
Abstract

The curse on today's clinical trials
The advances made in clinical cardiology in recent years are truly remarkable: large-scale randomized trials have provided a solid evidence base for adequate pharmacotherapy in most clinical settings. The investigation on combination therapies has provided guidelines for choosing the optimal treatment for the individual patient. Yet, progress seldom comes without its inherent problems: today, clinical researchers find themselves in a situation where the guideline-oriented therapies are well established and have significantly reduced clinical event rates. As a consequence it becomes increasingly difficult to prove the additional clinical benefit of a novel therapeutic intervention added on top of the established therapy. The only way to increase the power of the study is to increase patient numbers and/or the dosage/intensity of the clinical intervention.
In this issue of the European Journal of Cardiovascular Prevention and Rehabilitation we may find an example of such a clinical study by Allemann and colleagues, which yielded unexpectedly negative results most likely due to small patient numbers and low-dose interventions. The author compared the effects of mild endurance training and pravastatin on endothelial function in patients with coronary artery disease (CAD). Despite the fact that both interventions have separately been effective in improving endothelial function in numerous clinical studies the authors come to the conclusion that ‘In patients with CAD and average cholesterol levels, ten weeks of treatment with mild endurance exercise training or with pravastatin failed to improve endothelium-dependent or independent vasomotor function in forearm resistance vessels'.
Now, do we have to revise our opinion on these two established interventions or is there something else that went wrong?
Why did pravastatin fail to improve endothelial function?
The clinical evidence that statin therapy improves endothelial function is overwhelming; as early as 1994 it was documented that 6 months of treatment with pravastatin (10–20 mg/day) improved endothelium-dependent coronary vasomotion in patients with hypercholesterolaemia [1]. Several other consecutive studies confirmed this finding in patients with CAD [2] and in hypercholesterolemic patients [3]. Significant changes in endothelium-dependent vasomotion were detected as early as after 2–4 weeks of treatment [4, 5]. Are the effects of statins on endothelial function low-density lipoprotein (LDL)-dependent? The clear answer from the literature is no. In the RECIFE (Reduction of Cholesterol in Ischemia and Function of the Endothelium) trial the changes in flow-mediated dilation during 6 weeks of pravastatin therapy were unrelated to decreases in total cholesterol and LDL levels [6]. Additional evidence arguing against an LDL-dependency of the vascular effects came from studies in normocholesterolemic subjects in whom a single statin dose improved endothelial function before changes in LDL or C-reactive protein (CRP) could be detected [7, 8]. These findings led to the postulation of intrinsic pleiotropic effects of statins.
Today we know that statins have a multitude of LDL-independent effects on the endothelial metabolism resulting in increased nitric oxide (NO) production and decreased reactive oxygen species (ROS) generation (Table 1). In addition, statins enhance the release of endothelial progenitor cells (EPCs) from the bone marrow by a PI3-kinase/Akt-dependent pathway [9].
Pleiotropic effects of statins on endothelial function
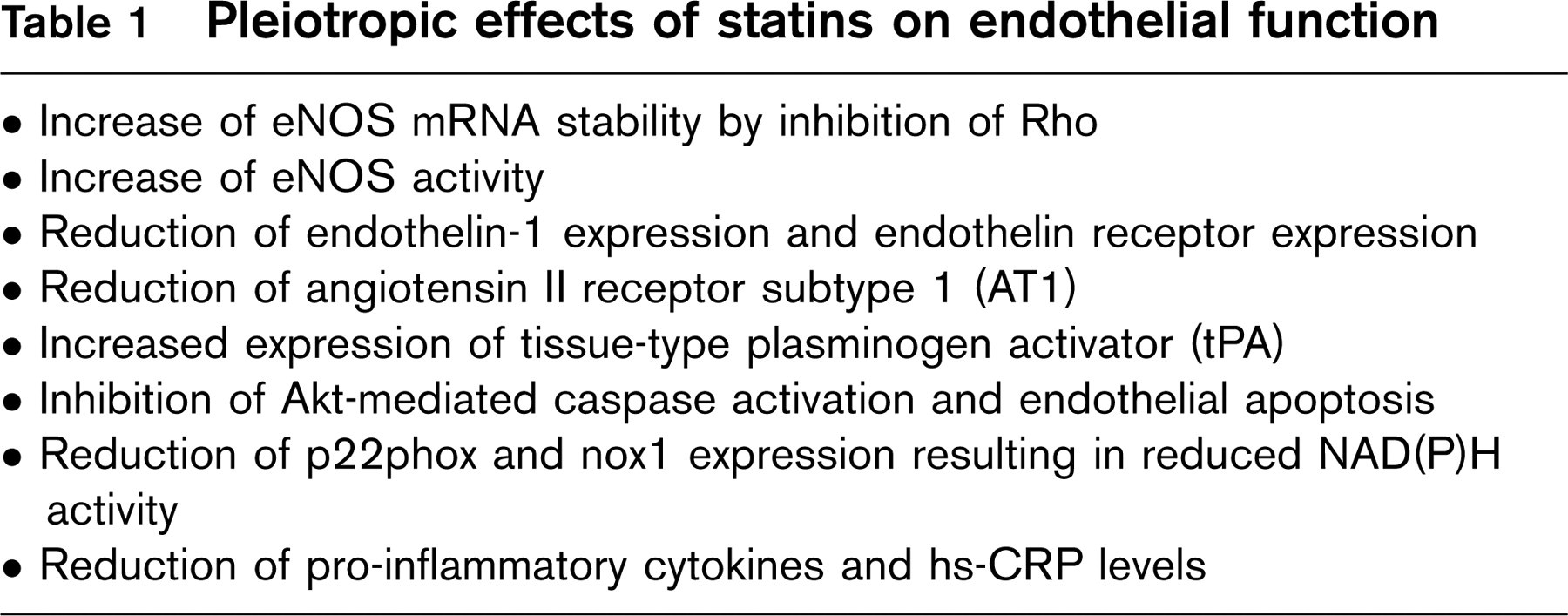
These EPCs have the ability to integrate into diseased areas of the endothelium and to replace dysfunctional endothelial cells resulting in improved endothelium-dependent vasomotion.
Given the plethora of pleiotropic statin effects on the vascular endothelium, the question of why statin therapy did not improve endothelial function in the study by Allemann becomes even more pressing. Fortunately enough, Vita and colleagues faced the same challenge when they found no difference in coronary endothelial function in CAD patients with mildly elevated cholesterol levels after 6 months of simvastatin therapy [10]. Among the proposed explanations for the discrepancy between their findings and those of other studies were: (1) subjects in this study had lower baseline total and LDL cholesterol levels; (2) less severe baseline atherosclerosis; and (3) relatively mild baseline endothelial dysfunction compared with subjects in studies in which improved endothelial function was observed.
Indeed CAD patients in the pravastatin group in Allemann's trial seem to have a low cardiovascular risk profile with normotensive blood pressure, an exercise capacity well above the age-adjusted average (166 ± 48 W), and only mildly elevated LDL-levels (148 mg/dL). All clinical conditions associated with severe endothelial dysfunction were excluded: clinical evidence of heart failure, arterial hypertension, peripheral vascular disease, diabetes mellitus, recent (≤ 3 months) transmural myocardial infarction and/or coronary artery bypass grafting (CABG), and current smoking. Presumably, all patients s/p interventional treatment of their CAD or peripheral vascular disease were excluded based on their continuing lipid-lowering therapy. It is no wonder that the authors end up with a low-risk patient cohort with mild endothelial dysfunction.
Why did mild endurance training fail to improve endothelial function?
To answer this question we have to remember the basic mechanisms of training-related effects on the vascular endothelium. The key stimulus for the endothelial cell is laminar shear stress. To generate an increased level of shear stress, subjects need to exercise at an intensity level that causes a hemodynamic response with increased cardiac output and vascular blood flow velocity. Therefore, most previous studies of exercise effects on vasomotion used strenuous programs with a training intensity of up to 70% of VO2max and a training duration of up to 60 minutes per day [11]. Allemann and colleagues trained their patients at a significantly lower intensity (the majority of patients (43 ± 9%) were between 50–60% of peak heart rate) for a much shorter duration of 180 minutes per week. Of this time, one-third was dedicated to walking, which is too low in intensity to elicit a significant hemodynamic response.
Previous studies have documented a clear relation between training duration and improvement of vascular endothelial function [12]. This observation provided a first hint that the previous results of cell culture experiments may also be valid in the clinical context: in cultures of human umbilical vein cells (HUVECs) exposed to different levels of steady laminar flow the increase in endothelial nitric oxide synthase (eNOS) expression [13, 14], phosphorylation [15], and NO production increased in proportion with the magnitude and duration of the shear stress applied. The same dose-response relation was also confirmed for pulsatile shear stress, which is closer to the in vivo situation with intermittent increases in blood pressure amplitude and flow [13].
In the case of the training intervention the combination of low-dose training with a low-risk patient cohort may explain the absence of any measurable vascular effects. This reinforces the old truth that there is probably no cardiac gain without some pain during exercise [16].
Why are studies with neutral or negative results important?
In the competitive environment of peer-reviewed journals negative or neutral clinical studies are severely underrepresented. As opposed to trials that show significant treatment effects neutral studies always face a number of methodological and statistical concerns from the reviewers who argue that the study was underpowered, the patient sample was too small, and the treatment period too short. However, the same arguments are also valid in any positive study (i.e., with significant results). We should remember the meaning of a significance level of P = 0.05. If you combine 20 variables with 50 others in chart and perform a chi-square test for each combination you will end up with 1000 P-values, of which 5% (i.e., 50) will be incorrectly ‘significant'. The relevance of this type I error in which the null hypothesis is rejected, although it is correct, is underestimated by most authors and reviewers.
Neutral or negative studies are important in two regards: whenever a new intervention has proved to be effective the impetus is: (1) to widen the range of clinical indications by testing it in different patient subgroups; and (2) to alter/reduce the dosage of the treatment. Therefore, neutral studies are necessary to determine the limits of the clinical indications and the lower end of the minimal effective dose. The study by Allemann and colleagues is valuable in this context in the sense that it shows the lack of effects of statin treatment or mild endurance training on vascular function in low-risk patients with stable CAD.