
Abstract
Background Variation of plasma total homocysteine (tHcy) levels among individuals is modified by 5,10-methylenetetrahydrofolate reductase (MTHFR) genotypes and selected atherosclerotic risk factors.
Design Cross-sectional study.
Methods Healthy Japanese men (n = 213) and women (n = 242) aged 40–69 years were examined.
Results Serum uric acid, hemoglobin, hematocrit, serum creatinine, and men were independently significantly associated with plasma tHcy. The relationship between serum uric acid and plasma tHcy was the strongest in those with the mutant homozygote (VV), but the overall statistical test of interaction was not significant.
Conclusions Serum uric acid, hematocrit, hemoglobin, creatinine, and men were determinants of plasma tHcy levels.
Further investigations are needed.
Introduction
Several epidemiological studies have reported that elevated plasma tHcy is an independent risk factor for atherosclerotic thrombotic vascular diseases [1]. A mutation of the 5,10-methylenetetrahydrofolate reductase (C677T MTHFR) gene is well known to increase plasma tHcy levels [1, 2]. Notably, this mutation modifies the relationships between plasma tHcy and several modifiable factors such as serum folate, vitamin B12 [1, 2], and uric acid concentrations [3], indicating a so-called gene–environment interaction. Since these factors are also related to other factors (e.g., alcohol drinking, smoking, and hematological variables) [4], we analyzed the relationships of selected atherosclerotic risk factors (age, sex, uric acid, hematocrit, hemoglobin, and creatinine) with plasma tHcy concentration considering the potential modification effects of the C677T MTHFR polymorphism.
Methods and materials
The participants (213 men and 242 women) were randomly selected from all residents aged 40–69 years in Shiso county, Japan in 2000. The assessment of lifestyle factors, blood collection, biochemical analyses, and MTHFR genotyping were previously described [2]. A written informed consent was obtained from all participants and the study was approved by the ethics review committees of National Institute of Health and Nutrition (NIHN), and Tokyo Medical and Dental University, Japan.
Statistical methods
All variables showing non-Gaussian distribution were logarithmically transformed. Mann–Whitney U-test, analysis of covariance and a multiple linear regression analysis were performed by using the SAS 8.2 software (SAS Institute, Cary, North Carolina, USA).
Results
Mean ± SD of age was 53.7 ± 8.6 years. The medium value of plasma tHcy was 11.1 μmol/l and those were significantly higher in men than in women (12.9 and 9.5 μmol/l, respectively; P < 0.0001 by U-test). The frequency of the mutant allele (V) in men was 0.42, and in women it was 0.38. The frequencies of the MTHFR AA, AV, and VV genotypes were 31.9, 52.1, and 16.0% in men, respectively, whereas it was 36.3, 50.8, and 12.9% in women, respectively, and the genotype distributions were in Hardy–Weinberg equilibrium.
Serum uric acid, hematocrit, hemoglobin, and serum creatinine were positively associated with plasma tHcy independently of age and sex (Table 1). Of these, the positive relationships between serum uric acid and plasma tHcy were 2.5- and 4-fold steeper in those with AV (standardized regression coefficient ± SE = 0.15 ± 0.06) and VV (0.25 ± 0.10) genotypes than in those with AA genotype (0.06 ± 0.05), respectively, even after multivariate adjustment for known confounding factors [age, sex, serum folate, serum vitamin B12, body mass index (BMI), and serum creatinine], suggesting a so-called gene–environment interaction, but the overall statistical test of interaction was not significant (P = 0.11). The positive associations of hematocrit, hemoglobin, and serum creatinine with plasma tHcy were observed in each genotype, but no differences for these associations among the three genotypes were found.
Discussion
Our study showed a significant association between serum uric acid and plasma tHcy levels in all subjects. The association was only significant and strongest in the homozygous mutant (VV) genotype after adjustment for known confounding factors. This result was approximately compatible with Motti et al. [3] who reported a significantly stronger relationship between uric acid and plasma tHcy level in those with VV genotype than in those with AA and AV genotypes. Our result was the first report for adult healthy subjects in a Japanese population. Although the underlying mechanism is still obscured, adenosine originating from S-adenosyl-homocysteine could represent a link between the homocysteine and uric acid metabolic pathway, and the MTHFR mutation could involve this mechanism such as the de novo synthesis of purines [3, 4]. A reduced intake of purinerich foods could prevent hyperuricemia and hyperhomocysteinemia.
Associations between blood biochemical variables and plasma tHcy level
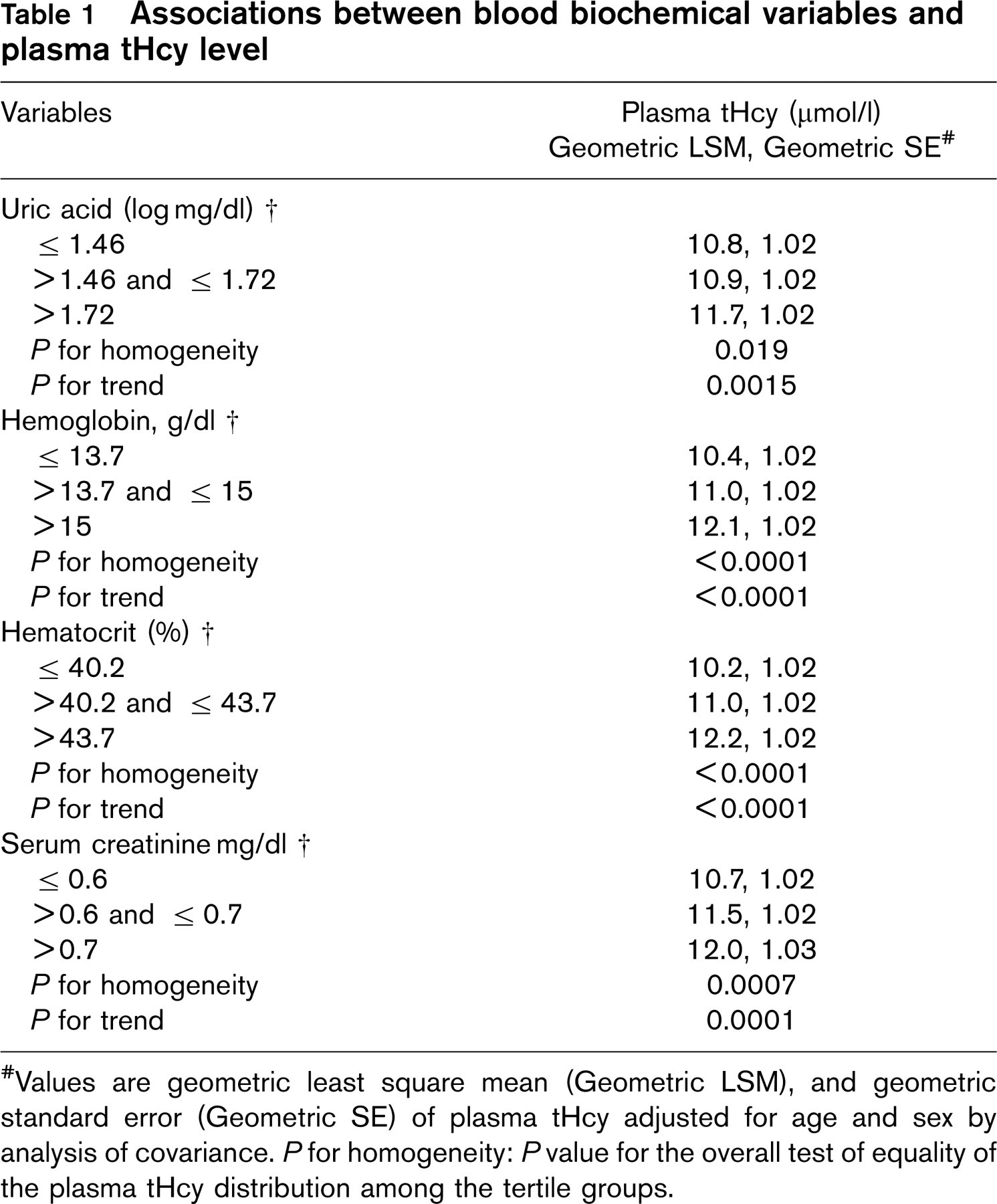
# Values are geometric least square mean (Geometric LSM), and geometric standard error (Geometric SE) of plasma tHcy adjusted for age and sex by analysis of covariance. P for homogeneity: P value for the overall test of equality of the plasma tHcy distribution among the tertile groups.
The hematocrit, hemoglobin, and serum creatinine were significantly associated with plasma tHcy in each genotype. Although such findings have not previously been reported in Japanese, the results are compatible with the other study [4]. The mechanisms involved are still not known. Smoking status was encountered in the determination of hemoglobin and hematocrit levels, and renal homocysteine excretion was also important for the determination of tHcy concentration. The plasma tHcy was strongly significantly associated with sex (men). It may be explained by BMI, smoking status, and lifestyle-related factors (serum folate and vitamin B12 levels) [1, 2], and smoking status in men was significantly associated with plasma tHcy (r = 0.20, P = 0.0041). We should emphasize on monitoring the recent preventive measure for smoking and body weight control.
In conclusion, men, serum uric acid, serum creatinine, blood hemoglobin, and hematocrit were determinants of plasma tHcy levels. In addition, the interaction of serum uric acid and the MTHFR mutation may influence the variation of plasma tHcy in this population. Our findings need further investigation.
Footnotes
Acknowledgements
Thanks to all participants in Shiso County, NIHN, Japan, and JSPS. We offer special thanks to Dr. Kazue Yamaoka, NIPH, Japan, for her helpful suggestions for statistical analysis. This study was supported by a grant-in-aid for General Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology of Japan; National Cardiovascular Centre Grant-in-aid; Japan Heart Foundation Grants, and Japan Society for the Promotion of Science (JSPS).