
Abstract
Background Chronic heart failure (CHF) is a serious condition that is associated with impaired health status and a high prevalence of depressive symptoms. To date, little is known about the determinants of health status and depressive symptoms in CHF. Therefore, the aim of this study was to assess whether Type D personality is associated with impaired health status and increased depressive symptoms in heart failure patients, independent of disease characteristics.
Methods Eighty-four patients (63 men and 21 women, mean age=65.9±12.1 years) with systolic CHF completed four questionnaires to assess Type D personality (14-item Type D Personality Scale [DS14]), health status (Minnesota Living with Heart Failure Questionnaire [MLWHFQ]), depressive symptoms (Center for Epidemiological Studies Depression Scale [CES-D]) and mood status (Global Mood Scale [GMS]) when visiting an outpatient heart failure clinic. Information on clinical variables was obtained from patients’ medical records.
Results Type D patients were more likely to experience impairment in health status (18/38=47%) as compared to non-Type Ds (11/46=24%), P=0.027. They also more often reported symptoms of depression; namely 18 of 38=47% versus 6 of 46=13%, P=0.001. When controlling for severity and etiology of CHF, age and gender, Type D remained a significant associate of impaired health status [odds ratio (OR) 3.0, 95% confidence interval (CI) 1.12–7.78] and depressive symptoms (OR 6.3, 95% CI 2.08–19.12).
Conclusions Type D was associated with impaired health status and increased depressive symptoms in CHF patients. These preliminary findings demonstrate the value of including personality factors in CHF research.
Introduction
Chronic heart failure (CHF), which is the end-stage of most heart diseases, is an important cause of cardiac morbidity and mortality [1], and has been labeled as an ‘emerging epidemic’ [1, 2]. CHF has also been related to impaired health status and quality of life [3–5] and comorbid depression [3, 6, 7]. Quality of life is a frequently used outcome measure in medical research and some patients have rated it as more important than extended survival [8]. Depression has been associated with increased risk of morbidity, mortality, (re)hospitalization [9, 10], and poor health status [3, 6] in CHF.
However, most studies have focused on the prevalence of depressive symptoms in hospitalized patients with CHF [6]. Gottlieb et al. [6] were among the first to determine the prevalence of depression in outpatients with heart failure and found depression to be a common comorbid condition. Moreover, little is known about the determinants of health status and depression in CHF, although studies have shown that markers of CHF severity cannot explain differences in poor quality of life [4, 6, 11]. Furthermore, to our knowledge the determinants of mood status have not been examined in CHF. Taken together, these findings suggest that we may need to expand our focus beyond looking at traditional risk factors, as knowledge of these determinants may lead to an expansion and refocusing of the treatment strategies used in CHF.
Personality may be an important determinant of individual differences in health status and depression in CHF that largely has been overlooked. Neuroticism, for example, has been shown to be an independent predictor of increased mortality in patients with CHF [12]. The adverse affect of the distressed (Type D) personality on health outcomes in patients with coronary heart disease (CHD), including high-risk patients with decreased left ventricular function following myocardial infarction, is also well documented [13–15]. A high score on two stable personality traits, namely negative affectivity (the stable tendency to experience negative emotions and effect across time and situations) and social inhibition (a stable tendency to inhibit the expression of these negative emotions in social situations) defines Type D personality [13, 16]. Type D personality is associated with increased risk of morbidity, mortality and impaired quality of life in patients with acute coronary syndromes [13, 14, 17]. A recent study also showed that Type D individuals with an implantable cardioverter defibrillator suffered from more anxiety and depressive symptoms compared with patients with non-Type D personality adjusting for experienced shocks [18]. Although patients with CHD are at risk of developing CHF, to our knowledge no study has examined the effect of Type D personality on health and mood status in patients with CHF.
Thus, the objective of the current study was to examine whether Type D personality is associated with impaired health and mood status and increased depressive symptoms in unselected outpatients with CHF.
Methods
Study population
Consecutive unselected patients (n = 121) with a diagnosis of systolic heart failure, visiting the heart failure outpatient clinic of the TweeSteden teaching hospital in Tilburg, the Netherlands, were asked to participate in the current study. Inclusion criteria were: (1) left ventricular ejection fraction <40% (LVEF); (2) systolic heart failure; and (3) capable of reading and understanding the Dutch language. Patients with other life threatening comorbidities (e.g. cancer, lung diseases etc.) were excluded.
Patients were treated for CHF according to the most recent guidelines by a cardiologist and a specialized heart failure nurse. Ninety-one (75%) patients agreed to participate and completed four psychological questionnaires. Seven questionnaires had too many missing values (> 10%) on the Type D Personality Scale and the Global Mood Scale (GMS) to extrapolate, and these patients were excluded from the study.
Clinical variables
Sociodemographic variables included gender and age. Information on severity (New York Heart Association [NYHA] functional class and LVEF) and etiology (ischemia) of heart failure was obtained from the specialized heart failure nurse or the treating cardiologist. Information on clinical variables (hypertension, diabetes mellitus, smoking, hypercholesterolemia, and adiposity) and medication was obtained from the patients’ medical records.
Type D personality
Type D personality was measured with the 14-item Type D Personality Scale (DS14) [19]. The scale comprises two subscales, negative affectivity and social inhibition, containing seven items respectively. Examples of items measuring negative affectivity are ‘I often make a fuss of unimportant things', and ‘I often feel unhappy'. ‘I often feel inhibited in social interactions', and ‘I find it hard to start a conversation’ are examples of items of the social inhibition subscale. The items are answered on a five-point Likert scale from 0 (false) to 4 (true). A predetermined cut-off of ≥ 10 on both subscales is used to determine those with a Type D personality [19]. Both subscales have good test–retest validity and high internal validity with Cronbach's α of 0.88 and 0.86 for the negative affectivity and social inhibition subscales, respectively [19].
Health status
The Minnesota Living with Heart Failure Questionnaire (MLWHFQ), a disease-specific quality of life instrument, was used to assess health status [20]. This questionnaire consists of 21 items that are answered on a four-point Likert scale. The reliability of the scale is good with Cronbach's α of 0.95 [20]. A higher score on the MLWHFQ represents a poorer health status. The MLWHFQ is a frequently used measure to assess health status in CHF patients [6].
Depression and mood status
Depressive symptomatology was assessed with the Center for Epidemiological Studies Depression Scale (CES-D) [21], a measure that frequently has been used to measure depressive symptoms in CHF [22]. The 20 items are answered on a four-point Likert scale ranging from 0 (rarely or none of the time) to 3 (most or all of the time). A higher score on the CES-D indicates more depressive symptoms with a score ≥ 16 indicating likely depressive symptomatology. The CES-D has a high internal consistency as measured by Cronbach's α ranging from 0.85–0.90, and scores correlate highly with other self-report measures of depressive symptoms [23].
The 20-item GMS was used to evaluate mood status, defined as negative and positive affect [24]. Each subscale consists of 10 items that are answered on a five-point Likert scale ranging from 0 (false) to 4 (true). The scale has a high internal consistency with Cronbach's α of 0.90 [24].
Procedure
Patients were approached by letter and asked to fill in the four questionnaires. Patients who had not returned the questionnaires within 2 weeks received a reminder telephone call. This study was conducted at the heart failure outpatient clinic of the TweeSteden Hospital as part of daily clinical practice. Patient participation was voluntary.
Statistical analysis
Discrete variables were compared with the chi-squared test and continuous variables with Student's t-test. Univariate and multivariate logistic regression analyses were used to assess the association between Type D personality and the outcome measures health status, depressive symptoms and mood status. Prior to running logistic regression analyses, the scores on the questionnaires were recoded into discrete variables. The highest tertile on the MLWHFQ indicated impaired health status, whereas the highest tertiles of both subscales of the GMS indicated increased negative effect and increased positive effect, respectively. In multivariate analyses, we adjusted for NYHA functional class, LVEF, etiology of CHF, gender, and age. All statistical tests were two-tailed. P < 0.05 was used for all tests to indicate statistical significance. Odds ratio (OR) with 95% confidence intervals (CI) are reported. All statistical analyses were performed using SPSS 11.5 for Windows (SPSS Inc.), Chicago, Illinois, USA.
Patient characteristics
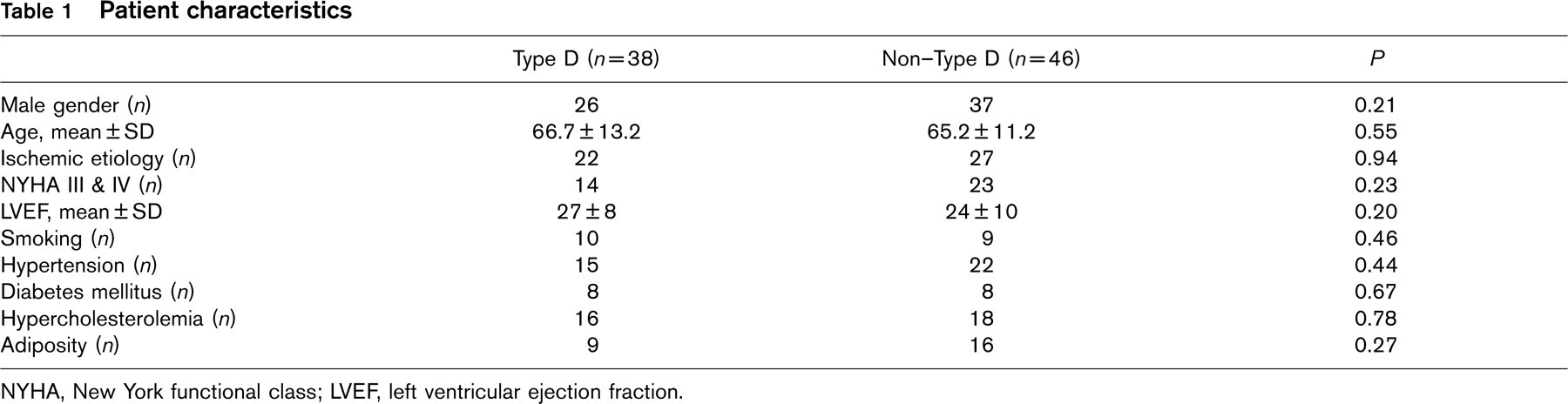
NYHA, New York functional class; LVEF, left ventricular ejection fraction.
Results
Patient characteristics
Patient characteristics are listed in Table 1. No significant differences were found between Type D and non-Type D patients on demographic and clinical variables (P > 0.05). Thus, Type D personality was not a function of NYHA functional class, LVEF or etiology of heart failure. Furthermore, no significant differences were found between Type Ds and non-Type Ds on the prescription of drugs (P < 0.05).
Type D patients reported impairment in health status more often than non-Type Ds (18/38 = 47% versus 11/46 = 24%, P = 0.027). They were also more likely to suffer from depressive symptomatology; namely 18 of 38 = 47% versus 6 of 46 = 13%, P = 0.001.
Type D personality, health status and depressive symptoms
In univariate analyses, Type D personality was associated with impaired health status and more depressive symptoms (Fig. 1). Age, gender, NYHA classification, LVEF and etiology of CHF were not significantly related to these endpoints in univariate analyses (Table 2).
When adjusting for severity and etiology of CHF, age, and gender, Type D personality was independently related to health status (OR 3.3, 95% CI 1.21–9.09) and depressive symptoms (OR 7.1, 95% CI 2.23–22.39) (Table 3).
Type D personality and mood status
In univariate analyses, Type D patients were more likely to experience negative effect and less likely to experience positive effect (Fig. 1). Type D personality remained a significant associate of negative effect (OR 3.4, 95% CI 1.26–9.23) and positive effect (OR 0.3, 95% CI 0.09–0.81) when controlling for severity and etiology of CHF and demographic variables. However, lower NYHA functional class (OR 3.7, 95% CI 1.07–12.61) and younger age (OR 0.9, 95% CI 0.91–0.99) were also independently associated with more positive effect in multivariate analyses (Table 3).
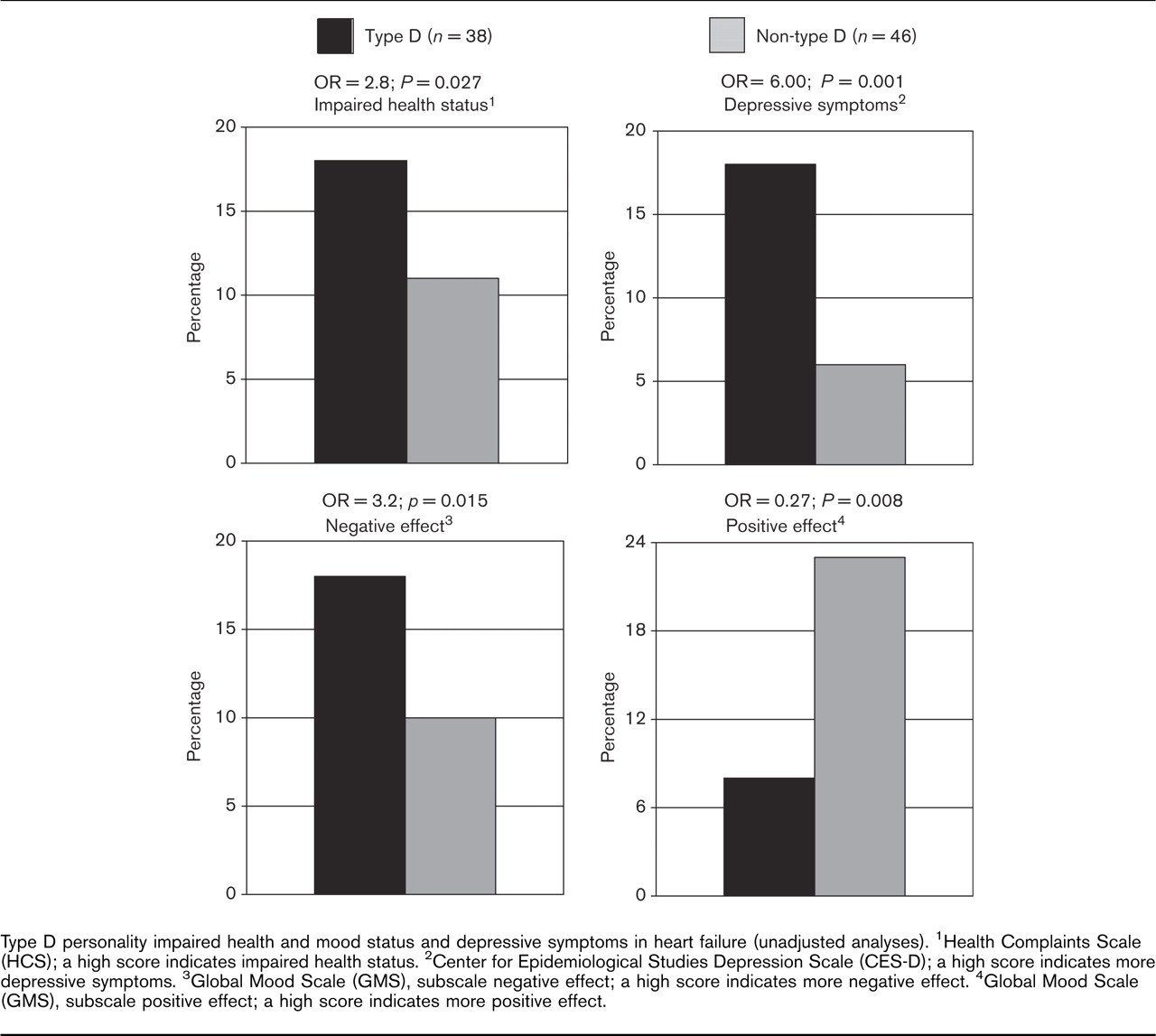
Type D personality impaired health and mood status and depressive symptoms in heart failure (unadjusted analyses). 1Health Complaints Scale (HCS); a high score indicates impaired health status. 2Center for Epidemiological Studies Depression Scale (CES-D); a high score indicates more depressive symptoms. 3Global Mood Scale (GMS), subscale negative effect; a high score indicates more negative effect. 4Global Mood Scale (GMS), subscale positive effect; a high score indicates more positive effect.
Relationship between clinical and demographic factors, health status and depressive feelings (unadjusted analyses)
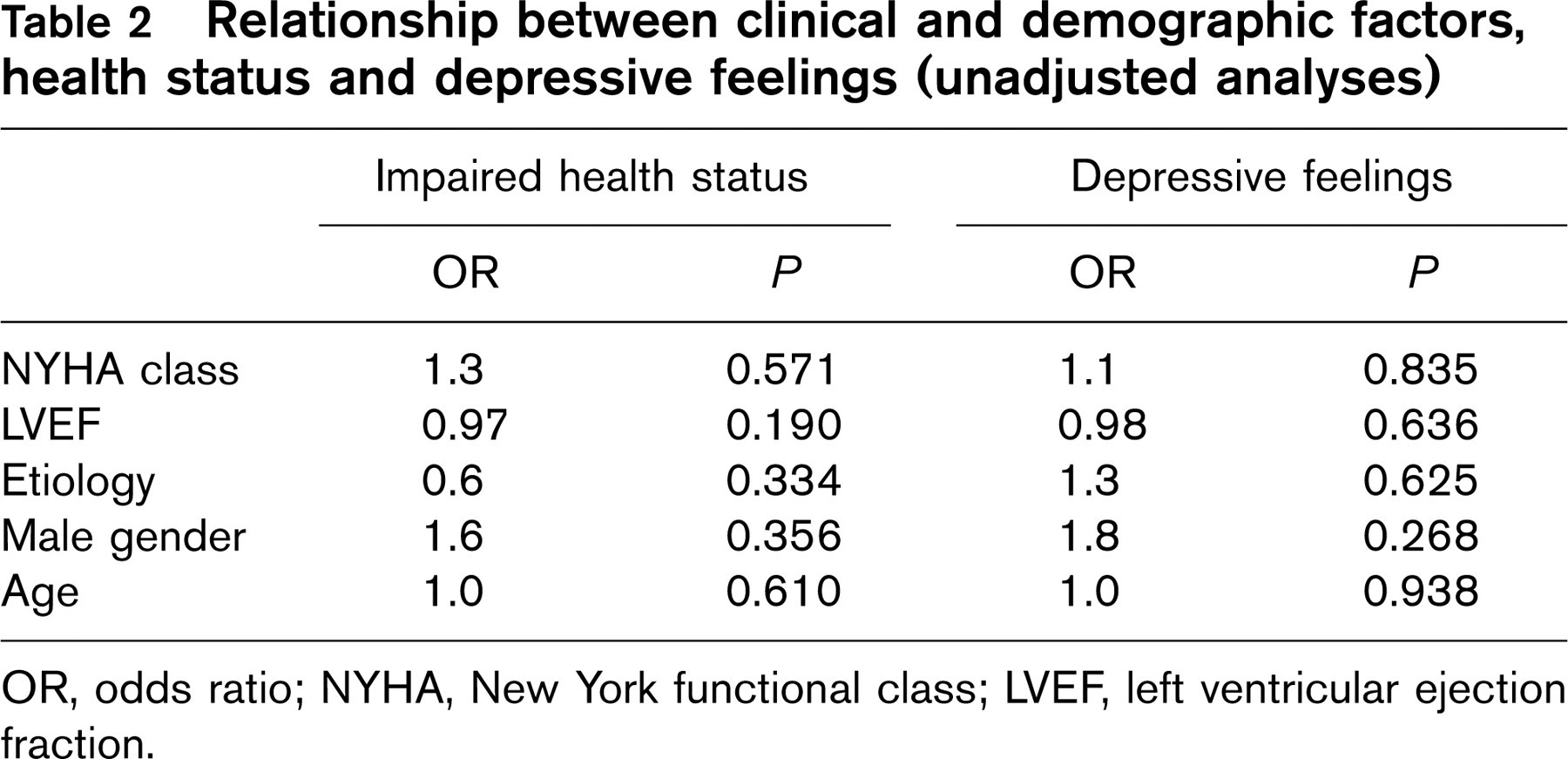
OR, odds ratio; NYHA, New York functional class; LVEF, left ventricular ejection fraction.
Discussion
As mentioned by Albus et al. [25], there is evidence that psychological factors like Type D personality contribute to the development and adverse outcome in CHD. To our knowledge, this is the first study to examine the influence of personality on health status and mood status in patients with CHF. Type D patients were more likely to have poor health status, increased depressive symptoms and impaired mood status compared with non-Type Ds. These associations remained significant when adjusting for severity (NYHA functional class) and etiology of CHF, gender, and age. Characteristics of CHF, namely NYHA functional class and LVEF, were not related to any of the outcome measures. This means that clinical measures of CHF are not related to health and mood status, and depressive symptoms, but Type D personality is.
Type D personality as a determinant of health status, depressive symptoms and mood status (adjusted analyses)
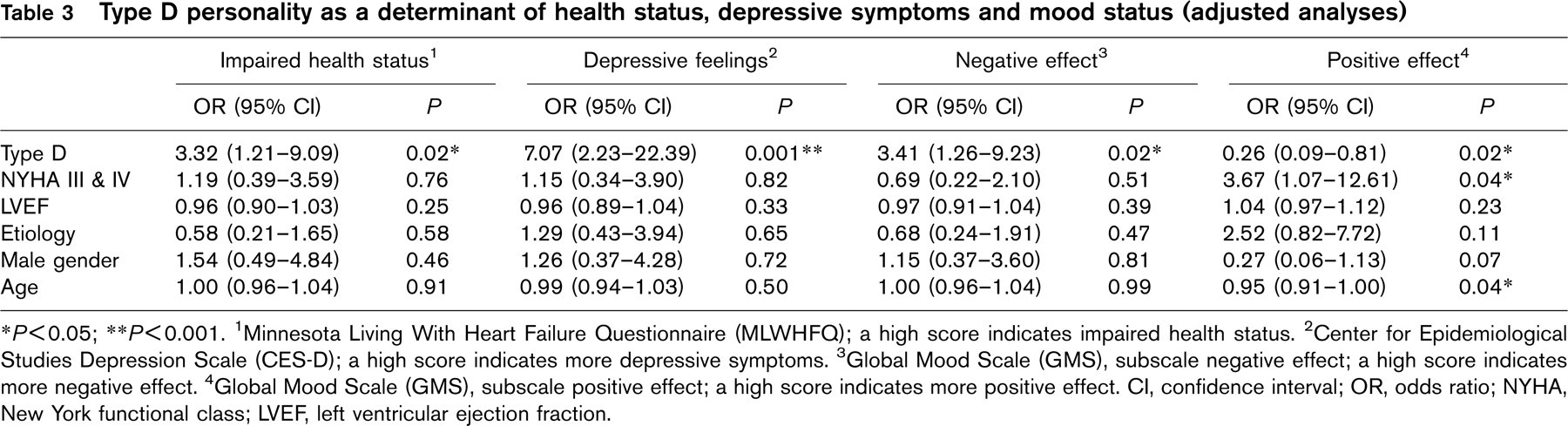
∗ P<0.05; ∗∗ P<0.001.
1 Minnesota Living With Heart Failure Questionnaire (MLWHFQ); a high score indicates impaired health status.
2 Center for Epidemiological Studies Depression Scale (CES-D); a high score indicates more depressive symptoms.
3 Global Mood Scale (GMS), subscale negative effect; a high score indicates more negative effect.
4 Global Mood Scale (GMS), subscale positive effect; a high score indicates more positive effect. CI, confidence interval; OR, odds ratio; NYHA, New York functional class; LVEF, left ventricular ejection fraction.
The results of the current study concur with studies having investigated the role of personality on quality of life in patients with acute coronary syndromes (ACS). These patients are at risk of developing CHF. In a prospective study of patients with ACS, Type D personality was found to be a predictor of impaired quality of life at 5 years follow-up [13]. In ACS patients, personality factors, such as Type D, have also been related to hard medical outcome [13–15], as has neuroticism in patients with CHF [12]. Furthermore, a recent study showed that Type D patients treated for arrhythmia with implantable cardioverter defibrillator (ICD) therapy experienced more anxiety and more depressive symptoms than non-Type Ds treated with ICD [18].
In previous research on depression and CHF, there has been a focus on the prevalence of depressive symptoms in CHF and the association between depression and prognosis in CHF [9, 11, 26]. Only one study has examined the role of depressive symptoms as a predictor of health status in patients with CHF [3]. Rumsfeld et al. [3] found depressive symptoms to be a strong predictor of worsened health status in CHF adjusting for baseline health status and over 20 patient variables. Ruo et al. [27] found similar results among patients with CHD. Recently, Gottlieb et al. [6] found the presence of depression in patients with CHF to be associated with reduced quality of life scores. No study, however, examined which factors are important in determining the depressive feelings that are so common in CHF.
Furthermore, although some studies have suggested an association between depression and personality traits, such as neuroticism [28] and alexithymia [29], and between depression and personality pathology [30], no study has examined the role of normal personality constructs as possible determinants of depressive feelings in CHF patients specifically. We found Type D personality, a personality type that is not characterized as psychopathology, to be an important associate of depressive feelings in patients with heart failure.
This study has a number of limitations. First, the cross-sectional design of the study does not allow for determination of cause and effect. Second, the number of patients was relatively small, which limits generalization of the results and the number of variables that can be controlled for in statistical analyses. Third, we did not include information on pacing techniques and other types of CHF treatment, because all patients included in this study were optimally treated by a cardiologist and a specialized heart failure nurse. Fourth, there is an overlap between symptoms of heart failure and depression. A diagnostic interview with a psychologist would provide better information on this issue.
Despite these limitations, this study is the first to investigate the role of Type D personality as an associate of health and mood status in heart failure patients. Moreover, the study was based on an unselected group of outpatients.
In conclusion, these preliminary findings suggest that Type D personality may be associated with adverse health status, increased depressive symptoms and impaired mood status in patients with CHF. The results also demonstrate that it may be worthwhile to include personality factors in future studies of patients with CHF, as personality may be an important explanatory factor of individual differences in outcome. Large-scale studies are now warranted to confirm these results.