
Abstract
Background QT interval prolongation can lead to torsades de pointes, a potentially fatal arrhythmia. Although research exists on the relationship between QT prolongation and clinical outcome, few studies have described risk factors for prolonged QT interval in the general population.
Methods The Third National Health and Nutrition Examination Survey (NHANES III) collected electrocardiogram interval data on 8561 subjects over 40 years of age and projected results to the US population. QT was corrected for heart rate using Fridericia's formula. Logistic regression analyses were performed to identify factors independently associated with prolonged QTc interval, defined as being in the upper 5% of the population QTc interval distribution. Analyses were conducted separately for women and men as a result of differences in the QT distribution between the sexes and also because of potential effect modification. Analytical variables included age, race/ethnicity, electrolyte measurements, body mass index, the recent use of QT-prolonging drugs and past medical histories of stroke, thyroid disease, hypertension, diabetes and myocardial infarction.
Results Age, female sex, hypocalcemia (men), hypokalemia (women), and a history of thyroid disease and myocardial infarction (men) were associated with a prolonged QTc interval. In addition, taking QT-prolonging medications in the past month was associated with more than a twofold increase in the odds of prolonged QTc interval in both men and women.
Conclusions Healthcare practitioners should be aware that a prolonged QTc interval is a potential indicator of cardiovascular risk, and should exercise caution in prescribing potentially QT-prolonging medications to certain patients.
Introduction
Prolongation of the QT interval, as measured by an electrocardiogram (ECG), has been used as a tool to predict fatal arrhythmic events [1]. Although the true relationship between the QT interval and clinical outcome is unknown, some epidemiological studies have shown an increased risk of cardiac death among those with prolonged QT intervals [2–6].
Many factors including age, female sex, hypokalemia, cardiac disease and gene mutations have been implicated in QT interval prolongation [5, 7–9]. Drug effects on QT have also been identified, particularly in the light of fatal cardiac events associated with the use of terfenadine and cisapride [10–12]. Certain medications in classes such as anti-arrhythmics, antibiotics, antipsychotics and anti-depressants prolong ventricular repolarization, lengthening the QT interval [13].
Although much is known about the factors that prolong the QT interval, few have described the epidemiology of QT duration in a representative sample of the US population. We used data from the Third National Health and Nutrition Examination Survey (NHANES III) to describe QT interval measurements in the US population as well as to quantify the association between known risk factors and QT prolongation. The risk factor profile generated by this study may help healthcare providers avoid QT-prolonging medications in vulnerable populations.
Methods
NHANES III was conducted by the National Center for Health Statistics between 1988 and 1994, and focused on the health and nutrition of US residents 2 months of age and older. Details of the study design and sampling methods have been published previously [14]. Participants aged 40 years and above were eligible for a single resting 12-lead ECG. QT intervals were machine read and calculated using the Novacode ECG program [15].
Of 8561 subjects who underwent ECG testing, 194 were removed as a result of missing QT interval data or other key variables. This analysis is based on the remaining 8367 participants. The corrected QT interval (QTc), which adjusts for the effects of heart rate on QT duration, was the outcome variable of interest. In order to determine the most appropriate correction formula, QTc by heart rate was plotted for both Bazett and Fridericia equations and assessed with univariable linear regression models. As QTc corrects for heart rate, no relationship should exist between heart rate and QTc after correction has been performed (β = 0 for linear regression line). A visible association was evident with the Bazett correction (β = 0.92, P < 0.0001) but much less so with the Fridericia plot (β = −0.11, P < 0.0001). Therefore, Fridericia's formula was used for QT interval correction [16], and heart rate was included in subsequent regression models.
Analytical variables selected from the NHANES III dataset included age, sex and race/ethnicity (white, black, Mexican-American and other), as well as other variables previously found to be associated with QT prolongation such as serum calcium (<2.1 mmol/l = hypocalcemia) and potassium (<3.5 mmol/l=hypokalemia), and body mass index (BMI) [7]. We plotted BMI versus QTc interval and found a non-linear relationship, and categorized this variable based on plot results and known cutpoints for BMI: underweight (BMI < 18.5 kg/m2), reference (18.5 ≤ BMI < 30), obese (30 ≤ BMI <40) and very obese (BMI ≥40). Self-reported history of stroke, thyroid disease, diabetes, hypertension and myocardial infarction were also evaluated. Finally, we examined the effects of taking a potentially QT-prolonging drug such as certain antimicrobial, anti-emetic and antipsychotic agents in the past 30 days [10, 17]. Because QTc interval length is typically longer in women versus men, separate analyses were performed by sex [7, 8, 18].
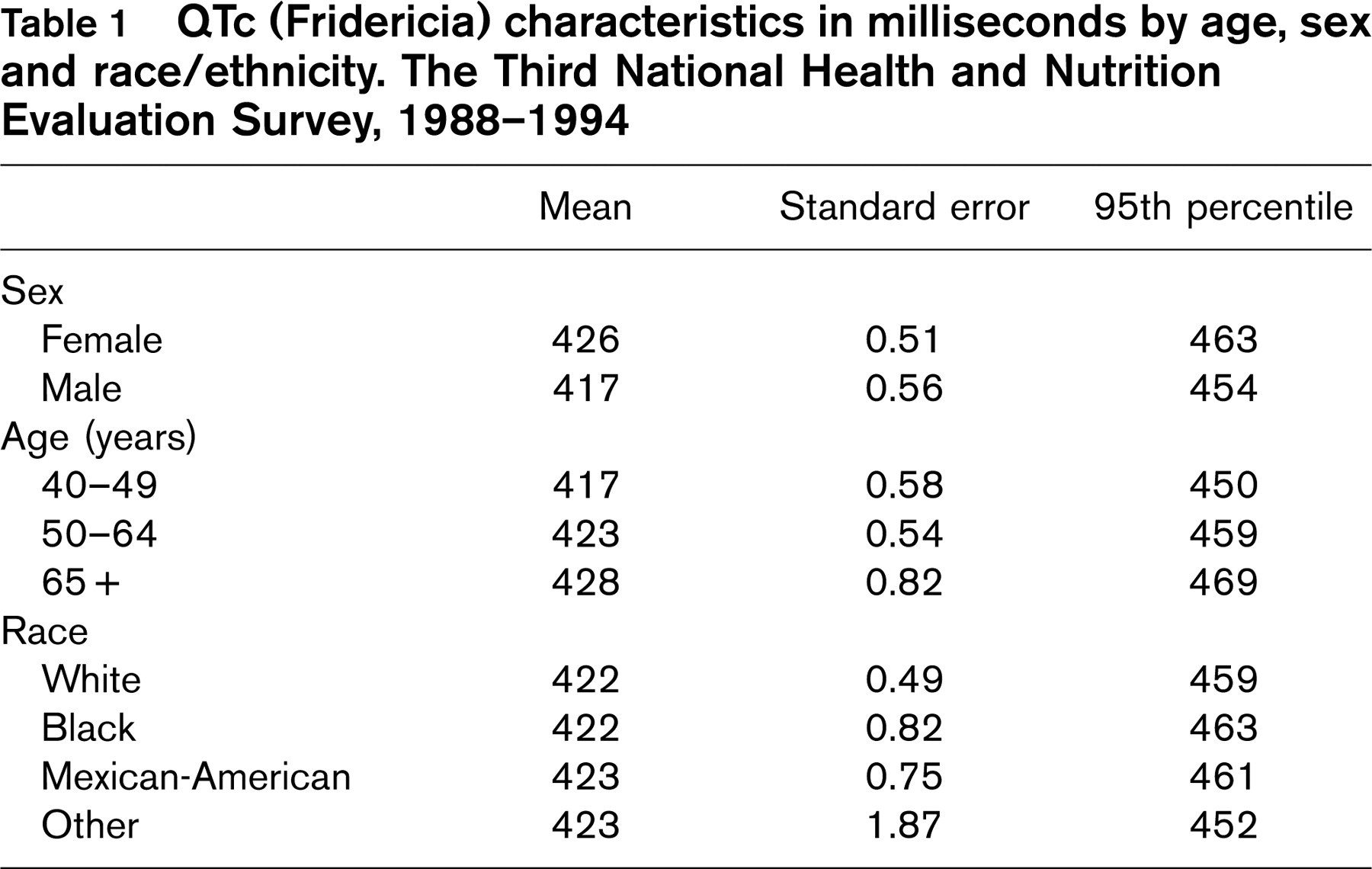
Analysis was conducted using logistic regression. QTc prolongation was defined as those subjects (cases) from NHANES III with QTc intervals falling into the upper 5th percentile of the QTc interval distribution. As there is no declared threshold of risk for QTc duration, studies differ in how QTc prolongation is defined. Our goal was to capture the risk factors of those at highest risk, and the upper 5th percentile was considered a reasonable cutpoint. Female cases represented participants with a Fridericia-corrected QTc greater than 463 ms and men greater than 454 ms (Table 1). The reference (controls) population for all comparisons was the remaining patients with ECG and QTc data.
SAS 8.02 (SAS Institute Inc., Cary, North Carolina, USA) and SUDAAN (8.0.2) (Research Triangle Institute, Research Triangle Park, North Carolina, USA) were used in data analyses. Sample weights were applied to provide nationally representative estimates and SUDAAN was used to calculate variance estimates given the complex, multistage survey design of NHANES III. Logistic regression was used to examine univariable and multi-variable associations with QTc prolongation. Although the Fridericia formula corrects for heart rate, no correction formula is ideal and therefore heart rate was included in all models [3]. All analyses utilized the weighted estimates from the NHANES III dataset. Diagnostics were assessed using tolerance values. All tolerance values were substantially greater than 0.10, indicating that collinearity among the independent variables was not present.
Results
QTc intervals were normally distributed within the population. The mean QTc was significantly longer in women than men (426 versus 417 ms, respectively, P < 0.0001), and was positively correlated with age (P < 0.0001) (Table 1, Figs 1 and 2). Little variation was noted in the QTc interval among racial groups, with white individuals having a mean interval of 422 ms; black individuals 422 ms; Mexican-American individuals 423 ms and others 423 ms.
QTc (Fridericia) characteristics in milliseconds by age, sex and race/ethnicity. The Third National Health and Nutrition Evaluation Survey, 1988–1994
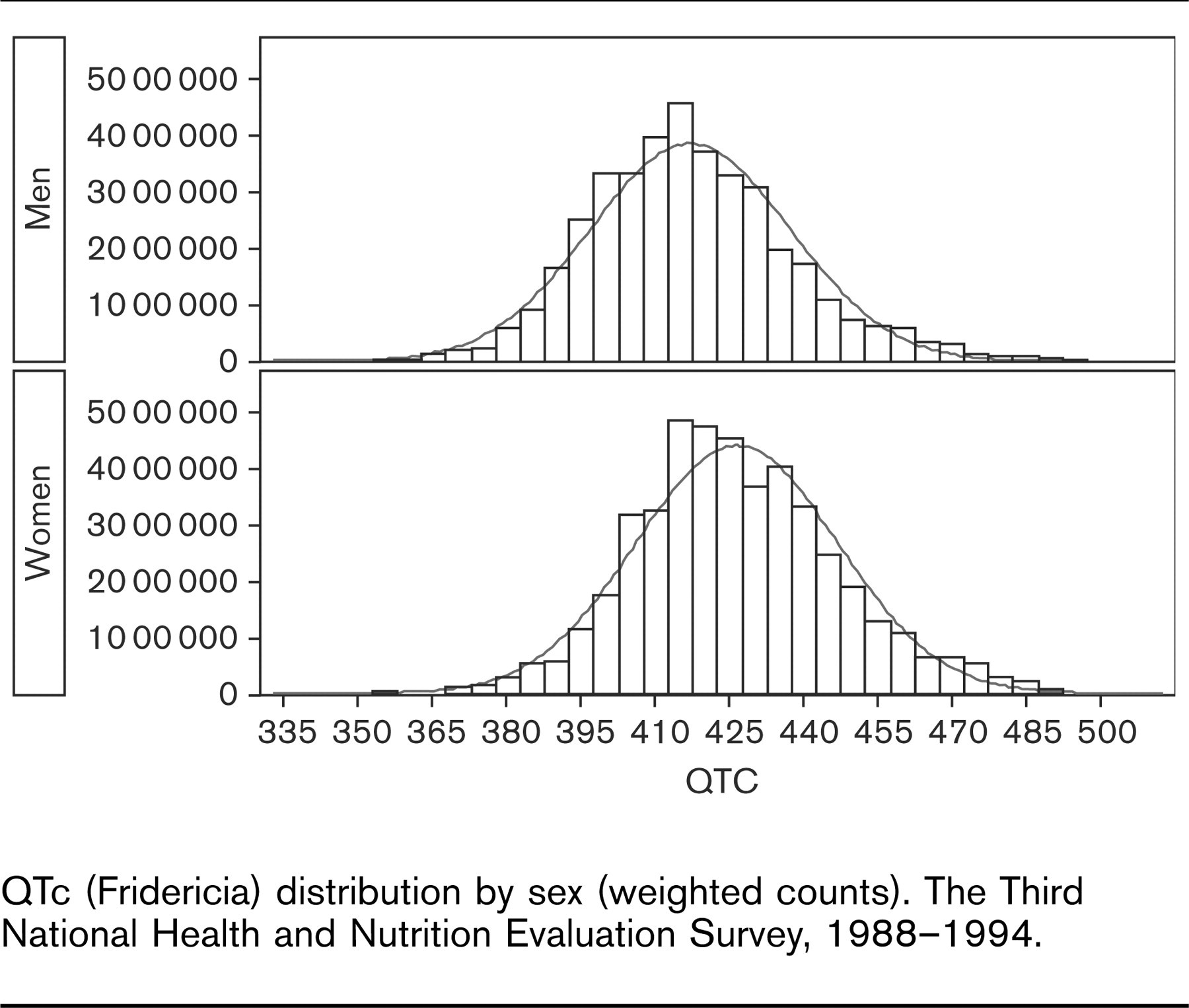
QTc (Fridericia) distribution by sex (weighted counts). The Third National Health and Nutrition Evaluation Survey, 1988–1994.
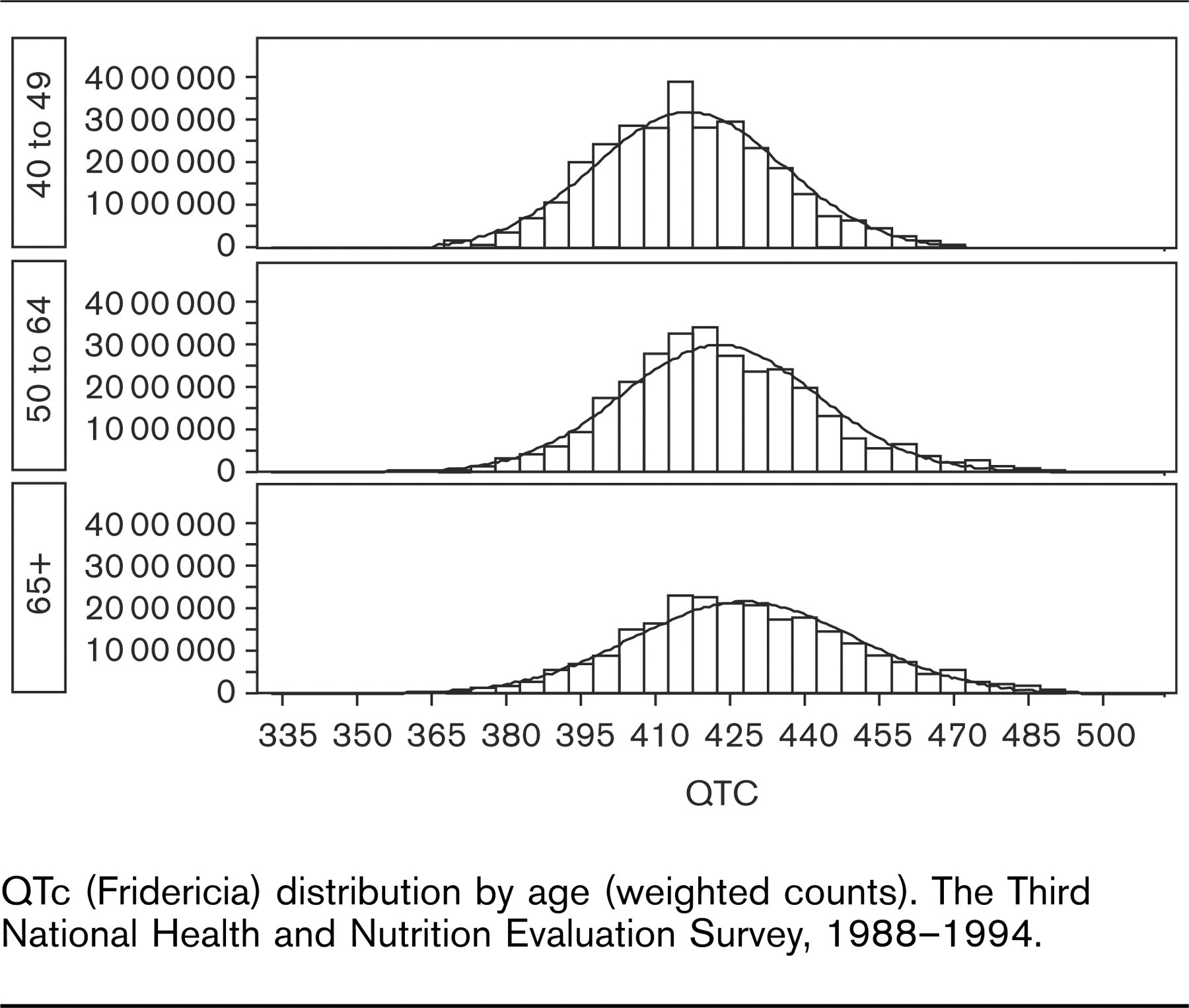
QTc (Fridericia) distribution by age (weighted counts). The Third National Health and Nutrition Evaluation Survey, 1988–1994.
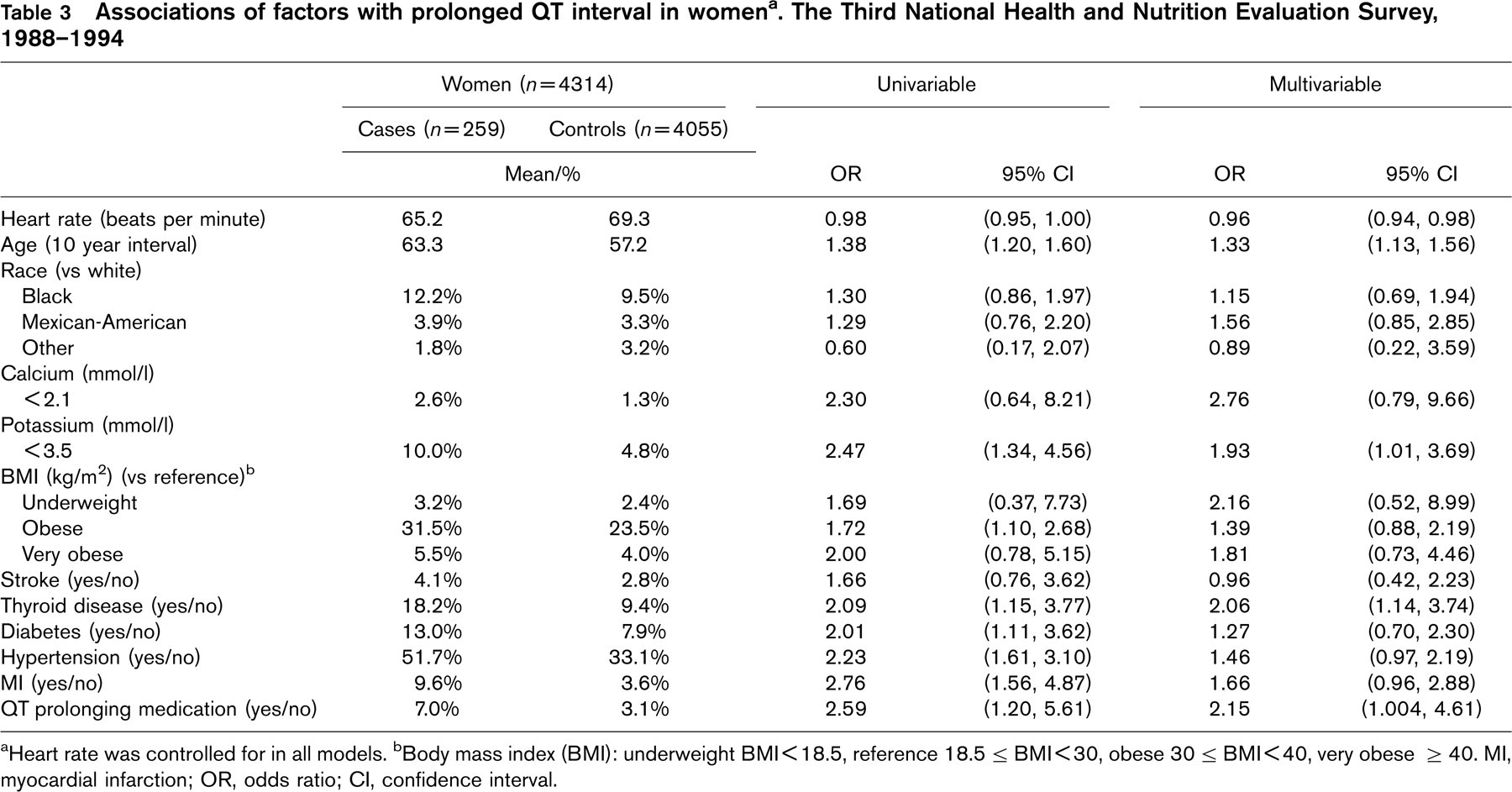
Of 4053 men and 4314 women, 270 and 259, respectively, qualified as cases of QTc prolongation (Tables 2 and 3). In univariable analysis, age, low potassium levels, and a history of thyroid disease, hypertension, myocardial infarction, and recent use of a QT-prolonging medication were significantly associated with a prolonged QTc interval for both women and men (Tables 2 and 3). In addition, male cases had higher odds of hypocalcemia [odds ratio (OR) 5.92] than male controls, whereas female cases had higher odds of being obese (OR 1.72) and having a self-reported history of diabetes (OR 2.01) than female controls.
Multivariable modeling showed a similar effect in men and women for age and history of thyroid disease. We also found that the recent use of QT-prolonging medications achieved statistical significance for both men [OR, 2.11; 95% confidence interval (CI), 1.002, 4.44] and women [OR, 2.15; 95% CI, 1.004, 4.61]. A sex effect was noted for several other variables. Hypocalcemia and a history of myocardial infarction were associated with QTc prolongation in men but not women and the opposite was true for hypokalemia (Tables 2 and 3).
Discussion
Consistent with previous findings, age, female sex, electrolyte disturbances, and a history of thyroid disease, hypertension, myocardial infarction and recent use of a QT-prolonging medication were associated with prolonged QTc intervals, in univariable or multivariable modeling, in this nationally representative sample. For both men and women, a history of thyroid disease or the recent use of QT-prolonging medications was associated with more than a twofold increased risk of having a prolonged QTc interval.
In a study of 2686 healthy middle-aged individuals, black men had a shorter QTc length than white men [19]. In the present study, no increased risk of QTc prolongation was found when comparing black and Mexican-American individuals to whites. A protective effect was found in the ‘other’ category compared with white individuals. This group made up 3.2% of the weighted sample and the racial/ethnic groups included are unknown, making interpretation difficult.
Hypocalcemia, hypokalemia and hypomagnesemia prolong ventricular repolarization, resulting in lengthened QTc intervals [20]. Sex differences were evident in this study for hypocalcemia and hypokalemia, with an association between QTc and hypocalcemia found in men, and an association for hypokalemia in women. Limitations, however, necessitate caution in interpreting these associations. Magnesium, not collected by NHANES, affects calcium levels and thus is a potential unmeasured confounder that could distort associations among these variables [21].
Obesity has been cited as a risk for QTc prolongation [22–26]. Limitations such as small sample size, lack of control group comparators and combining men and women in the analyses may explain discrepancies with the current study. Although univariable analysis did show a higher percentage of obese women in the case group, no association was found in multivariable modeling, suggesting that obesity is not an independent risk factor for QTc prolongation.
Associations of factors with prolonged QT interval in men a . The Third National Health and Nutrition Evaluation Survey, 1988–1994
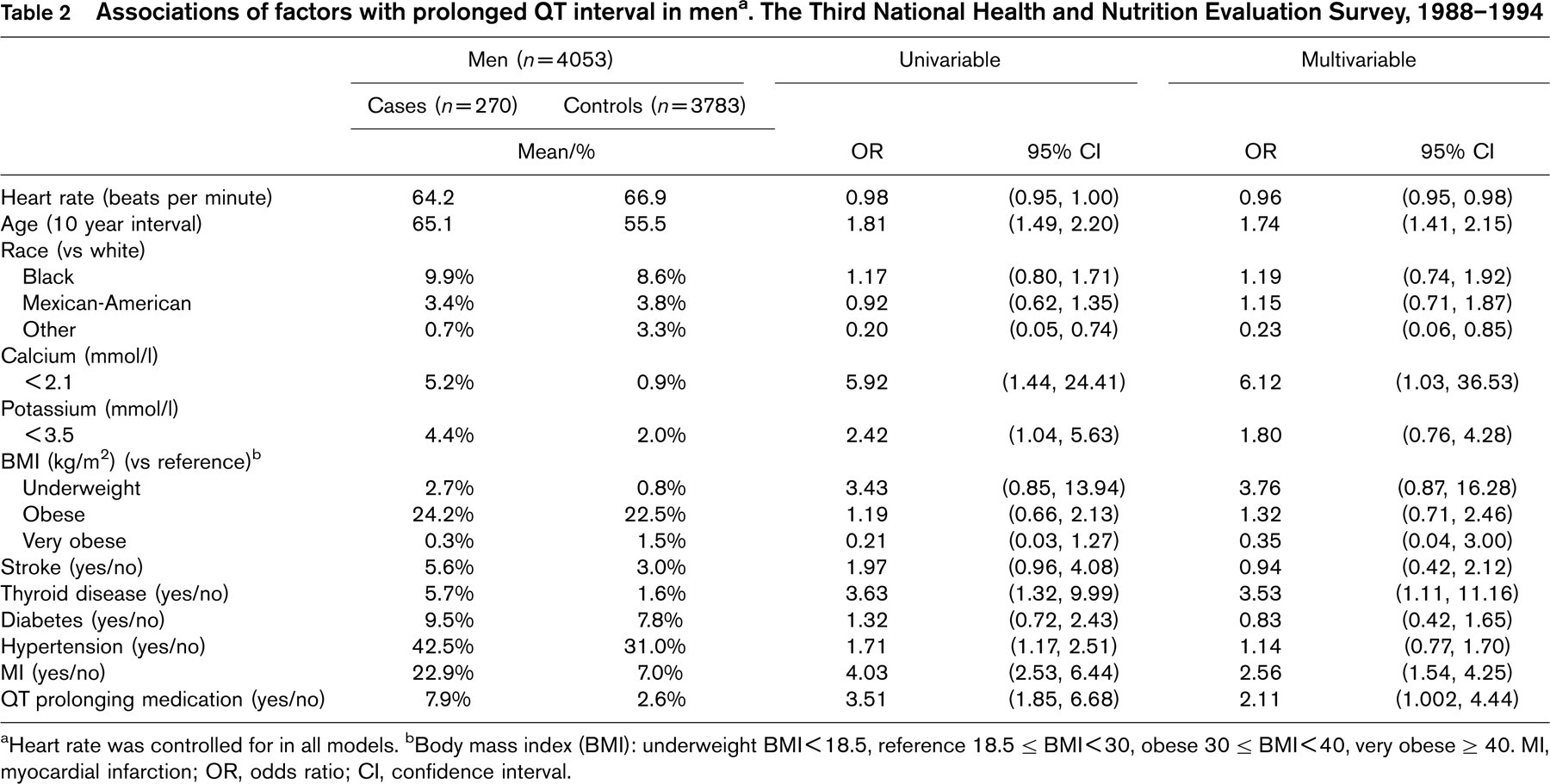
a Heart rate was controlled for in all models.
b Body mass index (BMI): underweight BMI<18.5, reference 18.5 ≤ BMI<30, obese 30 ≤ BMI<40, very obese ≥40. MI, myocardial infarction; OR, odds ratio; CI, confidence interval.
Associations of factors with prolonged QT interval in women a . The Third National Health and Nutrition Evaluation Survey, 1988–1994
a Heart rate was controlled for in all models.
b Body mass index (BMI): underweight BMI<18.5, reference 18.5 ≤ BMI<30, obese 30 ≤ BMI<40, very obese ≥40. MI, myocardial infarction; OR, odds ratio; CI, confidence interval.
Acute strokes can prolong QTc intervals [27], and stroke patients with prolonged QTc intervals are at a higher risk of cardiac death [28]. Individuals with type 2 diabetes who have prolonged QTc intervals are more likely to have strokes [29]. However, in our study, stroke by itself did not appear to be an independent risk factor for prolonged QTc.
A previous study using NHANES III data examined the relationship between QTc and diabetes, and found women (but not men) with diabetes to be more likely to have prolonged QTc intervals [25]. However, that study used Bazett's corrected QT formula, established cutpoints using terciles, and defined the upper tercile as a QTc of 440ms for both men and women. It also excluded patients with treated hypertension and those reporting a past myocardial infarction. Multivariable adjustment included age, race, heart rate and education, but failed to control for other factors such as electrolyte abnormalities and QT-prolonging medications. In our study, although diabetes was a significant risk factor in univariable analyses for women, it was not statistically associated with QTc in multivariable modeling. As Veglio and colleagues [30] demonstrated, QT interval length in diabetes is prolonged by complications and concomitant conditions such as ischemic heart disease, nephropathy, neuropathy and hypertension. Controlling for some of these factors here probably explains why diabetes was not found to be an independent risk factor for QTc prolongation in our study.
QT-prolonging drugs were independent risk factors for QTc prolongation in both men and women. This variable was based on self-report, included only medications consumed in the past 30 days and did not address the length of therapy. Despite these limitations, our results emphasize the potential population impact of the widespread use of QT-prolonging drugs in the general US population.
This study had a number of limitations. First, the QTc was measured and calculated based on one ECG reading. The QTc interval varies throughout the day and can be affected by factors such as sleep or meals [31–33]. The time of day of NHANES III ECG was not standardized, which could result in variability of the data. However, we have no reason to believe that there was a systematic variation in the time of day ECG were performed between cases and controls. In addition, debate exists over the most precise QT interval measurement technique. NHANES III used an automated method that may fail to define the end of the T wave precisely or differentiate T from U waves [34]. Nonetheless, studies have found similar results between automated and manual readings [35], and consistent measurements were maintained between cases and controls.
The QTc interval may be affected by multiple factors not accounted for in this study. Genetic determinants, meals, sleep, alcoholism, cardiomyopathy, cirrhosis and electrolyte imbalances such as magnesium have been shown to be risk factors for QTc prolongation [7]. NHANES III either did not collect information related to these factors or data were too incomplete to permit analyses. Whether the magnitude or direction of the findings for the variables considered in this study would change with the inclusion of these other factors is unknown.
The validity of NHANES data could also introduce misclassification bias. A history of stroke, thyroid disease, diabetes, hypertension and myocardial infarction were acquired from patient responses and were not validated by medical records. Such misclassification would probably be non-differential with respect to QTc, and thus would reduce the strength of association between these factors and QTc prolongation. Although agreement between self-report and medical records varies depending on the condition, self-report is reasonably accurate for well-defined diseases such as diabetes, and cardio- and cerebrovascular disease [36–39]. Results, however, vary depending on age, education and the population studied [40].
Multiple QT correction formulas exist to account for heart rate. Bazett's equation is most commonly applied, but overcorrects for heart rates above 60 beats per minute (bpm) and undercorrects for heart rates less than 60 bpm [41, 42]. Although no formula is perfect, Fridericia's provides a more accurate QT correction and is preferable in most studies [42]. This was confirmed in our study in which plots of QTc by heart rate showed that the Fridericia correction provided a more robust estimate of QTc.
The strength of this study is that it provides an epidemiological description of the QTc interval based on a representative sample of the US adult population. Previous studies described QTc in various populations as a predictor of a clinical outcome. Others looked at the relationship between QTc and specific risk factors. This is the first study that attempts to incorporate most of the suspected QTc interval-prolonging risk factors and quantify their magnitude of association in the general population. Given sex differences in the QTc interval distribution, men and women were analysed separately, and conservative cutpoints for QTc prolongation were established by identifying the upper 5% extreme of the normally distributed QTc interval curve for each sex. Upper limits of 470ms for women and 450ms for men (using Bazett's correction) have been proposed as prolonged QTc intervals [43]. Using Bazett's equation, our QTc cutpoints were 476 ms for women and 464ms for men, both above the proposed upper limits of normal. Therefore, this study identified the risk factors associated with the most pronounced QTc interval prolongation; factors that may be important for the development of future cardiovascular arrhythmias.
In summary, this study found that age, female sex, serum electrolytes, a history of thyroid disease, myocardial infarction (in men) and the use of a QT-prolonging medication in the past month were strongly associated with being in the upper 5% tail of the QTc distribution. Those who fall into this upper extreme may be at higher risk of sudden cardiac death as a result of the fatal arrhythmia known as torsades de pointes [10, 44]. Until future genetic and molecular studies better delineate the functionality of cardiac channel variants and the risk of sudden cardiac death [45], this study's QTc risk factor information may aid healthcare providers in avoiding additional risk in vulnerable populations. Assessing patient age, sex, serum electrolytes and medical history may help determine whether a screening ECG is warranted before prescribing medications that have the potential to prolong the QT interval.