
Abstract
Background Homocysteine and folate have been suggested to have opposite effects on the risk of stroke, although the results are controversial.
Design and methods The purpose of this study was to assess the effects of serum total homocysteine (tHcy) and serum folate levels on the risk of stroke in a prospective cohort study. The subjects were 1015 men aged 46–64 years and free of prior stroke, examined in 1991–1993 in the Kuopio Ischaemic Heart Disease Risk Factor (KIHD) Study.
Results At baseline the mean serum tHcy concentration was 10.9 μmol/l (SD 3.4). During an average follow-up time of 9.6 years, 49 men experienced a stroke, of which 34 were ischaemic. In Cox proportional hazards models, men in the highest tHcy third had a risk factor-adjusted hazard rate ratio (RR) of 2.77 [95% confidence interval (CI): 1.23–6.24] for any stroke and 2.61 (95% CI: 1.02–6.71) for ischaemic stroke, compared with men in the lowest third. The mean baseline serum folate concentration was 10.4 nmol/l (SD 4.1). Men in the highest third of serum folate (> 11.2 nmol/l) had an adjusted RR for any stroke of 0.35 (95% CI: 0.14–0.87) and for ischaemic stroke of 0.40 (95% CI: 0.15–1.09), compared with men in the lowest third.
Conclusion Elevated serum tHcy is associated with increased risk of all strokes and ischaemic strokes in middle-aged eastern Finnish men free of prior stroke. On the other hand, high serum folate concentration may protect against stroke.
Introduction
Stroke is one of the leading causes of morbidity and mortality in the developed countries. One of the proposed risk factors for stroke is serum homocysteine (Hcy), an intermediate amino acid produced during the metabolism of methionine. Four meta-analyses have suggested that serum total homocysteine (tHcy) concentration is a risk factor for cardiovascular diseases (CVD), including stroke [1–4], one suggesting that the association is causal [1].
Folate plays an important role as a methyl donor in the remethylation of Hcy back to methionine. This has raised interest in the role of folate in the prevention of CVD. Indeed, low serum or dietary folate is associated with increased serum tHcy concentration [5], and on the other hand, folate supplementation is an effective way to decrease serum tHcy [6]. Furthermore, there are several findings of an inverse relationship between dietary or serum folate and risk of stroke [7–9].
In this prospective cohort study we investigated the effects of serum tHcy and folate levels on the risk of all strokes and on ischaemic strokes in middle-aged men from eastern Finland. We also wanted to study whether the effect of tHcy on the risk of stroke is affected by serum folate concentration.
Methods
Study population
The Kuopio Ischaemic Heart Disease Risk Factor (KIHD) Study is an ongoing prospective population-based cohort study designed to investigate risk factors for CVD, atherosclerosis and related outcomes in middle-aged men from eastern Finland [10], the population with one of the highest recorded rates of coronary heart disease (CHD). A total of 2682 participants (82.9% of those eligible), aged 42, 48, 54, or 60 years, were enrolled in the study between 1984 and 1989. The baseline examinations for the present analysis were carried out during 1991–1993 at the 4-year re-examinations of the KIHD study. Out of the total of 1229 men eligible for the study, 52 had died, had had a severe illness, or had migrated from the region, and 139 could not be contacted or refused to participate. Thus, 1038 men were examined in 1991–1993, of which data on serum tHcy concentration was available for 1027 men. Men with a history of stroke (n = 12) were excluded, leaving 1015 men for the final analyses. Data on income was available for 996 men and on total physical activity for 1010 men. The population mean for these two variables was used to replace the missing values in statistical analyses.
Determination of serum tHcy concentration
The serum tHcy concentration was analyzed by high-performance liquid chromatography [11] with modifications described by Schwab et al. [12] in 2001 at the National Public Health Institute, Helsinki, Finland. The results represent total serum homocysteine, which is referred as serum tHcy. The coefficient of variation (CV) between batches (n=30) for two-pooled serum samples were 4.3 and 5.4% at levels 11.2 and 7.4 μmol/l, respectively. The mean bias in a quality-control program was 2.2% [12].
Determination of serum folate concentration
Serum folate concentration was measured by radioimmunoassay (Quantaphase II; Bio-Rad, Hercules, California, USA). Folate measurements were carried out in 1998 in serum samples collected during 1991–1993 and kept frozen at −80°C. The between-batch CV of quality control serum (Lyphochek Immunoassay Plus Control levels 1, 2, 3, Bio Rad Laboratories, ECS Division, Anaheim, California, USA) at levels 5.5, 13.4 and 23.6 nmol/l were 6.4, 6.7 and 6.7%, respectively (n = 16).
Other measurements
Assessment of medical history, smoking and alcohol consumption using both questionnaires and interviews, and assessment of blood pressure were carried out as described previously [13]. The collection of blood specimens and measurement of serum lipids and lipoproteins and plasma lycopene and beta-carotene have been described in detail elsewhere [13–15]. Physical activity in leisure time was assessed from a 12-month history, modified from the Minnesota leisure time physical activity questionnaire; the intensity of physical activity was expressed in metabolic equivalents of oxygen consumption [16]. The 12-month history gives a more accurate estimate of the past level of physical activity than shorter-term measurements [17]. Body mass index (BMI) was computed as the ratio of weight in kilograms to the square of height in metres.
Ascertainment of follow-up events
Incident strokes between 1984 and 1992 were ascertained through the FINMONICA stroke register [18]. Information on stroke incidence between 1993 and 31 December 2002 was obtained by computerized linkage to the Finnish national hospital discharge registry and death certificate registry. Diagnostic information was collected from hospitals and classified by a neurologist (J.S.) using diagnostic criteria identical to the FINMONICA criteria. The sources of information on stroke were from hospital documents, death certificates, autopsy reports, and medico-legal reports. The diagnosis of stroke was based on the sudden onset of clinical signs or focal or global disturbance of cerebral function lasting > 24 h (except in the case of sudden death or when interrupted by surgical intervention) with no apparent cause other than a vascular origin. Each suspected stroke (ICD-9 codes 430–439 and ICD-10 codes I60–I68 and G45–G46) was classified as: (1) definite stroke; (2) no stroke; or (3) an unclassifiable event. The data from the FINMONICA stroke register were annually rechecked with the data obtained from the computerized national hospital discharge and death registers. Definite strokes and unclassifiable events were included in the group of any stroke. Each definite stroke was classified as: (1) an ischaemic stroke (ICD-9 codes 433–434 or ICD-10 code I63); or (2) a haemorrhagic stroke (ICD-9 codes 430–431 or ICD-10 codes I60–I61). If the subject had multiple strokes during follow-up, the first event was considered the end point.
Statistical methods
The data are expressed as means ± SD. Means were compared with analysis of variance (ANOVA). Categorical variables were compared with the chi-square test. Correlations were estimated with Pearson correlation coefficients (r). Cox proportional hazards models were used to analyze the associations between serum tHcy or folate and incidence of stroke. Risk factor adjusted hazard rate ratios (RR) were estimated as the antilogarithms of coefficients from multivariable models. Systolic blood pressure, smoking, diabetes, body mass index (BMI), serum total and low-density lipoprotein (LDL) cholesterol, alcohol intake, history of ischaemic heart disease, income, and total physical activity were considered as confounders. These factors were eliminated from the full model if their joint removal did not result in a change of the tHcy RR of 10% or more. Age and examination year were forced in the models. Confidence intervals (CI) were estimated on the basis of the assumption of asymptotic normality of the estimates. All tests of significance were two-sided. Data were analyzed using SPSS 11.0 for Windows (SPSS Inc., Chicago, Illinois, USA).
Baseline characteristics of the 1015 study participants in thirds of the serum total homocysteine concentration
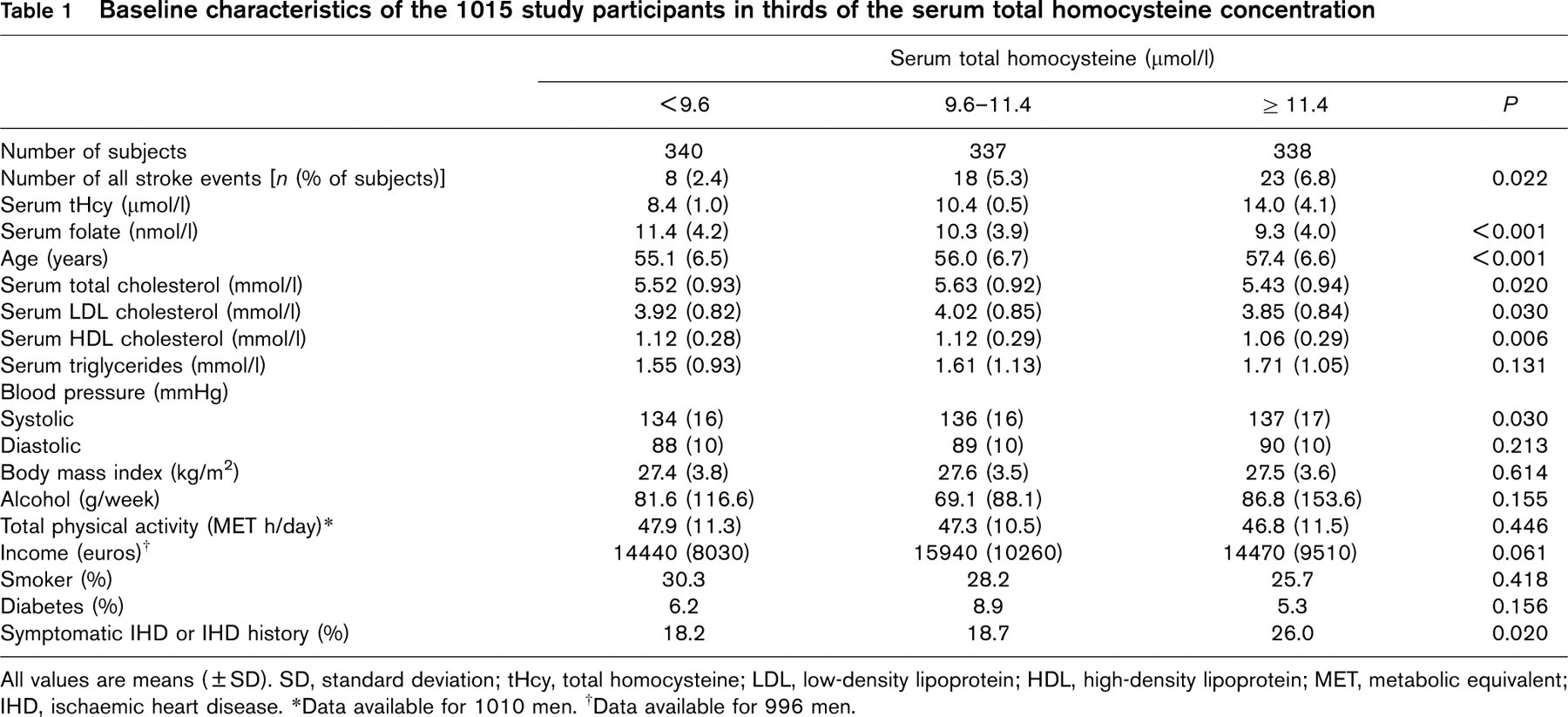
All values are means (± SD). SD, standard deviation; tHcy, total homocysteine; LDL, low-density lipoprotein; HDL, high-density lipoprotein; MET, metabolic equivalent; IHD, ischaemic heart disease.
∗ Data available for 1010 men.
† Data available for 996 men.
Results
At baseline the mean serum tHcy concentration was 10.9 μmol/l (SD 3.4, min–max 2.8–51.2 μmol/l). The men in the highest serum tHcy third were older, had lower serum folate and high-density lipoprotein (HDL) concentrations and higher triglyceride concentrations, higher systolic blood pressure and higher prevalence of symptomatic ischaemic heart disease or history of ischaemic heart disease compared to the lowest third (Table 1).
The mean serum folate concentration was 10.4 nmol/l (SD 4.1, min–max 2.3–40.5 nmol/l). The men in the highest serum folate third were younger and had higher total and HDL cholesterol and triglyceride concentrations and lower serum tHcy concentrations. They also had higher systolic and diastolic blood pressure, BMI and alcohol intake and were more physically active. In addition, they smoked less and had a higher prevalence of diabetes than men in the lowest third (Table 2).
During a mean follow-up time of 9.6 years (SD 2.2) 49 men experienced a stroke, of which 34 were ischaemic. The subjects were divided into thirds based on the serum tHcy concentration. The age and examination year adjusted RRs for any stroke in thirds of + Hcy were 1, 2.16 (95% CI: 0.94–4.96) and 2.77 (95% CI: 1.23–6.24), the P for linear trend across the thirds was 0.014. The age and examination year adjusted RRs for ischaemic stroke in thirds of + Hcy were 1, 1.71 (95% CI: 0.63–4.64) and 2.61 (95% CI: 1.02–6.71), the P for linear trend being 0.039. Additional adjustment for stroke risk factors (systolic blood pressure, smoking, diabetes, BMI, serum total and LDL cholesterol, alcohol intake, history of ischaemic heart disease, income, and total physical activity) or serum folate did not change the results. Figure 1a presents the age and examination year adjusted stroke survival curves for men in each serum tHcy third.
The age and examination year adjusted RRs for any stroke in the thirds of serum folate were 1, 1.04 (95% CI: 0.57–1.90) and 0.43 (95% CI: 0.18–1.05), the P for linear trend being 0.200. The respective RRs for ischaemic strokes were 1, 0.81 (95% CI: 0.38–1.72) and 0.49 (95% CI: 0.18– 1.31), the P for linear trend being 0.361. After additional adjustment for alcohol intake and diabetes the RRs for any stroke were 1, 1.00 (95% CI 0.55–1.83) and 0.35 (95% CI: 0.14–0.87), with a P for linear trend being 0.046. The RRs for ischaemic stroke were 1, 0.79 (95% CI 0.37–1.68) and 0.40 (95% CI: 0.15–1.09), with a P for linear trend being 0.117, after additional adjustment for serum LDL cholesterol and diabetes. Further adjustment for other risk factors (systolic blood pressure, smoking, diabetes, BMI, serum total and LDL cholesterol, alcohol intake, history of ischaemic heart disease, income, and total physical activity) and serum tHcy did not change the results. Neither did adjustment for plasma lycopene and beta-carotene. Figure 1b presents the age, examination year, alcohol intake and diabetes adjusted stroke survival curves for men in each serum folate third.
Baseline characteristics of the 1015 study participants in thirds of the serum folate concentration

All values are means (± SD). SD, standard deviation; tHcy, total homocysteine; LDL, low-density lipoprotein; HDL, high-density lipoprotein; MET, metabolic equivalent; IHD, ischemic heart disease.
∗ Data available for 1010 men.
† Data available for 996 men.
The RRs according to serum tHcy and folate medians were also determined. The risks of any stroke and ischaemic stroke were increased in the group of men with both elevated serum tHcy and low serum folate concentrations compared with the group of men with low serum tHcy and high serum folate (Table 3). No significant increase in risk was observed in men with elevated serum tHcy when serum folate was above median (group 3). The correlation between serum tHcy and serum folate was −0.15 (P < 0.001).
Discussion
The main finding of this prospective cohort study was that high serum tHcy concentration may increase and high serum folate concentration may decrease the risk of any stroke and ischaemic stroke in middle-aged men from eastern Finland who were free of previous stroke at baseline.
There are some limitations in our study. First, the number of events was relatively low, which also prevented us from studying the risks of haemorrhagic strokes separately. Secondly, serum folate was used instead of dietary folate and although serum and dietary folate are well correlated, serum folate may not be a good indicator of long-term dietary intake. Unfortunately dietary intakes were not assessed at the baseline for this study and neither was red cell folate, which is considered to be a marker of long-term folate status [19]. Finally, since folate is found mainly in foodstuffs of plant origin, other nutrients may also contribute to the benefit. However, plasma levels of lycopene and beta-carotene, also markers of a healthy diet, did not attenuate the beneficial effect of folate.
There are several meta-analyses concerning the association between high blood tHcy concentration and increased risk of stroke [1–4]. In one meta-analysis the association has been suggested to be causal; the authors conclude that lowering tHcy concentrations by 3 μmol/l from current levels would reduce the risk of stroke by 19–24% [1]. Another meta-analysis suggested a 19% reduction in stroke risk with the same 3 μmol/l lowering of tHcy concentration [2]. This reduction in tHcy would be achievable by increasing folate intake [20, 21]. In two previous Finnish nested case–control studies the results have been inconsistent [22, 23]. A recent study of 201 cerebral infarction cases and 201 controls of the cohort of 13 840 male smokers free of CVD of the Alpha-Tocopherol and Beta-Carotene (ATBC) Cancer Prevention study found a graded increase in the odds ratio (OR) of cerebral infarction per quarter increase in tHcy concentration [22]. In these 50- to 69-year-old men the adjusted OR in the highest quarter compared with lowest quarter was 2.1 (95% CI: 1.1–3.9). In contrast, in the earlier study of 42 male and 32 female stroke cases between 40 and 64 years of age and without prior CVD of a total study population of 7048, no association was found between tHcy and risk of stroke in either gender [23]. The authors of the ATBC study consider this discrepancy to be due to the relatively low mean and range of tHcy in the other Finnish study compared to their study or interaction between smoking and tHcy [22]. Differences in the mean tHcy levels, although small, could also explain part of the inconsistency with our study and the earlier study [23].
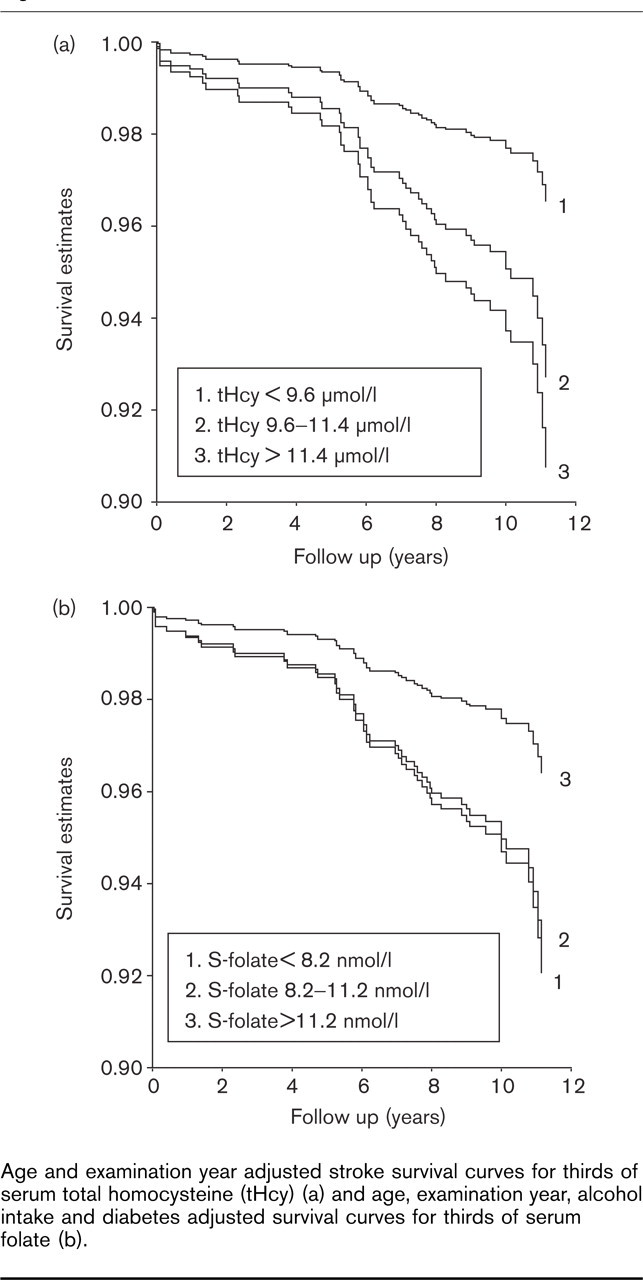
Age and examination year adjusted stroke survival curves for thirds of serum total homocysteine (tHcy) (a) and age, examination year, alcohol intake and diabetes adjusted survival curves for thirds of serum folate (b).
In our previous study in this same study population tHcy was not associated with acute coronary events [24, 25]. This may be due to different mechanism(s) by which Hcy induces stroke compared to acute coronary disease. Also, the smaller diameter of cerebral arterioles may make them more susceptible to oxidative damage, which has been proposed as one mechanism by which Hcy induces its negative effects, in addition to induction of endothelial injury [26]. However, the mechanisms are not completely understood.
High serum folate concentration, on the other hand, was associated with lower risk of stroke, which is in line with previous studies that have studied either serum or dietary folate [7–9]. Furthermore, if serum folate levels were above the median, tHcy did not increase the risk of stroke. Neither did addition of tHcy as a covariate in the folate models. This could suggest that folate may be beneficial independently of tHcy concentration, which has also been reported before [27, 28]. As is the case with Hcy, the mechanisms behind folate's beneficial effects are still unclear. There is, however, some evidence that folic acid or its metabolite 5-methyltetrahydrofolate may directly improve endothelial function, possibly by reversing endothelial dysfunction and reducing plaque size/growth [29]. In our previous studies serum folate has also been associated with greatly reduced incidence of acute coronary events [25, 30], suggesting a systemic protective effect of folate against CVD. On the other hand, a recent randomized controlled trial failed to find an effect on recurrent stroke, CHD events or death after high-dose vitamin therapy (folic acid, B6, B12) compared with low-dose vitamin therapy during the 2 years of follow-up in patients with non-disabling cerebral infarction [31]. The mean reduction of tHcy in the high-dose group was 2 μmol/l greater than in the low-dose group. They however found a persistent and graded association between baseline tHcy and outcomes. As the authors commented, the follow-up time may have been too short to find an effect. Also, the coincided folic acid fortification of the US grain supply with the initiation of the trial probably had reduced the prevalence of low folate and high tHcy levels, persons who might have been most likely to benefit [31]. Thus, trials using different populations and a longer follow-up time are needed to clarify whether tHcy is an independent risk factor or only a marker for CVD and whether folate has a beneficial impact independent of blood tHcy concentration, as has been suggested [27, 28]. Several such trials are currently underway [32]. Unfortunately the two other large trials in North America designed to investigate the effects of folic acid and other B vitamins on cardiovascular outcomes are also affected by the folic acid fortification, which may reduce the statistical power to detect any effects of vitamin supplementation [33]. In the Finnish study populations the range of serum folate is large, thus increasing the power to find associations between folate and risk of events. Furthermore, there are no folate fortification programmes in Finland.
In conclusion, this study suggests that: (1) elevated serum tHcy concentration may increase the risk of stroke; and (2) high serum folate concentration may protect against stroke in middle-aged Finnish men without prior stroke. The results from the ongoing trials may show whether supplementation with folic acid is beneficial against CVD.
Hazard rate ratios according to the serum total homocysteine and folate medians
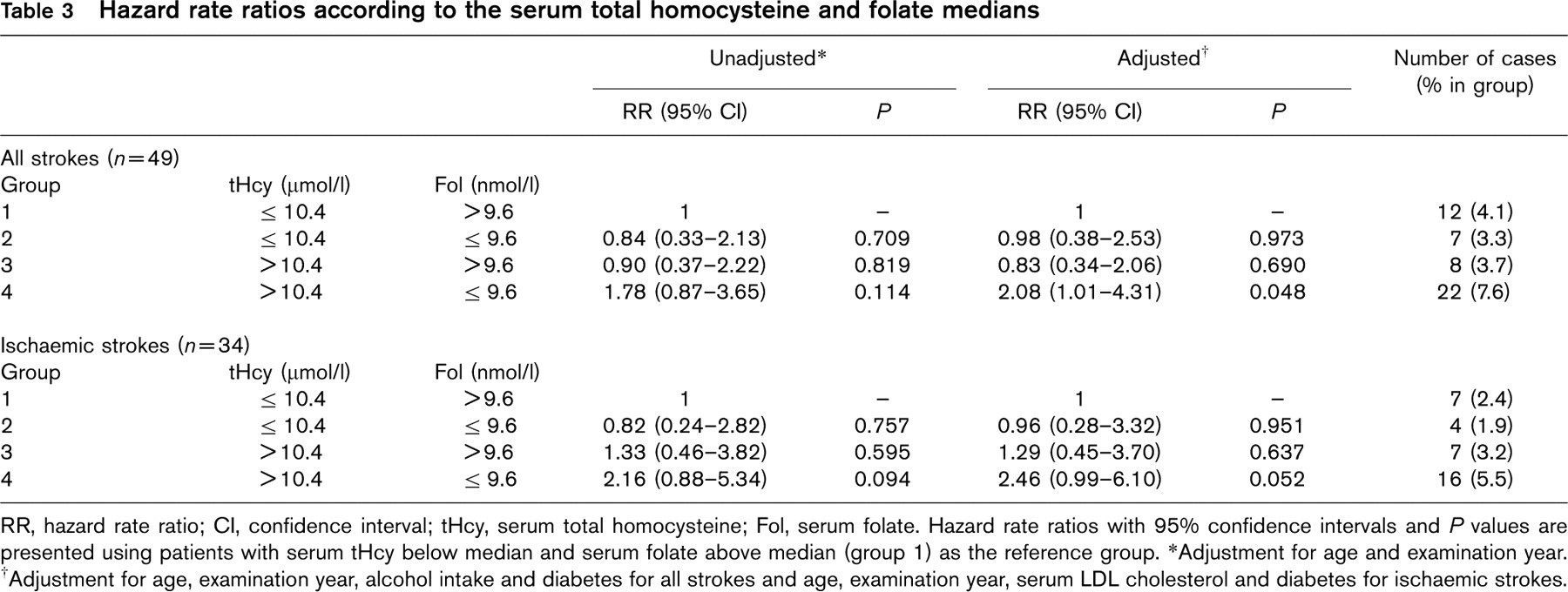
RR, hazard rate ratio; CI, confidence interval; tHcy, serum total homocysteine; Fol, serum folate. Hazard rate ratios with 95% confidence intervals and P values are presented using patients with serum tHcy below median and serum folate above median (group 1) as the reference group.
∗ Adjustment for age and examination year.
† Adjustment for age, examination year, alcohol intake and diabetes for all strokes and age, examination year, serum LDL cholesterol and diabetes for ischaemic strokes.
Footnotes
Acknowledgements
We thank our staff for helping with data collection. This study was presented in part as a poster at the American Heart Association's 44th Annual Conference on Cardiovascular Disease Epidemiology and Prevention in San Francisco, USA, 3–6 March 2004. This work was supported by grants from the Academy of Finland, Helsinki, Finland (grants 41471, 1041086 and 2041022 for J.T.S. and grants 201688 and 80185 for S.V.), the Yrjö Jahnsson Foundation, the Juho Vainio Foundation, the Finnish Cultural Foundation and the Finnish Foundation for Cardiovascular Research (for J.K.V.).