ∗∗∗ P<0.001; †, for patients discharged from hospital alive; I/CCU, intensive/coronary care unit; ACE, angiotensin-converting enzyme.
Women with prior ACS/revascularization were also less likely to be prescribed statins on intensive/coronary care discharge than men with prior ACS/revascularization, when controlling for age and total cholesterol level (OR =1.94, 95% CI 1.02–3.71, P = 0.045). For a patient aged 65 with a total cholesterol level of 5mmol/l, this translated to an 86% chance a man would be prescribed statins, but only a 77% chance that a woman would be. However, women without prior ACS/revascularization on admission were just as likely to receive statins on discharge, as were men with no past history, when controlling for age and total cholesterol level (OR = 1.09, 95% CI 0.75–1.6, P > 0.05).
Discussion
The present survey evaluated the treatment of suspected ACS patients on a national level. It highlighted that men and women were treated differently in certain key aspects of care. Differences in treatments received by gender were seen both before the current hospitalization in patients with prior established coronary disease, and at discharge.
The first major finding in the current survey was that women with prior history of ACS/revascularization were less likely to have received revascularization prior to index admission. Men were almost twice as likely to have had prior revascularization when controlling for age, private insurance status and total cholesterol level. Indeed, men were also almost twice as likely as women to have had any form of invasive cardiac treatment (data not shown). Differential treatment by gender occurred when deciding whether a patient should undergo invasive cardiac treatment, even though the patients had already previously entered the healthcare system. This data replicates international findings on prevalence of revascularization rates between men and women [2–5, 8, 9]. It may be that the women in the present survey did not require revascularization, as their underlying disease could differ from their male counterparts [1, 4]. Therefore, although women received differing levels of treatment, it may not have been sub-optimal. However, this seems unlikely as data from those with a confirmed positive history of ACS/revascularization were analyzed. Older patients were also less likely to have received revascularization.
In terms of prescribed medications, there were no differences between genders in the rate of anti-hypertensive or lipid-lowering medication prescription prior to the current admission. This parity was also reflected in the acute care of patients, with similar numbers of men and women receiving both reperfusion therapy and antiplatelet therapy during the current admission. This finding compares well against other surveys, which have shown that women receive less acute reperfusion therapy than men [1, 10].
On intensive/coronary care discharge, similar proportions of men and women were prescribed antiplatelet and anti-hypertensive medications (although women received more diuretic medications). The levels prescribed compare well with the Euro Heart Survey [3]. However, women were significantly less likely to be prescribed lipid-lowering medications. For patients aged 65 with a total cholesterol level of 5 mmol/l, this translated into a 5% decreased chance of being prescribed statins for women. This reflects a significant disadvantage for women in secondary prevention. Given that lipid-lowering therapy reduces coronary heart disease mortality for women [11], and that it is recommended that all coronary heart disease patients be prescribed lipid-lowering medication regardless of total cholesterol level [12], this finding is of concern. Interestingly, for those who had no prior ACS/revascularization, women were just as likely as men to be prescribed statins. The differential treatment was only seen for women with a prior history of ACS/revascularization. Reasons for this are unknown, and this aspect requires further research.
In relation to gender, the present results show that some aspects of international guidelines are being adhered to (in this case reperfusion guidelines), whereas other aspects (statin prescription) have yet to be fully implemented. These findings, along with the findings of other similar research, where discrepancies in treatments between genders are seen [1–5, 8–10], need to be further discussed by Cardiology Societies at national and international level.
Conclusions
Overall, there is evidence of treatment bias in favour of men in this national sample of patients admitted to intensive/coronary care for suspected ACS. This is reflected in increased coronary interventions in men prior to the current acute admission, and in a higher rate of prescription of lipid-lowering medication on intensive/coronary care discharge. Encouragingly, there were no treatment differences in the acute phase of in-hospital treatment, with men and women receiving reperfusion and antiplatelet medications equally often. The extent to which these findings reflect differing onset patterns of coronary heart disease for men and women needs to be further investigated.
Footnotes
Acknowledgements
This project was funded by a grant from the cardiovascular strategy, Department of Health and Children.