
Abstract
Background
The development of new strategies to encourage increased levels of physical activity can help to reduce the incidence of cardiovascular disease. A new system of electrical muscle stimulation (EMS) has been developed that attempts to cause an increase in energy expenditure by mimicking the action of shivering in the body. The purpose of this study was to show that this form of EMS is capable of eliciting a cardiovascular exercise response in healthy adults.
Design
An observational study.
Methods
Ten healthy volunteers completed a maximal treadmill test and four EMS sessions using a hand-held EMS device that delivered current to the body via five silicone rubber electrodes on each leg. At each session subjects completed 3 min stimulation at each of four stimulation outputs (10, 20, 30 and 40% of maximum output) while cardiopulmonary gas exchange and heart rate (HR) were measured. Physiological responses at increasing levels of stimulation were evaluated.
Results
Average (±SD) HR and oxygen consumption (VO2) levels of 67 ± 11 bpm and 4.7 ± 1.2 ml/kg per min at rest, respectively, were increased to 186 ± 10 bpm and 44.9 ± 9.8 ml/kg per min at peak exercise intensity on treadmill testing. The electrical stimulation was generally well tolerated by the subjects. Subjects demonstrated statistically significant increases in all physiological variables measured with successive increases in stimulation intensity. Peak HR and VO2 at 40% stimulation intensity were 101 ±12 bpm and 14.9 ± 4.3 ml/kg per min, respectively.
Conclusions
These results demonstrate that this form of EMS is capable of producing a physiological response consistent with cardiovascular exercise at mild to moderate intensities. It achieves this without producing gross movement of the limbs or loading of the joints. This EMS-induced cardiovascular exercise response could be used to promote increased levels of physical activity in populations unable to participate in voluntary exercise.
Introduction
Reduced physical fitness and a sedentary lifestyle are major risk factors for the development of cardiovascular disease. Protection against cardiovascular disease can be achieved by engaging in physical activity/cardiovascular exercise [1]. This involves body movement produced by repetitive muscle contraction that substantially increases energy expenditure [2]. Unfortunately, those who most need to exercise are often unable to do so because of their underlying disease. This includes individuals with spinal cord injury [3], and to a lesser extent, obesity [4].
A solution to this problem is to use electrical muscle stimulation (EMS) to elicit a cardiovascular exercise response through the facilitation of repetitive contractions of large muscle groups. However, conventional EMS-induced tetanic muscle contractions have a minimal effect on energy consumption. Eijsbouts and co-workers [5] demonstrated that bilateral stimulation of the quadriceps, hamstrings, gastrocnemius and tibialis anterior muscle groups at maximally tolerated intensity could produce an increase in oxygen consumption (VO2)of approximately 0.11/min in healthy adults at rest and during arm-cranking exercise. Such levels of VO2,in isolation, are unlikely to result in therapeutic benefit. Other efforts have been targeted at investigating the effects of EMS-induced leg cycling exercise (EMS-LCE) in healthy and spinal cord-injured (SCI) individuals. In EMS-LCE, EMS-induced muscle contractions produce movement that dissipates energy through an external apparatus, a cycle ergometer. EMS-LCE can result in VO2 levels of the order of 0.6-0.8 l/min in SCI individuals [6,7]. Training with EMS-LCE can also result in improvements of 10-35% in aerobic capacity (peak VO2) in SCI individuals [8–11].
Muscles may be viewed as energy conversion elements, which convert stored energy to mechanical work [12]. The aerobic energy conversion process requires oxygen to be delivered to the muscle fibres. As with any thermodynamic conversion process, some of the energy is dissipated in the form of heat, and is not converted to mechanical energy. The mechanical energy produced by the muscles is transmitted to the external environment through the skeletal system, and is dissipated in the form of work as locomotion or mechanical energy in an external device [13]. Consequently, stimulating a cardiovascular response by increasing oxygen demand is normally associated with the dissipation of energy into the external environment in the form of work. For those individuals whose movement is restricted or who are unable to bear weight on their joints, it is desirable to reduce the efficiency of the energy conversion process, such that the maximum energy is consumed for the minimum mechanical work created.
We have developed a novel EMS system capable of eliciting a cardiovascular exercise response with minimal gross movement or loading of the limbs or joints. The pattern of EMS used in this investigation was modelled on shivering, which is the natural process for generating heat when the body temperature falls. Shivering generates heat with no external work [13] through rhythmical muscle contractions, occurring at a rate of approximately 4-8 Hz. We attempted to mimic this pattern of muscle activity by using EMS to elicit cardiovascular exercise via rapid, short-duration, rhythmical contractions in the large lower extremity muscle groups. The purpose of this study was to show that this form of EMS is capable of eliciting a cardiovascular exercise response in healthy adults by causing a substantial increase in energy expenditure.
Methods
Ten healthy volunteers were recruited from the staff working at Castle Hill Hospital, Hull, UK. The Hospital Ethics Committee approved the study, and written informed consent was obtained in all cases. The 10 subjects included eight men and two women with a mean age of 37.6 ± 6.8 years (range 31-49) and an average weight and body mass index (BMI) of 76.3 ± 14.1 kg and 24.7 ± 3.5 kg/m2, respectively. Before participating in the study, each individual had a complete physical examination to ensure that they were fit to undertake physical activity. Physical examination was completely normal in all individuals.
A specially designed hand-held muscle stimulator (BioMedical Research Ltd., Galway, Ireland) powered by a 9 V battery was used in this investigation. The stimulator current waveform was designed to produce rhythmical contractions in the lower extremity muscle groups occurring at a frequency of 4 Hz. The maximum peak output pulse current used in the present study was 120 mA, which was 40% of the maximum rated output. Impulses were delivered through five silicon rubber electrodes on each leg (area per leg 600 cm2)as illustrated in Figure 1. These were applied to the body via a pair of tight-fitting shorts, which extended to the knee. The quadriceps, hamstrings and gluteal muscles were stimulated as the subjects lay supine for all stimulation sessions.
Each subject underwent a maximal cardiopulmonary exercise treadmill test with metabolic gas exchange using the modified Bruce protocol before his or her first stimulation session. Stimulation sessions consisted of 3 min rest in supine lying, followed by 12 min EMS, during which the stimulation intensity was increased every 3 min by increments of 10% up to a limit of 40% of maximum stimulator output. Each subject completed four stimulation sessions and was free to end a session prematurely if they felt uncomfortable for any reason. Eight of the 10 subjects completed all four stimulations sessions, whereas two subjects completed all sessions at 10, 20 and 30% stimulation intensity but did not complete all sessions at 40% intensity; however, these two subjects did reach 40% stimulation intensity during at least one session. Cardiopulmonary gas exchange was simultaneously assessed using a facemask and gas analysis system (Oxycon Delta; Erich Jaeger GmBH, Germany) to assess VO2, carbon dioxide consumption (VCO2), and minute ventilation (VE). Continuous heart rate (HR) and electrocardiographic monitoring was carried out during every EMS session.
Data analysis
The data were analysed in two ways: The magnitude of the physiological response to EMS-induced exercise was assessed using the average of the peak HR (bpm) and VO2 (ml/kg per min) at 40% stimulation intensity during repeated sessions. Subjects' peak HR, peak VO2, heart rate reserve (HRR; maximum resting HR), and oxygen consumption reserve (VO2R; maximum resting VO2) were calculated from their treadmill test data. The level of increases in HR and VO2 at 40% stimulation intensity relative to resting levels were then calculated and expressed as a percentage of HRR and VO2R, respectively, for each subject to calculate the exercise training intensity they achieved using EMS. Peak energy expenditure (kcal/h) at 40% stimulation intensity was also calculated for each subject to identify calorie consumption.
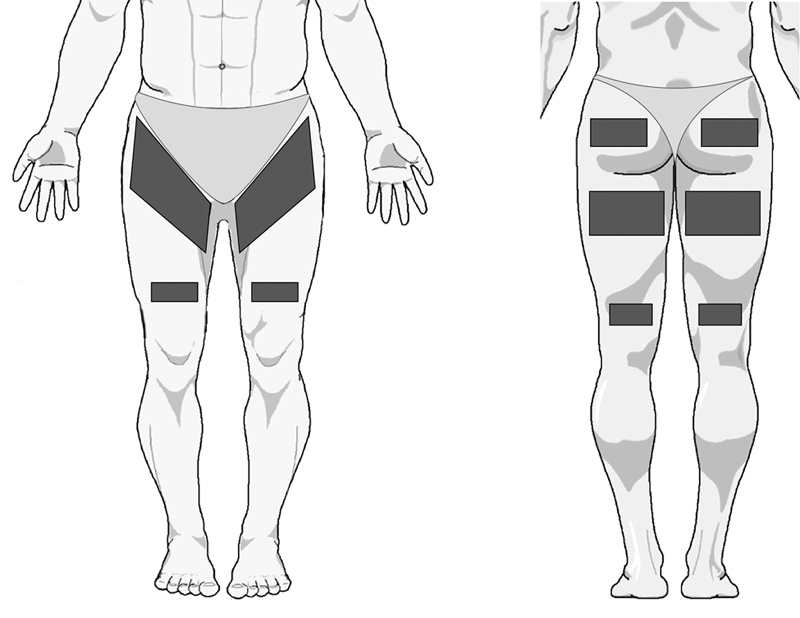
Location of stimulating electrodes.
The dose-response relationship associated with this form of EMS was analysed by measuring physiological responses at increasing intensities. Peak VO2, VCO2,VE and HR values were recorded at rest and at each stimulation intensity level at each EMS session. Increases in each variable at 10, 20, 30 and 40% of maximum stimulation output compared with resting values were then calculated for each subject, and group mean (± SD) increases were calculated. Increases above resting values were expressed in absolute and relative terms. Differences in physiological responses between the different levels of stimulation were assessed using repeated measures analysis of variance with post hoc comparisons between levels using paired t-tests. The level of significance was set at the 99% confidence level with a Bonferroni-adjusted P value of less than 0.0008.
Results
Subjects' resting HR and VO2 plus peak HR and VO2 from their treadmill test and at 40% stimulation are shown in Table 1. The physiological response to EMS-induced exercise varied between subjects. Group average peak HR and VO2 were 101 ± 12 bpm and 14.9 ± 4.3 ml/kg per min, respectively, at 40% stimulation intensity. Training intensities experienced by the subjects were similar whether the HRR or VO2R method was used as the basis for calculation (r = 0.6), and also varied between subjects. Training intensities ranged from 20 to 47% when the HRR method was used and from 16 to 50% when the VO2R method was used to calculate the training intensity. Group mean peak energy expenditure at 40% stimulation was 351 ± 82 kcal/h.
Increases in VO2, VCO2, VE and HR with successive increases in stimulation intensity are illustrated in Figure 2. Subjects exhibited increases in all physiological variables during stimulation compared with resting values. VO2, VCO2, VE and HR were all significantly increased at 10% stimulation intensity when compared with resting values (P < 0.01). Group mean values for these variables continued to increase significantly with each increase in stimulation level up to 40% of stimulation output (P < 0.01). At 40% stimulation intensity VO2 and VCO2 increased by 0.7 ± 0.2 and 0.6 ± 0.2 l/min, respectively, compared with resting levels. VE increased by 13.8 ± 10.8 l/min and HR increased by 30.1 ± 11.1 bpm above resting values.
Physiological responses to 40% stimulation intensity
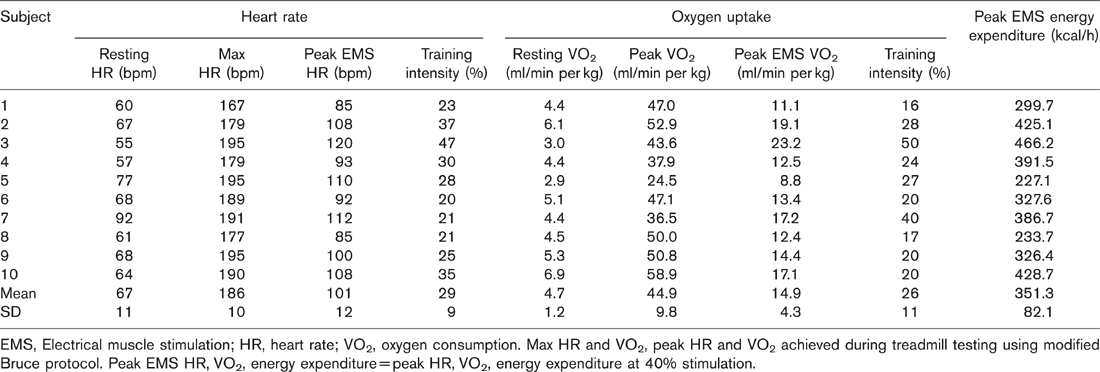
EMS, Electrical muscle stimulation; HR, heart rate; VO2, oxygen consumption. Max HR and VO2, peak HR and VO2 achieved during treadmill testing using modified Bruce protocol. Peak EMS HR, VO2, energy expenditure = peak HR, VO2, energy expenditure at 40% stimulation.
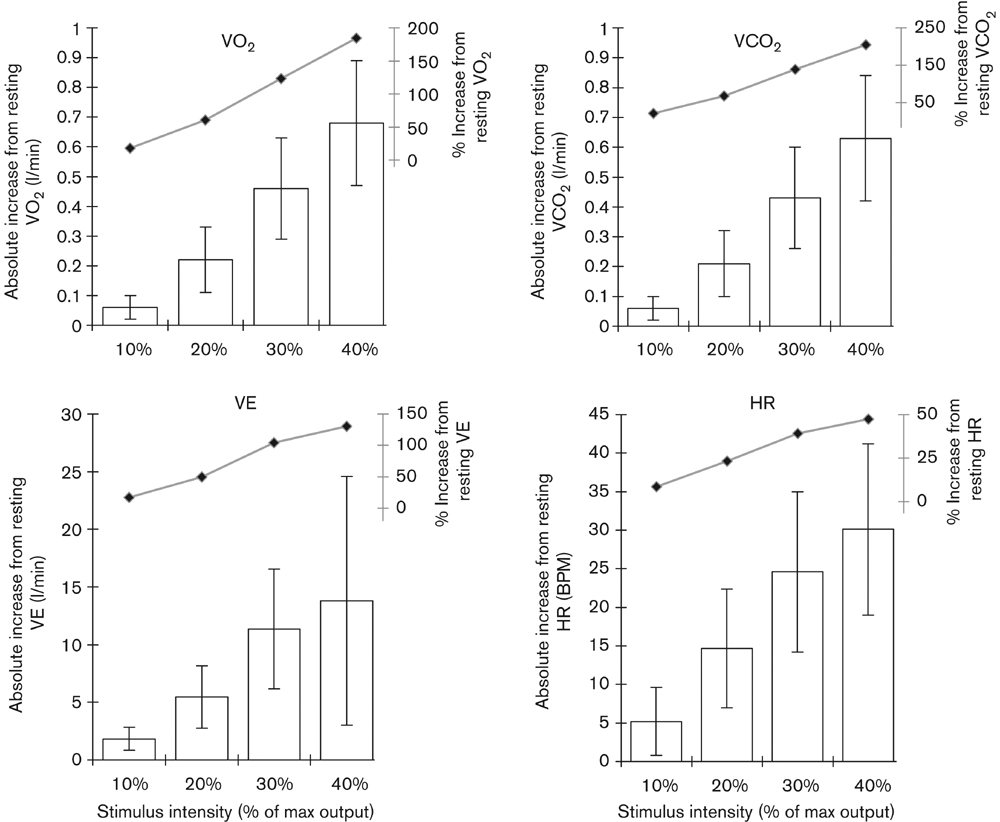
Increases in physiological responses with successive increases in stimulation intensity. Values are group mean responses from all sessions completed at each stimulation level (±SD). Differences between group mean responses at different stimulation intensities are statistically significant for all variables (P < 0.01). HR, Heart rate; VE, minute ventilation; VCO2, consumption of carbon dioxide; VO2, consumption of oxygen.
Discussion
The results from this investigation demonstrate that this novel application of EMS can elicit a cardiovascular exercise response. That is, it can produce a substantial increase in energy expenditure via repetitive muscle contractions. Physiological responses to this EMS-induced exercise were consistent, with a light to moderate exercise intensity; peak EMS-induced exercise intensities ranged from 2.5 to 7.7 metabolic equivalents, and the group mean training intensity was approximately 26-29%. Mean levels of energy expenditure (351 ± 82 kcal/h) were similar to levels expected for activities such as walking at 3-3.5 mph; calculated on the basis of a mean body weight of 76 kg [13]. At this level of energy expenditure, subjects would have to use the device for an approximate cumulative total of 2 h per week to have performed the minimum quantity of exercise recommended for health benefit by the American Heart Association (700 + kcal/week) [14]. However, it is unlikely that repeated exposure to this exercise intensity would be sufficient to result in increases in cardiovascular fitness (peak aerobic capacity), as a training intensity of 40% of HRR or VO2R is regarded as the threshold level for increases in VO2max [15].
It is important to note that the subjects in the present investigation only used the stimulator at 40% of its maximum capacity. This limit was introduced as this was the first study of the effects of this system of EMS in healthy adults, and it was necessary to investigate safety and tolerability at submaximal stimulation intensities at this stage of the investigation. Physiological variables observed in the study indicated that none of the subjects experienced an adverse cardiovascular reaction to the EMS-induced exercise. Physiological responses were consistent with those to be expected during voluntary exercise, suggesting that this form of EMS can elicit an exercise response in a safe manner. The stimulation was generally well tolerated by the subjects, with only two subjects reporting it sufficiently uncomfortable to prevent them from reaching a stimulation output of 40% at all sessions. A further two subjects reported that they found the stimulation produced minimal discomfort, whereas the remaining six felt moderate discomfort at 40% output. For most subjects, discomfort levels declined at successive stimulation sessions. This experience is in accordance with our previous experience of EMS, in that subjects usually report greatly varying feelings on its comfort/discomfort, but relative comfort levels improve with use.
We observed statistically significant increases in all physiological variables measured with successive increases in stimulator output. This demonstrates the presence of a clear dose-response relationship with this form of EMS-induced exercise. This indicates that the use of the stimulator at higher intensities is likely to result in a greater cardiovascular response. We have observed higher training intensities at higher stimulation outputs in the course of pilot testing of this form of EMS.
These are important findings, as we have demonstrated that EMS-induced muscle contractions can produce substantial increases in energy expenditure with minimal gross movement of the limbs or loading of the joints. VO2 increased by 0.7 ± 0.2 l/min above resting VO2. Eijsbouts et al. [5] had previously demonstrated VO2 increases of the order of 0.1 l/min in healthy adults using EMS at maximally tolerated intensities. VO2 increases observed in this study are similar in magnitude to those observed previously during LCE produced by EMS in SCI individuals [6,7].
The results observed in this first investigation into this form of EMS are encouraging. This is the first study to show that unloaded EMS-induced muscle contractions can produce a significant increase in cardiovascular exercise intensity and energy expenditure with a clear dose-response relationship. By improving comfort levels associated with this form of stimulation, it should be possible to elicit cardiovascular responses of greater magnitude and promote increases in physical fitness.
In the future, this form of stimulation may prove beneficial for those populations who experience difficulty with the voluntary performance of loaded physical activity, for example, obese patients and patients with spinal cord injury; patient groups who possess an increased risk of developing cardiovascular disease. It could be argued that there are potential difficulties to overcome if this form of stimulation is to prove beneficial in these patient groups. SCI patients may possess a reduced muscle mass, and therefore may not demonstrate sufficient hemodynamic response to this form of stimulation. On the other hand, these patients are also likely to be able to tolerate very high stimulation intensities, and previous investigators have demonstrated that electrical stimulation can be used to promote LCE in SCI patients to good effect [11]. Excessive cutaneous fat in obese patients will result in increased resistance to the transfer of electrical current to neural tissue, and may cause increases in the level of discomfort associated with muscle stimulation. However, electrical stimulation of muscle is routinely used by physiotherapists for patients with varying levels of body fat percentages with good effect. Obese patients may also benefit from prolonged stimulation at lower intensities using larger electrodes (resulting in lower current densities), in order to produce the cumulative energy expenditure required for weight loss. In future studies, we plan to investigate the effects of a period of training using this form of EMS in healthy adults and in patient groups such as those mentioned above.