
Abstract
Background
The risk of cardiovascular disease increases progressively with increasing blood glucose from levels well below the diabetic threshold. In the Reykjavik Study the relationship between heart failure and abnormal glucose regulation was already apparent at the level of impaired glucose tolerance. The aim of this study was to determine the prognosis of participants with any glucose abnormality and heart failure and to test whether the combination of these conditions may adversely affect the subsequent prognosis.
Design
A prospective population-based study.
Methods
Data from the first visit of 19 381 participants were used. Participants were divided into groups according to their glycaemic and heart failure level, and comparisons were made between the groups and disease-free participants serving as a reference group. The risk of mortality and morbidity was calculated with adjustments for main cardiovascular risk factors and ischaemic heart disease.
Results
Participants in the reference group were younger, had lower body mass indices and more seldom a history of myocardial infarction compared with diseased groups. Mortality was lowest in the reference group (P < 0.0001) increasing to a maximum in participants with the combination of glucose abnormality and heart failure. Prognostically, the mortality risk associated with abnormal glucose regulation was increased but was lower than the risk of diabetes. The risk of a new myocardial infarction was highest in participants with diabetes [hazard ratio (HR) 1.6; 95% confidence interval (CI) 1.3-2.0] or diabetes in combination with heart failure (HR 1.8; CI 1.1-2.7).
Conclusions
Heart failure or glucose abnormalities are related to increased morbidity and mortality. The combination of glucose abnormality and heart failure did, however, not add further to the unfavourable prognosis in the presence of ischaemic heart disease.
Introduction
The risk of cardiovascular disease increases progressively with increasing blood glucose from levels well below the present diabetic threshold [1,2]. An already elevated fasting blood glucose increases the incidence of heart failure [3]. The continuous association between blood glucose abnormalities and heart failure is strong, as recently shown in the Reykjavik Study [4]. In this population-based epidemiological study the relationship between heart failure and abnormal glucose regulation was already apparent at the level of impaired glucose tolerance. That underlines the importance of the question of whether the combination of heart failure and abnormal glucose regulation at a prediabetic level affects the prognosis to a greater extent than could be expected from having only one of these disease manifestations, and if it is comparable with the dismal prognosis seen in individuals with diabetes and heart failure [5,6].
The present follow-up of the Reykjavik Study reports on cardiovascular morbidity and mortality over time among participants in relation to the presence of heart failure or glucose abnormalities when originally entering the study. We hypothesized that the combination of these conditions may adversely affect the subsequent prognosis.
Methods
The Reykjavik study plan
All people born between 1907 and 1935, who were inhabitants in Reykjavik on 1 December 1966, were invited to participate in the study as detailed elsewhere [7]. The final year of follow-up was 2001. The attendance rate varied between 65 and 77%, declining somewhat over time.
Baseline characteristics were based on a standardized questionnaire regarding health, social conditions and education in combination with a medical examination. Information was collected on age (years), family history, smoking (yes/no/previous), previous diseases, current medications, height (in cm), weight (in kg), blood pressure (hypertension: systolic pressure ≥ 160 mmHg or diastolic pressure ≥ 95 mmHg or a history of hypertension), body mass index (BMI; kg/m2) and laboratory examinations including cholesterol (mg/dl) [4]. Previous and current ischaemic heart disease (IHD) was defined as a history of myocardial infarction [8], angina pectoris [Rose questionnaire [9] and electrocardiogram (ECG) changes], percutaneous coronary interventions and coronary artery bypass graft surgery noted at the first visit and checked against hospital records. ECG and chest X-ray were performed in each participant as well as an oral glucose tolerance test (OGTT; 50 g glucose in 250 ml water) at each visit until 1990 [4,10,11].
For the purpose of this study each participant was allocated into one of the following six groups on the basis of the information available at their very first study visit. Group 1: the reference group comprising those who were free of glucometabolic abnormalities and heart failure; group 2: participants with abnormal glucose regulation; group 3: participants with type 2 diabetes; group 4: participants with heart failure; group 5: participants with abnormal glucose regulation and heart failure; and group 6: participants with the combination of type 2 diabetes and heart failure.
Informed consent was obtained from all participants and the National Bioethics Committee approved the study as did the Data Protection Authority.
Definitions
Glucometabolic abnormalities were categorized as type 2 diabetes: fasting serum glucose of 7.0 mmol/l or greater (≥ 126 mg/dl) or OGTT serum glucose of 11.1 mmol/l or greater (≥ 200 mg/dl) or abnormal glucose regulation (AGR: newly diagnosed impaired glucose tolerance or elevated fasting glucose) equals fasting serum glucose 6.1-6.9 mmol/l (110-126 mg/dl) or OGTT serum glucose 7.8-11.0 mmol/l (140-200 mg/dl). These conditions were defined on the basis of information from the Icelandic Heart Association questionnaire or as newly diagnosed type 2 diabetes or AGR based on OGTT or, from 1990, fasting serum glucose [4].
Heart failure was defined according to the European Society of Cardiology guidelines as the combination of at least two symptoms, dyspnoea, tiredness or ankle oedema, and one objective evidence of cardiac engagement as disclosed by the ECG (Q-wave myocardial infarction according to MONICA criteria [8], left bundle branch block, left ventricular hypertrophy) or chest X-ray (pulmonary congestion, cardiomegaly or left ventricular enlargement) [12].
Myocardial infarction was defined according to the MONICA criteria [8].
Morbidity and mortality
Cardiovascular and all-cause mortality and morbidity in the form of new myocardial infarctions were registered from the date of the first study visit until 31 December 2001. Mortality was based on information from a complete registry of death causes available from the Icelandic National Roster. All-cause mortality was defined according to International Classification of Disease versions 9-10 [13,14]. Cardiovascular mortality included deaths from coronary artery disease, heart failure, sudden death and stroke.
Statistical analysis
Survival was estimated by means of a Cox regression model using time on study as the timescale, with adjustment for age, smoking, cholesterol, systolic blood pressure, BMI and IHD in a multivariable analysis model. The survival was also estimated and compared using age as the time-scale with similar results [15,16]. Hazard ratios (HR) were used to represent the effect on morbidity and mortality by the different risk groups. Significance levels are given as absolute P values if not less than 0.001.
Results
The Reykjavík Study was attended by 19 381 individuals, of whom 9323 were men. The average time of follow-up was 21.5 years (range 14-30). The heart failure diagnosis was based on symptoms and ECG criteria in 64% of the male and 54% of the female participants, respectively. Eleven per cent of the men and 23% of the women had symptoms combined with chest X-ray criteria. The remaining participants (25% men and 23% women) had symptoms together with ECG and chest X-ray criteria for the diagnosis of heart failure. Sixty per cent of the men and 56% of the women had newly diagnosed diabetes, whereas the rest presented with a history of diabetes. During the study period, 83 men and 67 women with abnormal glucose regulation developed diabetes. Participants with abnormal glucose regulation at a younger age (< 60 years) were more likely to develop diabetes than those who presented with abnormal glucose regulation at an older age.
The distribution of participants in groups 1-6 and their clinical characteristics are presented in Table 1. This table also reveals the proportion of patients with ischaemic heart disease and those with a history of myocardial infarction. Participants in the reference group were younger and had a lower BMI, but they less often had a history of hypertension and ischaemic heart disease. Smoking habits and blood cholesterol did not differ much between the groups.
Mortality
The number of participants who died during the complete period of follow-up is presented in Table 2. The total mortality was highest in those with the combination of any glucose abnormality and heart failure (P < 0.0001) and cardiovascular death was the single most common cause in all groups, on average 48% among men and 34% among women, and lowest in the reference group among both sexes.
Survival curves during the first 10 years of follow-up are presented in Figure 1. In the age-adjusted Kaplan-Meier survival estimates the mortality was significantly higher among participants with glucometabolic perturbations or heart failure compared with those in the reference group. In addition, there was a trend towards impaired survival in those with a combination of glucose abnormality and heart failure compared with the heart failure group (P < 0.01). All case groups still had a high mortality risk after adjustment for age, ischaemic heart disease and other risk factors. However, after testing for interaction the trend towards impaired survival in the group with the combination of glucose abnormality and heart failure did not remain significant (Table 3). As presented in Table 3, the HR for survival decreased in all case groups after adjustments in which age and ischaemic heart disease had the greatest contribution.
The adjusted HR and 95% confidence intervals related to survival in the reference population (group 1) for all-cause and cardiovascular mortality during the total time of follow-up with age as the time scale for both sexes combined are presented in Figure 2. Both heart failure and diabetes were related to a significant increase in mortality during follow-up, and mortality was also increased among those with abnormal glucose regulation. By and large, the pattern was similar for cardiovascular mortality. The combination of a glucose abnormality and heart failure did not increase the mortality significantly compared with the existence of only one of these disorders.
Morbidity
The HR and 95% confidence intervals for developing a new myocardial infarction in participants in groups 2-6 in relation to those in reference group 1 are presented in Table 4. The risk was increased in men and women with diabetes and in women with heart failure. Overall, there was a trend towards a higher risk among women, particularly those with the combination of diabetes and heart failure. Abnormal glucose regulation did not show an association with the development of myocardial infarction.
Clinical characteristics at the first visit in the Reykjavik study population divided into the six study groups, adjusted for age
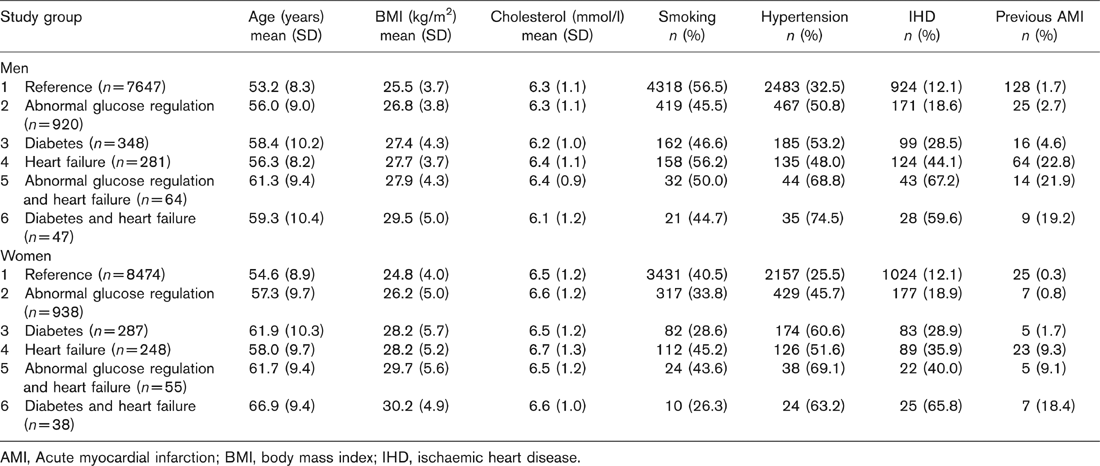
AMI, Acute myocardial infarction; BMI, body mass index; IHD, ischaemic heart disease.
All-cause and cardiovascular mortality In the six groups by the end of follow up

AGR, Abnormal glucose regulation.
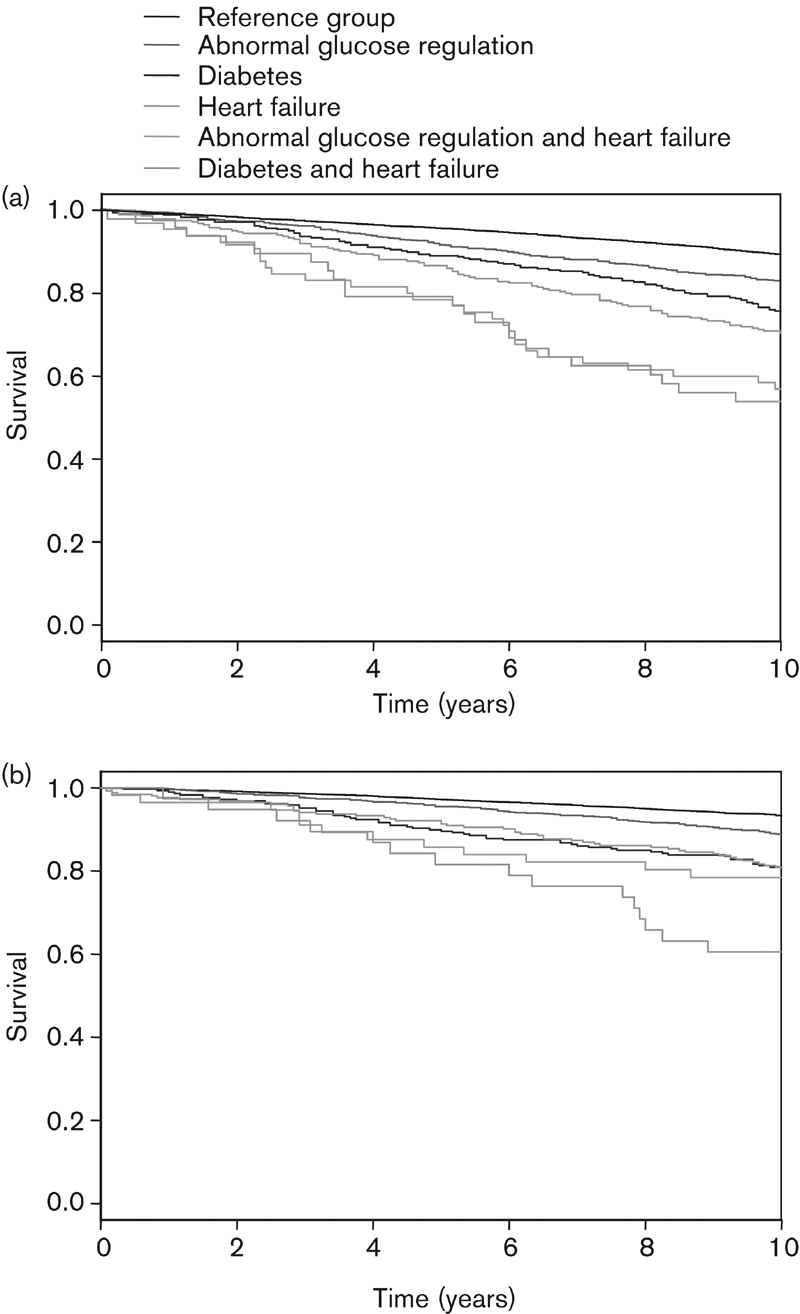
Survival curves during 10 years of follow-up for all groups of participants with/without heart failure and a glucose abnormality adjusted for age; (a) men (b) women.
Discussion
In this truly population-based study diabetes and heart failure were linked to an unfavourable vital prognosis, already apparent among individuals with less pronounced glucometabolic perturbations, including those newly detected by means of a glucose tolerance test. The outcome, which was unrelated to sex, remained after adjustments not only for traditional risk factors for coronary artery disease but also for previously known ischaemic heart disease. The trend towards an added unfavourable prognosis of the combination of glucometa-bolic perturbation and heart failure did, however, not reach statistical significance compared with the prognostic information by each of these conditions on their own.
The present findings are unique because they originate from a very large study population with a high participation rate and an unusually long period of follow-up. Combined with a complete registration of cardiovascular morbidity and mortality based on official registries and hospital records this should make the study well suited to explore the importance of glucose abnormalities, including those newly detected. A potential limitation is the lack of an originally defined heart failure algorithm in the study protocol because heart failure is a diagnosis based on clinical criteria and thereby is less well suited for epidemiological studies. According to guidelines from the European Society of Cardiology, the heart failure diagnosis should be based on both symptoms and signs of heart failure [12]. Currently, the best method to diagnose myocardial dysfunction is echocardiography. The present study was designed in 1966, and by then neither echocardiography nor clear recommendations of heart failure symptoms, major or minor, were available. The Reykjavik Study questionnaire did, however, include many questions on tiredness, breathlessness and oedema, which together with ECG registrations and chest X-ray made it possible to define heart failure with reasonable accuracy.
Patients with diabetes are at a high risk of cardiovascular disease. The highest proportion is seen in individuals with additional cardiovascular risk factors [17]. Hypertension together with myocardial infarction was the main risk factor for heart failure in the Framingham study [18]. Likewise, the Rotterdam Study showed an increased risk of heart failure in participants with ischaemic heart disease [19]. The present finding, that previous myocardial infarction was more prevalent in participants with heart failure, is thus not surprising. Participants with diabetes had an increased risk of developing a new myocardial infarction, further illustrating the relationship between glucometabolic perturbations and ischaemic heart disease. These disorders are, together with hypertension, often referred to as the cardiotoxic triad. The existence of such an entity gets support from the above-mentioned results. However, abnormal glucose regulation did not confer any risk of myocardial infarction by itself.
Survival analysis based on follow-up until 1 January 2002 in all groups of participants
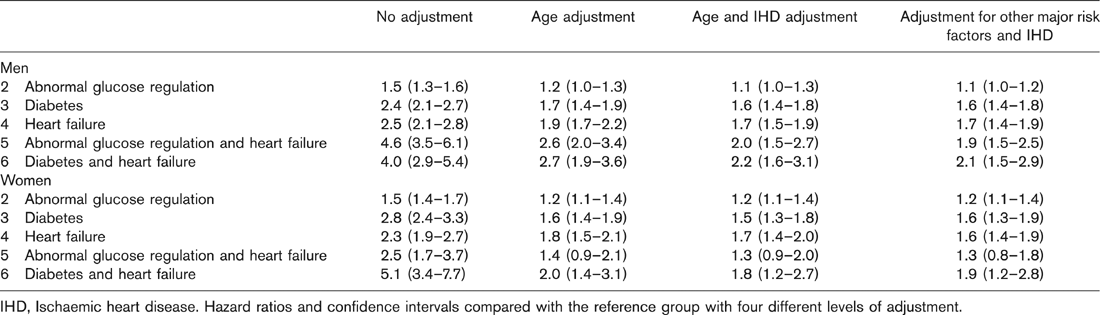
IHD, Ischaemic heart disease. Hazard ratios and confidence intervals compared with the reference group with four different levels of adjustment.
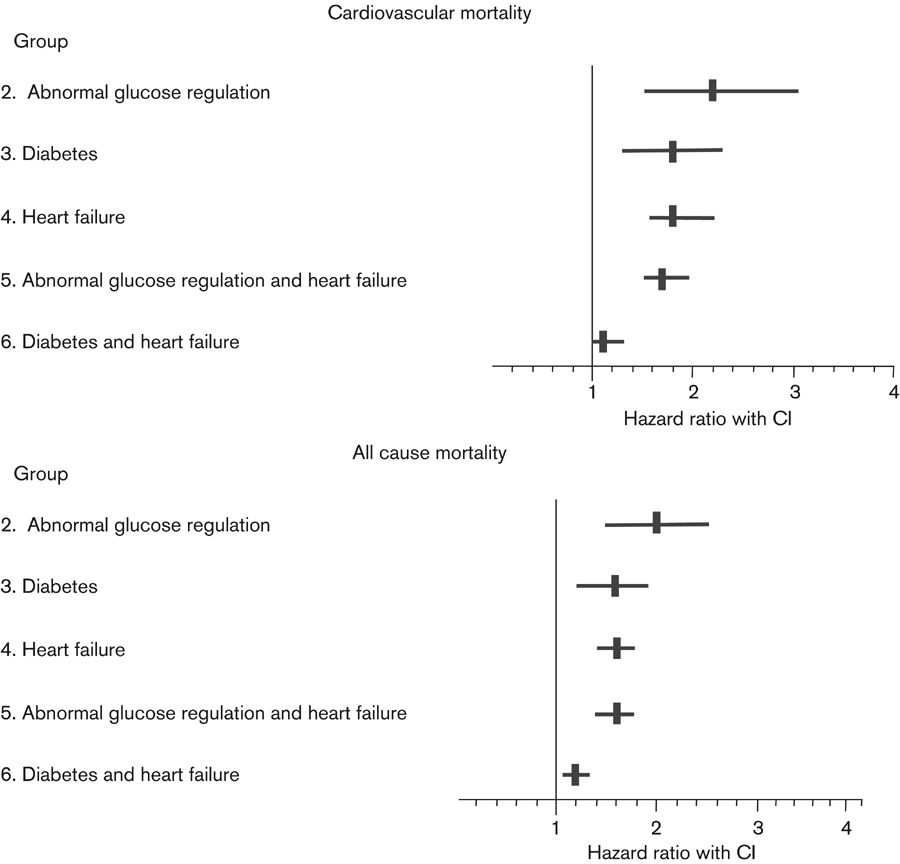
All-cause and cardiovascular mortality during total follow-up time data for all participants (men and women). Adjustments are made for age, systolic blood pressure, cholesterol, body mass index, smoking and ischaemic heart disease. Data are presented as hazard ratios (95% confidence intervals; CI).
New myocardial infarctions in participants, without or with a previous myocardial infarction, in the study groups in relation to the reference population (group 1)
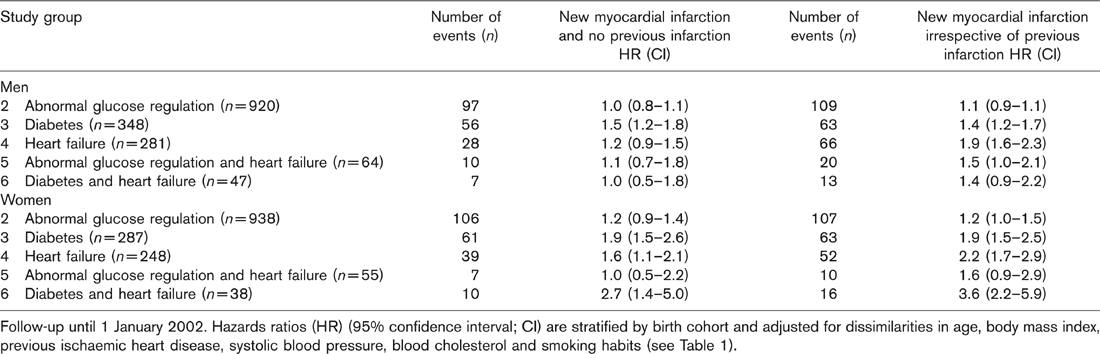
Follow-up until 1 January 2002. Hazards ratios (HR) (95% confidence interval; CI) are stratified by birth cohort and adjusted for dissimilarities in age, body mass index, previous ischaemic heart disease, systolic blood pressure, blood cholesterol and smoking habits (see Table 1).
Since first suggested by Lundbaek [20] in 1954, the presence of special diabetes cardiomyopathy has been debated as has its pathophysiological background. In 1974, Kannel et al. [21], on the basis of epidemiological data from the Framingham Study, proposed that diabetes causes some form of cardiomyopathy. The unfavourable vital prognosis in diabetic patients with left ventricular dysfunction has often been related to the presence of a widespread and diffuse coronary artery disease causing ischaemic cardiomyopathy [22]. The fact that mortality differences in the present study remained after adjustments makes ischaemic heart disease a less likely single explanation for the increased mortality. It rather indicates that there may be a direct relationship between glucose abnormalities and myocardial performance.
Morphological changes seen in the diabetic heart are not specific for this disease. Similar structural abnormalities are seen in the hypertensive heart [23,24]. However, some changes, such as increased left ventricular mass and wall thickness, seem to increase with worsening glucose intolerance [23,25]. The present study did, however, not reveal a poorer prognosis of participants with the combination of a glucose abnormality and heart failure when compared with participants with either disease occurring separately. Our results do not therefore add complete evidence for the existence of a specific diabetic cardiomyopathy. Too few participants in the groups combining glucose abnormalities and heart failure is the most likely explanation for the lack of a statistically significant impaired prognosis compared with that with either disease. In a study of elderly patients with diabetes, Bertoni et al. [26] found a significantly higher mortality in those with heart failure and diabetes compared with those with diabetes only. Gustafson et al. [5] noted that diabetes is an independent risk factor for mortality in patients with heart failure. Such studies did, however, look at patients rather than general populations. To the best of our knowledge, the present investigation is the only truly population-based epidemiological study. Additive information, supporting the existence of a diabetic cardiomyopathy, would be that improved glucometabolic control in individuals with the combination of glucose abnormality and heart failure improve their prognosis irrespective of the existence of ischaemic heart disease. Such a study would be of major interest as an attempt to improve survival in patients with the combination of heart failure and glucose perturbations, a common group.
Poor glycemic control has been associated with an increased risk of heart failure in diabetic patients without previous myocardial infarction, with each 1% increase in haemoglogin Alc associated with a 12% increased risk of heart failure [27]. The present findings indicate that tight glycemic control may be of interest to test, with the goal to improve the prognosis in heart failure not only in patients with established diabetes, but also in those with abnormal glucose regulation.
Conclusion
Heart failure or glucose abnormalities occurring separately and together are related to an increased morbidity and mortality, but the combination of these disorders did not have a significant interaction effect. Abnormal glucose regulation is associated with diminished survival unrelated to the presence of ischaemic heart disease, and to our knowledge shown for the first time in such a large, truly population-based study.
Footnotes
Acknowledgements
The authors would like to give special thanks to Ingibjörg Stefánsdóttir for help in data collection and to staff of the Icelandic Heart Association for other assistance.