
Abstract

Introduction
As the final pathway for the myriad diseases that affect the heart, the syndrome of heart failure (HF) is a growing epidemic. Although considerable progress has been made in the pharmacological management of patients with HF, the social and personal burden of HF is still characterized by debilitating symptoms, frequent re-hospitalizations and a high rate of mortality [1]. Additional factors such as the existence of multiple co-morbidities, an ageing population, potential interaction among multiple medications and psychological impact combine to augment the complexity of HF management. As such, HF is a chronic, costly and life-threatening disorder that constitutes a significant burden for both patients and the health care system.
The traditional model of care delivery is thought to contribute to frequent hospitalizations because in these brief episodic encounters little attention is paid to the numerous barriers to effective HF treatment and to common modifiable factors that are the cause of many hospital readmissions. In the face of these limitations, it is recognized that a HF disease multidimensional management programme is necessary to curb the rising cost of management and to improve morbidity and mortality [2].
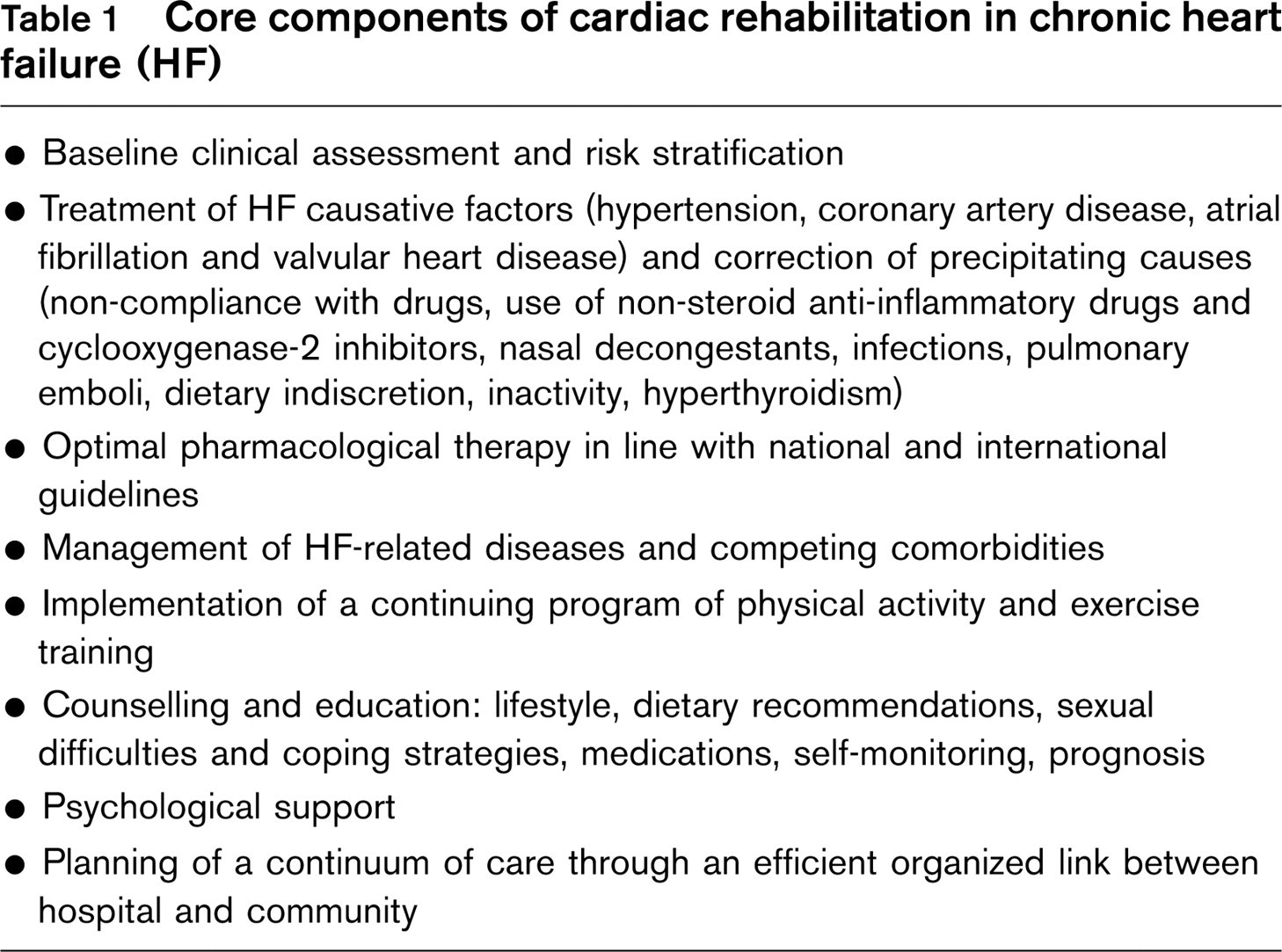
Cardiac rehabilitation is the ideal comprehensive structured disease intervention since it best addresses the complex interplay of medical, psychological and behavioural factors facing chronic HF patients and carers [3]. It is a coordinated multidimensional intervention designed to stabilize or slow disease progression, alleviate symptoms, improve exercise tolerance and enhance quality of life, thereby reducing morbidity and mortality. Core components of cardiac rehabilitation include baseline clinical assessment and risk stratification, optimal pharmacological therapy, management of HF-related diseases, non-pharmacological therapy in the form of an integrated management system with a continuing programme of physical activity, exercise training, counselling and education, and psychological support.
Despite the virtues of cardiac rehabilitation, only a small percentage of eligible HF patients ever get referred, due to barriers such as lack of physician and patient-family awareness of its benefits, and logistical or financial constraints. As such, HF is an example of a patient population that challenges cardiac rehabilitation with the need to employ active strategies to disseminate and implement appropriate standards of care.
To address this challenge, in January 2003, the Working Group on Cardiac Rehabilitation and Exercise Physiology of the European Society of Cardiology decided to promote a comprehensive framework for reviewing and describing the core components of cardiac rehabilitation in chronic HF. In this summary article, salient features of the position paper on core components of cardiac rehabilitation in chronic HF are provided.
Objectives
The aims of the Position Paper by the Working Group on Cardiac Rehabilitation and Exercise Physiology of the European Society of Cardiology are:
To provide advice for all health care practitioners dealing with chronic HF patients in the definition and development of cardiac rehabilitation programmes.
To describe the core components of a cardiac rehabilitation programme for patients with chronic HF.
To define a flexible multifactorial integrated management approach to ensure a continuum of care through an efficient organized link between hospital and community with programmed referral procedures and controls.
To broaden the indication for cardiac rehabilitation extending candidacy to all HF patients including those at high risk or most vulnerable, such as the elderly, patients with an implantable cardioverter defibrillator (ICD) or left ventricular assist devices, or heart transplantation recipients.
Core components of cardiac rehabilitation in chronic heart failure (HF)
Core components
The members of the Working Group on Cardiac Rehabilitation and Exercise Physiology of the European Society of Cardiology (ESC) recommended the need for a comprehensive strategy for HF patients in the cardiac rehabilitation setting, targeting the following components (Table 1).
First component: clinical assessment of patients with established heart failure
The 2001 American College of Cardiology/American Heart Association (ACC/AHA) Guidelines present a new classification of HF into four stages, from A (high risk for development of HF) to D (advanced HF) [4]. In contrast with the New York Functional Class (NYHA) classification, the evolution from stage A to stage D in the individual patient has no reverse path. The new classification based on clinical (symptoms) and laboratory presentation (left ventricular remodelling) underscores the progressive nature of HF and the fundamental preventive role of treatment strategies directed at reducing morbidity and mortality [5]. Careful history, physical examination, cardiac imaging and a new biochemical assay describing fluid status, functional capacity and cardiac rhythm should be performed for the accurate assessment of HF severity. Identification of factors contributing to worsening condition (arrhythmias, infection), comorbidities and chronic HF-related diseases can influence management strategies [6–8].
Second component: identification and management of chronic HF-related disease
As the disease progresses and the HF population ages, medications directed at the underlying pathophysiology of HF may not completely relieve symptoms. Specific treatments of HF-related disease (and co-morbidities) directed toward comfort are needed alongside medical management. Moreover, coexisting conditions are responsible for 40% of preventable short-term hospital readmissions.
Several chronic HF-related conditions (and co-morbidities), including depression, anaemia, renal insufficiency, cachexia, atrial fibrillation and sleep disorders [9–15], have been commonly observed in patients not enrolled in clinical trials. To guide disease management – in the new collaborative perspective – a more comprehensive assessment of precipitating factors and HF-related disease needs to be performed. Identification of factors that adversely affect quality of life or survival in HF may not only aid in better defining prognosis but also provide new opportunities for novel therapeutic strategies [16, 17].
Third component: pharmacological approach
A pharmacological approach based on evidence and guideline recommendations is fundamental in the management strategy of chronic HF. Current HF treatment includes agents that prolong life, alleviate symptoms and reduce hospital admissions. Moreover, the treatment of HF causative factors, including hypertension, coronary artery disease and dyslipidaemia increases the number of pharmacological agents that are necessary for many HF patients. The simultaneous presence of competing comorbidities further complicates the pharmacological management scenario. The ever-increasing complexity of polypharmacotherapy is daunting, causing these therapies not to be used, especially by practitioners who lack the time and expertise to pursue the kind of ‘micromanagement’ required with complex regimens. Although little evidence is available to guide polypharmacotherapy, collaborative disease management programmes that include a careful review of medications can provide an empirical tool that is a valid option for chronic HF with multiple comorbidities and polypharmacy [18].
Fourth component: non-pharmacological approach
Personal education and support of patient and carers is imperative [19]. A complete and continuous education programme for treating chronic HF patients, including information on causes of disease, drug regimen, dietary restrictions, physical and work activities, lifestyle changes and measures of self-control, will equip patients (and their carers) to play a more active role in management [20]. Understanding the information needs of patients and carers is vital, and good communication between healthcare professionals and patients/carers is essential. The content, style and timing of information should be tailored to the needs of individual patients, and cognitive ability should be assessed when imparting information [21]. Education should be delivered while the patient is in hospital and reinforced following discharge [22–24].
Fifth component: exercise training
Authoritative sources [25, 26] have established that individually tailored exercise training is well tolerated and produces positive adaptations in HF patients. Exercise training benefits have been reported in skeletal muscles, respiratory and cardiovascular systems and in their physiological responses to exercise. In the last 25 years, the applicability and efficacy of exercise training and a long list of impressive physiological gains achieved have been substantiated in thousands of selected stable chronic HF patients, overwhelmingly advocating that exercise training can be a highly cost-effective resource in chronic HF. According to the Working Group on Cardiac Rehabilitation & Exercise Physiology and the Working Group on Heart Failure of the European Society of Cardiology [25] and the American Heart Association Committee on Exercise, Rehabilitation, and Prevention [26] recommendations, exercise training should be prescribed to all stable chronic HF patients as a component of the multifactorial cardiac rehabilitation programme. After careful clinical, functional and risk stratification, and evidence-based medical therapy, exercise training programmes should be individualized for each patient, starting at a lower training intensity and for shorter session times for more debilitated patients. If facilities are available, resistance training may be incorporated as part of the overall exercise programme [27].
Sixth component: psychological support
Given the high morbidity and mortality associated with HF, it is not surprising that patients typically report psychological distress, reduced social functioning and diminished quality of life [10]. Nevertheless, until recently, the psychological correlates of HF have been somewhat neglected. Studies that address depression, anxiety, social support and coping style are beginning to emerge, documenting that either medications or cognitive behaviour therapy may bring improvements to the individual's quality of life, reduce the number of hospital admissions, and even lower mortality rate. Cardiac rehabilitation programmes offer an attractive conduit through which HF patients may be identified for incipient signs or symptoms of affective disease, allowing for initiation of potential specific interventions if indicated. Cardiac rehabilitation strategies appears to be cost-effective, decreasing psychological distress, improving coping skills and reducing some biological risk factors, such as social isolation and tobacco use.
Organizational aspects of cardiac rehabilitation in chronic HF
Cardiac rehabilitation is characterized by a continuum of services that spans inpatient and outpatient rehabilitation (Table 2). Inpatient rehabilitation should begin as soon as possible after hospital admission: every eligible HF patient should receive appropriate strategies for optimal therapy and have access to an individualized programme and, where possible, group education, according to clinical assessment and risk stratification. Education should be interactive with full participation of patient/carers: each intervention should be explained and the early mobilization programme should vary according to individual needs and hospital protocols. Progression of mobilization should be developed according to the patient's clinical condition, functional capacity, age, comorbidity with careful medical review and supervision. Education, reassurance and support, and mobilization should be part of routine daily care for every HF inpatient.
As the length of stay for acute HF and procedures continues to decrease, patient and family attendance in outpatient cardiac rehabilitation programmes assumes even greater importance. Structured outpatient cardiac rehabilitation, either residential or ambulatory, is crucial for the development of a life-long approach to prevention. Attendance should start soon after discharge from the hospital, ideally within the first few days. Different HF management programmes have been illustrated, and their content and the effectiveness of interventions vary widely [28, 29]. Outpatient cardiac rehabilitation may be provided in a range of settings, such as HF clinics, non-clinic settings (community health centres and general medical practices), or a combination of these [28]. Outpatient cardiac rehabilitation may also be provided on an individual basis at home, in a structured combination of home visits, telephone support (early telephone follow-up and continued telephone availability), telemedicine or specially developed self-education materials [28]. The main elements of outpatient cardiac rehabilitation include assessment, review and follow up, low or moderate intensity physical activity, exercise training, education, discussion and counselling.
Continuum of cardiac rehabilitation services
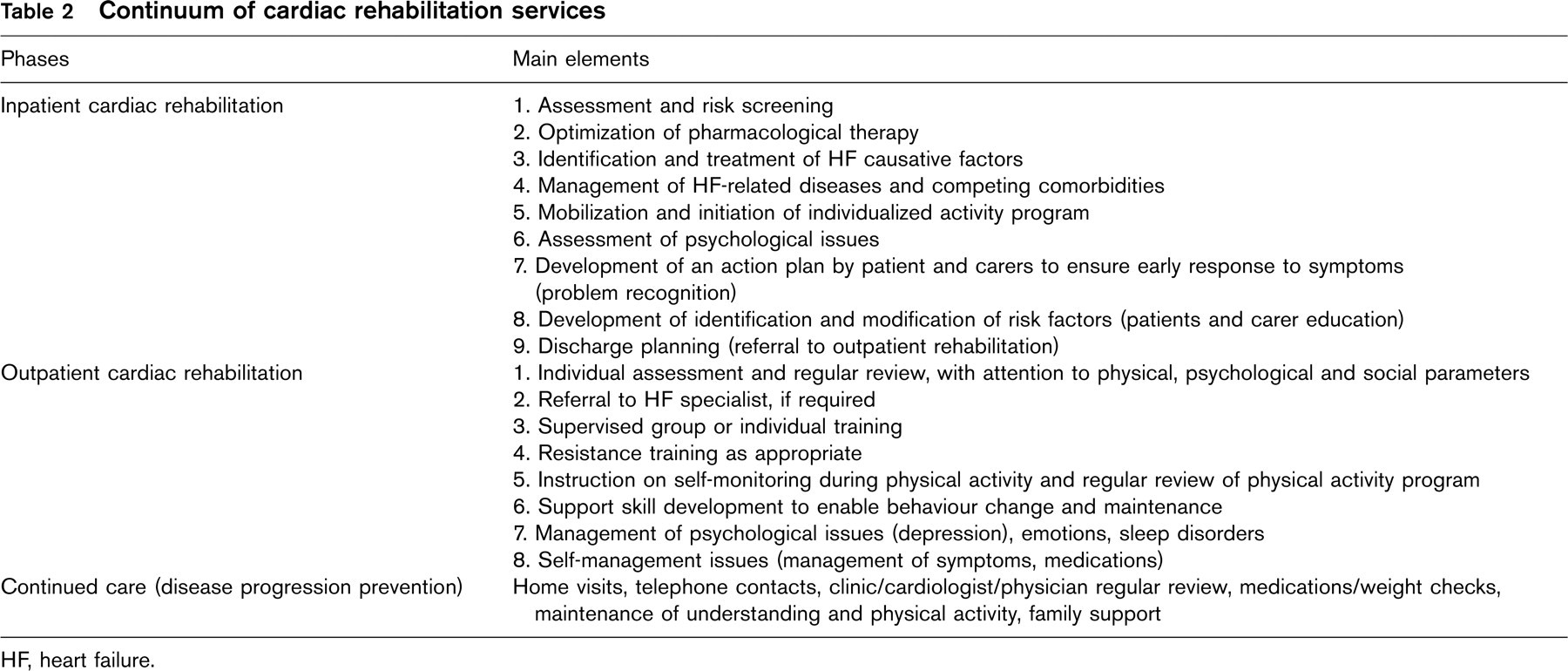
HF, heart failure.
Although a variety of disease management strategies with appropriate discharge planning and post-discharge support can, in the hands of experienced healthcare professionals, work in high-risk HF patients, patient education to enhance self-care, follow-up monitoring by specially trained staff, and access to specialized HF clinics seem the most effective approaches [28]. The need for a continuum of care is clear and the programme of self-care and prevention of lapses, recurrences and readmissions should be life-long. Evaluation of ongoing cardiac rehabilitation programme objectives on a regular basis is a key to success.
The recommended model for cardiac rehabilitation is delivered by a multidisciplinary team: team members have different backgrounds and training and therefore different areas of expertise. A designated programme coordinator is essential to ensure efficient running of the rehabilitation programme. The programme and medical director should be a cardiologist with good organizational, management and interpersonal skills.
Final remarks
Despite major advances in heart failure therapy, it is clear that medications alone are not the answer to the HF epidemic. Once the HF patient population has been characterized, it is important to ensure that all patients receive the proven level of effective care. Standards of treatment have been well delineated in the guidelines [4]. After the initial period of intervention, HF patients need continuous long-term support outside the hospital environment. Therefore, it is mandatory to promote and implement individualized discharge planning, therapeutic re-evaluation and continued patient education.
Cardiac rehabilitation is the ideal comprehensive flexible structured disease intervention: core components of cardiac rehabilitation include baseline clinical assessment and risk stratification, optimal pharmacological therapy, management of HF-related diseases, non-pharmacological therapy in the form of an integrated management project with a continuing programme of physical activity, exercise training, counselling and education, and psychological support. Indeed, cardiac rehabilitation is a uniquely structured comprehensive multidisciplinary intervention, with a flexible follow-up strategy, and offering patients easy access to the specialized HF team. All HF patients should attend a rehabilitation programme as soon as they are discharged from acute care institutions to assure clinical stability and to prevent hospitalizations.
Conclusions
Cardiac rehabilitation provides a specialized multifactorial management for all HF patients, in particular for patients at high risk, with advanced HF or recent hospitalizations, for the elderly and populations that are under-served or vulnerable. Cardiac rehabilitation is a highly effective strategy in the modern increasingly competitive health care climate. The future challenge for the Working Group on Cardiac Rehabilitation and Exercise Physiology of the European Society of Cardiology (ESC) and policymakers is to promote strategies to increase participation in cardiac rehabilitation programmes and to incorporate this management approach into future health care planning in an effort to deal with the current epidemic of chronic HF.