
Abstract
Background Stroke represents worldwide the second and seventh cause of death and invalidity, respectively. Patients with ischaemic stroke or transitory ischaemic attack (TIA) are at high risk of recurrence, therefore requiring intensive treatment. Hypercholesterolaemia is a modifiable risk factor for stroke. The general practitioners attitude towards detection and treatment of dyslipidaemia among patients with stroke or TIA in Italy is unknown; we therefore aimed to address this issue taking advantage of the database of The Italian College of General Practitioners.
Methods Prevalence of the monitored factors (lipid levels, statin prescription, and lipid level control with hypolipidaemic agents prescription) were analysed on a patient population of 465 061.
Results A total of 2555 (49% women and 51% men) patients with a diagnosis of stroke and 2755 patients (52% women and 48% men) with a diagnosis of TIA were included in the study. Total plasma cholesterol (TC) was reported in more than 60% of the patients and low-density lipoprotein cholesterol (LDLc) and high-density lipoprotein cholesterol (HDLc) in less than half. Total plasma cholesterol and LDLc were controlled in 70.3 and 72.8% of the patients, respectively. The percentage of controlled patients decreased to 64% when both LDLc and TC were considered. Statins and fibrates were prescribed in a small proportion of patients (16.9 and 3.5%, respectively). An acceptable control of blood lipids was achieved in a majority of those patients (60.2%). However a relatively large number of patients (646) with high plasma lipids remained untreated. Conclusions Monitoring and intervention strategies on plasma lipid levels in patients with a diagnosis of stroke or TIA need to be improved. Eur J Cardiovasc Prev Rehabil 12: 159–163 © 2005 The European Society of Cardiology
Introduction
Stroke represents worldwide the second cause of death, and the seventh cause of invalidity [1]. In Italy, stroke represents the third cause of mortality and the first cause of disability [2]. Furthermore patients who experienced ischaemic stroke or transitory ischaemic attack (TIA) are at high risk of recurrence [1, 2].
Ischaemic stroke and coronary heart disease (CHD) share common risk factors, which lead to arterial damage and alter vascular morphology and function. The intima–media thickness (IMT) of carotid arteries is a strong predictor of both stroke and CHD, and an association between IMT and plasma low-density lipoprotein (LDL) cholesterol (LDLc) exists [3]. In a meta-analysis of 45 cohorts with about 13 000 cases of cerebrovascular events, however, no clear correlation between blood cholesterol levels and cerebrovascular events was observed [4]. This discrepancy may result from two opposite trends: a positive association between hyperlipidaemia and ischaemic stroke and an inverse relationship between cholesterol levels and haemorrhagic stroke [5]. Large secondary prevention trials with 3-hydroxy-3-methylglutaryl coenzyme A (HMG CoA)-reductase inhibitors consistently found a significant reduction of ischaemic stroke [6] and this finding was recently confirmed in the Heart Protection Study [7]. Furthermore, increased high-density lipoprotein cholesterol (HDLc) levels are associated with a significant decrease of ischaemic stroke [8]; it has been suggested that hypolipidaemic treatment reduces stroke and/or TIA incidence after myocardial infarction by increasing HDLc levels [9].
An overview of randomized trials including more than 36 000 patients treated with hypolidaemic, non-statin drugs, found no benefit of cholesterol lowering on the risk of ischaemic stroke [10]. More recently, a meta-analysis of 38 major trials, including more than 83 000 patients, suggested that lipid-lowering therapy effectively reduces strokes, independent of the type of drugs used, but dependent on the degree of plasma lipid reduction [11].
Italian guidelines recommend aggressive control of plasma LDLc in patients with atherosclerotic stroke [12] and elevated plasma lipids are among modifiable risk factors in the Statement for Healthcare Professionals from the Stroke Council of the American Heart Association [13].
The present study was primarily aimed at describing the knowledge of plasma lipid levels in patients with a diagnosis of stroke and TIA by general practitioners, and the degree of control of plasma lipid levels in these subjects. To this end data were extracted from the Health Search Database of the Italian College of General Practitioners.
Methods
Data source
Data were obtained from the Health Search Database (HSD) of the Italian College of General Practitioners (SIMG). The HSD currently contains information from over 550 GPs selected to observe a representative sample of the whole Italian population with over 800 000 patients recorded.
Participating GPs use the same software to enter data during their daily practice and periodically send anonymous records of their patients, which include all the recorded clinical data since the patient registered with his GP.
The information recorded includes patient demographics, medical diagnosis coded according to the International Classification of Diseases, ninth edition (ICD-9), drug prescriptions coded according to the ACC system, hospital referrals, and diagnostic investigations.
Data are subjected to a number of quality checks, such as weekly number of office visits, completeness of prescription records, drug prescription linked to medical diagnosis, and completeness of mortality records. Data from physicians failing to meet standard quality criteria are not considered for analysis.
Patient selection
In this study we considered 318 GPs with a patient population of 465 061 individuals. This sample is homogeneously distributed nationwide and is representative of the Italian population, according to the data of The National Institute of Statistics [14].
We selected the cases with a coded diagnosis of stroke (ICD-9 codes: 434.9, 438, 438.0, 342, 342.0, 342.1, and 342.9) or encoded as ‘stroke', ‘hemiparesis', or ‘hemiplegia’ present in HSD on 31 December 2001; ICD-9 diagnosis related to haemorrhagic stroke were not included. We also selected patients with a diagnosis of TIA (ICD-9 codes: 435).
Overall, 2555 stroke cases and 2755 TIA were identified (all with a coded ICD-9 diagnosis). For each patient age, gender, year of first-ever event, presence of concurrent diseases [i.e. diabetes, myocardial infarction (MI), atrial fibrillation], certified total invalidity, systolic blood pressure (SBP), diastolic blood pressure (DBP), total plasma cholesterol (TC), HDLc, and plasma triglycerides (TG) were obtained. Low-density lipoprotein cholesterol was computed with the Friedewald formula [14, 15] for TG values not exceeding 400 mg/dl. Information on established therapies (therapies prescribed at least twice in the last 6 months) with hypolipidaemic drugs, either statins or fibrates.
Blood lipid control was classified according to the guidelines suggested by the Italian Ministry of Health at the time of the query. The following categories were used (mg/dl): (1) optimally controlled: TC < 200 and/or LDL < 130; (2) acceptably controlled: TC between 200–239 and/or LDL between 130–159; (3) uncontrolled: TC between 240–289 and/or LDL between 160–189; (4) unacceptably uncontrolled: TC ≥ 290 and/or LDL ≥ 190.
Statistical analysis
Prevalence of the monitored factors was evaluated by means of the uncorrected chi-square test to ensure power uniformity. Continuous variables were compared when needed with either the unpaired t-test or the univariate ANOVA. Statistical analysis was performed by using SPSS v. 10.1 (SPSS Inc., Chicago, Illinois, USA).
Results
Sample characteristics
In total, 2555 patients (49% women and 51% men) with stroke and 2755 patients (52% women and 48% men) with TIA were included in the study (Table 1); all had one of the coded diagnoses (ICD-9 codes: 434. 9, 438, 438.0, 342, 342.0, 342.1, 342.9 and 435). Mean age was 73.4 ± 12.2 years and did not differ between stroke and TIA patients.
A number of concomitant diseases and/or risk factors, such as smoking habits, diabetes, atrial fibrillation or MI, were also analysed. The prevalence of known current smokers was quite low (13.1%), with a sizeable proportion of ex-smokers (32.2%). Diabetes represented the most frequent concurrent disease and the prevalence was higher among stroke patients (Table 1). Atrial fibrillation and MI were detected in concomitance with stroke or TIA in 10.5 and 5.3% of patients, respectively, and the prevalence was similar among stroke and TIA patients (Table 1). The evaluation according to the type of disease is also reported in Table 1.
Lipid profile
The lipid profile data with mean values for TC, LDLc, HDLc and TG are reported in Table 1. Low-density lipoprotein cholesterol and HDLc were not recorded in more than half of the stroke/TIA patients, whereas TC was reported for a greater number of patients (Table 2). Missing information ranged from 68.4% (LDLc in patients with stroke) to 35.3% (TC in patients with TIA). Overall, data on lipid profile was most frequently missing among patients with stroke (Table 2).
Main demographic and clinical characteristics of the sample
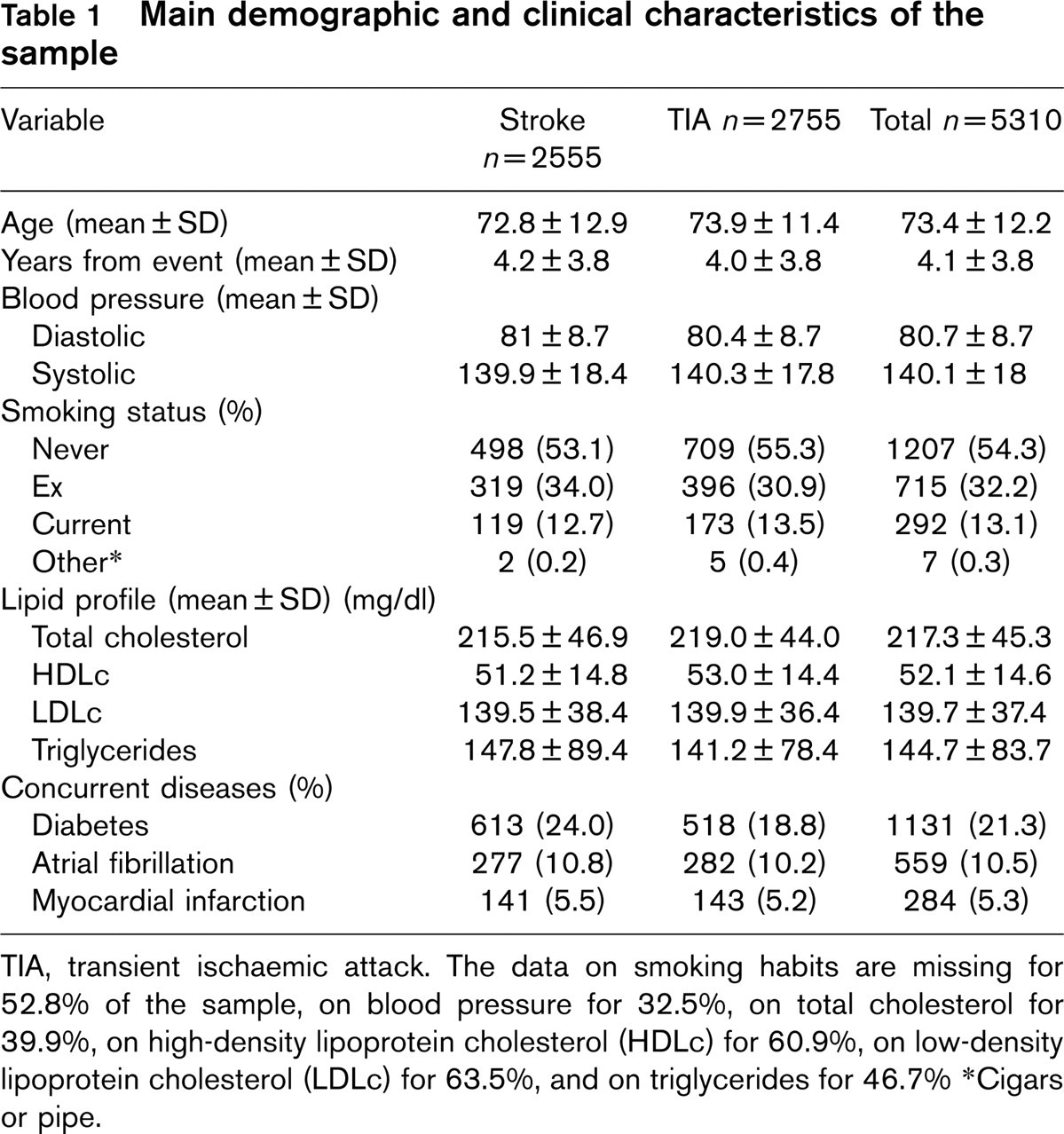
TIA, transient ischaemic attack. The data on smoking habits are missing for 52.8% of the sample, on blood pressure for 32.5%, on total cholesterol for 39.9%, on high-density lipoprotein cholesterol (HDLc) for 60.9%, on low-density lipoprotein cholesterol (LDLc) for 63.5%, and on triglycerides for 46.7%
∗Cigars or pipe.
Degree of lipid control
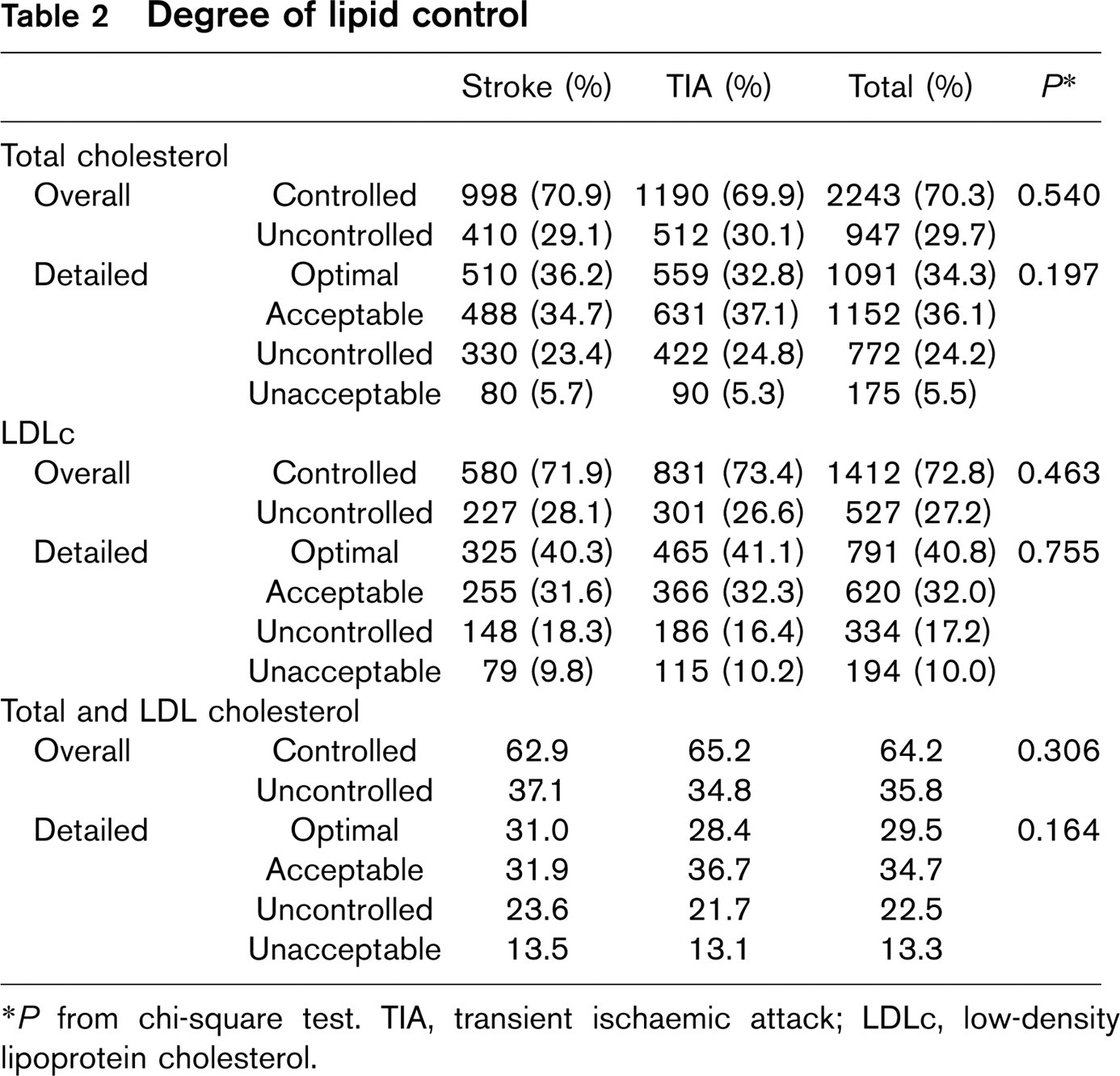
∗ P from chi-square test. TIA, transient ischaemic attack; LDLc, low-density lipoprotein cholesterol.
Lipid values (mg/dl; mean±SD) in patients not treated with statins, treated with statins, and those requiring treatment
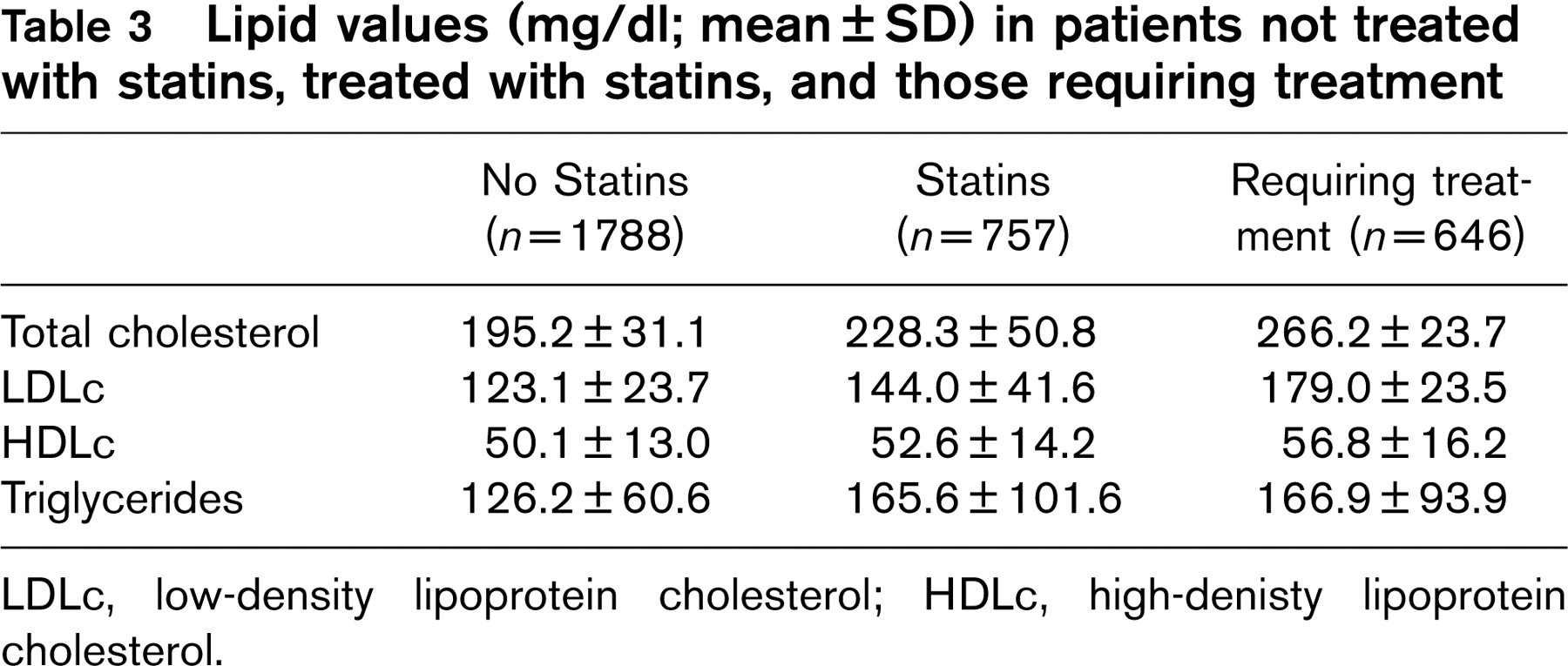
LDLc, low-density lipoprotein cholesterol; HDLc, high-denisty lipoprotein cholesterol.
When plasma lipid control was evaluated according to the previously mentioned criteria, TC and LDLc were controlled in 70.3 and 72.8% of the patients, respectively (Table 2). The percentage of controlled patients decreased to 64% when both LDLc and TC were considered (Table 2). Uncontrolled patients were 22.5% and unacceptably controlled 13.3%. The level of control by diagnosis of stroke or TIA did not differ (Table 2).
Use of HMG CoA-reductase inhibitors and fibrates
The majority of our patients (1788, 56.0%) did not qualify for drug therapy according to their lipid values; 757 (23.7%) were prescribed with statins; 646 (20.3%) deserved treatment, but were not prescribed with statins; the mean lipid level values of these three groups are summarized in Table 3.
Statins were prescribed in a small proportion of patients (16.9%). Lipids were controlled in the majority of those patients (60.2%). However, statin prescription was not associated with a higher number of patients controlled versus untreated patients (60.2 versus 73.5%).
The quality of this control (ranked from optimal to unacceptable) was significantly lower in the statin group. Only 28.3% were optimally controlled as compared to 36.1% in untreated patients (Table 4). Furthermore, 39.8% of the patients treated with statins did not reach target cholesterol levels and, therefore, should have been treated more aggressively (Table 4).
Lipid control by statins in patients with stroke or transient ischaemic attack
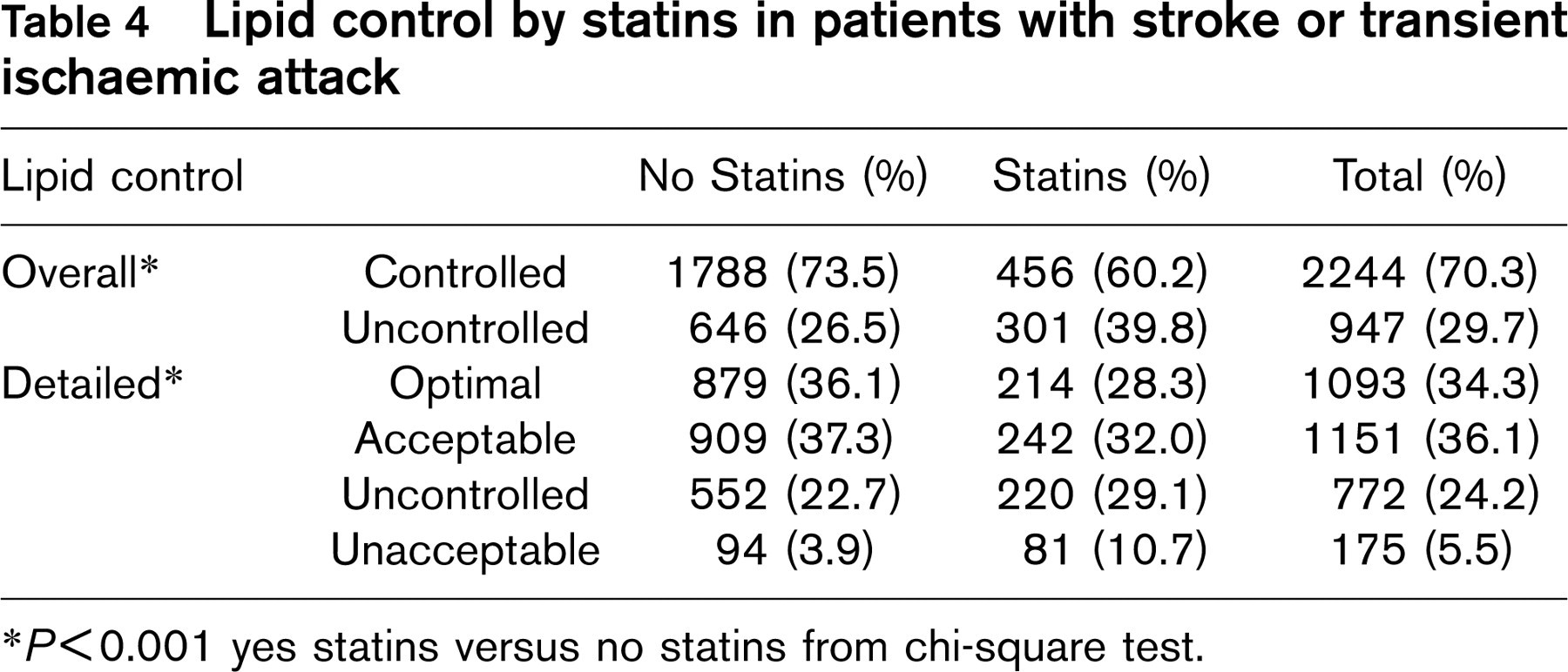
∗ P<0.001 yes statins versus no statins from chi-square test.
The presence of MI did not modify the general pattern of lipid control. It should also be observed that stroke patients with MI were generally less well controlled for lipid profile (TC, LDLc, HDLc) than TIA patients with MI (not shown). This finding suggests that the presence of CHD prompts the initiation of cholesterol-lowering therapy, but probably the GPs treat only those patients whose life expectancy and/or quality is less impaired.
Discussion
Control and management of the risk factors represents a fundamental approach to avoid recurrence of cardiovascular events, including stroke [2, 13, 16, 17].
The risk of recurrence of stroke and TIA is quite high, ranging from 7–15% in the first year and 4–9% per year during the following 5 years [2]. Therefore, interventions aimed at reducing the risk of recurrence of events are required. Lowering of plasma lipid levels effectively prevents the occurrence of stroke and TIA [6, 7, 18, 19, 20]; national and international guidelines recommend aggressive lipid-lowering treatment in atherosclerotic stroke [12, 21].
In the present study we addressed how Italian GPs monitor plasma lipid levels in patients with TIA or stroke and how they control elevated plasma lipid and lipoprotein levels in patients at high risk of disease recurrence.
Overall total cholesterol levels are known in approximately 55% of the patients with stroke and 65% of those with TIA. This finding may be explained in several ways. Firstly, some GPs may not have recorded relevant data; secondly, the invalid patient may not easily access the physician office; thirdly, the knowledge of plasma lipid levels is not perceived as relevant to the management of the patient. We believe that this latter possibility largely contributes to our findings.
Overall, as for plasma lipid management, TC was controlled in 70.3% of patients, according to the current Italian guidelines; this document doesn't recognize stroke as an equivalent of CHD and requires total cholesterol level > 190 mg/dl and previous myocardial infarction/global coronary risk > 20% in 10 years to recommend statin therapy.
In addition, if we apply the more stringent targets suggested by the third Report of the National Cholesterol Education Program, a smaller percentage of stroke or TIA patients monitored in this study should be considered as controlled for lipid parameters: 20.6% for TC levels, 5.0% for LDLc levels, and 30.9% for HDLc levels. These data clearly underscore the need of a more aggressive approach to lipid lowering in patients with stroke/TIA by Italian GPs.
At present, relatively few patients are taking statins, despite the evidence that lipid lowering, particularly with statins, reduces the risk of stroke [22] and that these drugs are effective even in patients with only mild-to-borderline cholesterol elevations [7]. It is well documented that the compliance with the guidelines by physicians is far from being optimal [23–25]. Furthermore, less than half of the patients who qualify for any kind of lipid-lowering treatment for CHD risk reduction are receiving it [26]. Accordingly, the data from our study show that only about 46% of patients at high risk, qualifying for statin treatment, were actually prescribed such therapy, further stressing the need of improving compliance to guidelines by GPs.
However, it must be noted that the benefit of lipid lowering for prevention of stroke has been only recently demonstrated and that the Italian guidelines available when our database was queried did not specifically recommended the use of statins for this purpose.
Prescription of statins in this study was not associated with a higher number of patients controlled for lipid parameters; there are several possible explanations for such a result. First, patients selected for statin treatment were likely to be at higher risk (worse lipid profile) with respect to untreated patients (Table 4). Second, the relatively small effect on lipid control on statin use may be due to poor compliance of the patient. Data concerning doses of statins used and/or duration of treatment are not available. Third, the concept of treatment to target is not being perceived as a goal by physicians, perhaps because reaching the recommended levels requires intensive efforts. Accordingly, 646 patients with lipid values requiring treatment were not treated (Table 3).
Our study also has some limitations: the GPs enrolled in the study were selected for having a more detailed database and this may have led to over-estimation of the real entity of lipid control. Moreover, no attempt was made to validate the diagnosis of stroke or TIA and no information about compliance has been recorded. This, however, is not directly relevant to our study since we aimed at addressing physician attitude towards control of plasma lipid in patients diagnosed with stroke or TIA.
Passive methods of disseminating and implementing guidelines by publication in professional journals or mailing to targeted healthcare professionals, rarely lead to changes in prescribing behaviour in routine practice. Since there are specific barriers to change, multifaceted interventions may be more effective than single interventions [27]. In our opinion, efforts to improve blood lipid level control in secondary prevention of ischaemic stroke should include audit and feedback [28] and the use of automated electronic reminders [29].
In summary, this study demonstrates the need to improve both the monitoring and intervention strategies on plasma lipid levels in patients with a diagnosis of stroke or TIA. Even in the presence of concomitant diseases such as diabetes and MI, which may per se require the use of hypolipidaemic drugs, a high number of patients are not adequately controlled for blood lipids.
Overall, the planning of novel educational strategies for both patients and physicians, which will underline the relevance to identify high-risk patients in order to improve prevention, is clearly requested.