
Abstract

Introduction
Epidemiology
Blood pressure increases with age. Systolic blood pressure continues to increase throughout adult life, related to progressive arterial stiffening, whereas diastolic blood pressure plateaus in the sixth decade of life and decreases thereafter [1]. Blood pressure is lower in women than in men below the age of ∼ 50 years, rises more steeply in women around menopause and becomes higher in women than in men thereafter.
In recent epidemiological studies, hypertension was defined as systolic blood pressure ≥ 140 mmHg, and/or diastolic blood pressure ≥ 90 mmHg, or being on antihypertensive treatment. In Western Europe the prevalence of hypertension in the population amounts to ∼ 25%. When broken down by age and gender, the prevalence is approximately 15%, 30% and 55% in men aged 18–39 years, 40–59 years, and ≥ 60 years, respectively, and about 5%, 30% and 65% in women in these age groups. The prevalence of isolated systolic hypertension is very low before the age of 50 years, but increases sharply thereafter. These epidemiological data indicate that hypertension may already be present in the young athlete, though rarely, but will occur more frequently in the older sportsman. Unless blood pressure is measured, hypertension may remain undetected because it usually causes no symptoms. The global burden of hypertension is expected to increase from ∼ 26% to ∼ 29% between 2000 and 2025 [2].
However, ∼ 25% of patients with hypertension by conventional measurements have a normal blood pressure on 24-hour ambulatory monitoring or on home blood pressure measurements—so-called white-coat or isolated clinic hypertension [3, 4]. Young athletes with clinic hypertension often have normal blood pressure on ambulatory monitoring [5]. On the other hand, a small percentage of patients have masked or isolated ambulatory hypertension, which is characterised by a normal blood pressure in the office and an elevated blood pressure out-of-the office [6].
Hypertension as a cardiovascular risk factor
Hypertension is associated with an increased incidence of all-cause and cardiovascular mortality, sudden death, stroke, coronary heart disease, heart failure, atrial fibrillation, peripheral arterial disease and renal insufficiency. In the population at large, the relationship between cardiovascular complications and usual blood pressure is linear [7]. The prognosis of white-coat hypertension is better than that of sustained ambulatory hypertension and studies suggest that it is even similar to that of persons with true normal blood pressure, whereas patients with masked hypertension appear to have a worse outcome than true normotensives [3, 4, 6, 8].
Despite conclusive evidence that antihypertensive therapy reduces the complications of hypertension [1, 9], only about half of all patients with hypertension are under treatment and only a fraction of these have normal blood pressure [10, 11]. Systolic blood pressure appears to be more difficult to control than diastolic blood pressure, particularly in older patients.
Definition of hypertension
The classification of hypertension is based on multiple conventional blood pressure measurements, taken on separate occasions, in the sitting position, by use of a mercury sphygmomanometer or another calibrated device, according to established guidelines. Table 1 summarizes the definitions and classification of blood pressure levels, as adopted in the 2003 European Society of Hypertension, European Society of Cardiology guidelines for the management of arterial hypertension [1, 12]. The universally accepted blood pressure threshold for hypertension is 140/90 mmHg.
Twenty-four hour ambulatory blood pressure monitoring should be considered in cases of suspected white-coat hypertension, considerable variability of office blood pressure, marked discrepancy between blood pressure measured in the office and at home, and in subjects with high office blood pressure and low global cardiovascular risk. The current threshold for the definition of hypertension is 125/80 mmHg for 24-hour blood pressure. The threshold for daytime ambulatory blood pressure and the self-measured blood pressure at home is 135/85 mmHg. Patients above the threshold for conventional blood pressure and below the threshold for the out-of-office pressure are considered to have white-coat or isolated office hypertension and the reverse is true for masked or isolated ambulatory hypertension [1, 13].
Approximately 95% of patients with hypertension have essential or primary hypertension, which results from an interaction between genetic factors and lifestyle/environmental factors that include being overweight, high salt intake, excessive alcohol consumption and physical inactivity. The main causes of secondary hypertension involve renovascular, renal and adrenal abnormalities [1]. The role of blood pressure-increasing ergogenic aids should be considered in the hypertensive sportsman or athlete. Athletes may be taking large doses of prohibited substances such as anabolic steroids, erythropoietin, stimulants, and so forth. The uncontrolled use of these agents has been associated with numerous side effects including hypertension [14]. Also the use of non-steroidal anti-inflammatory drugs should be specifically considered, since these compounds may increase blood pressure [15] and are commonly used in the athletic setting. This also includes the newer COX-2 inhibitors [16].
Definitions and classification of clinic blood pressure levels (mmHg) [1]
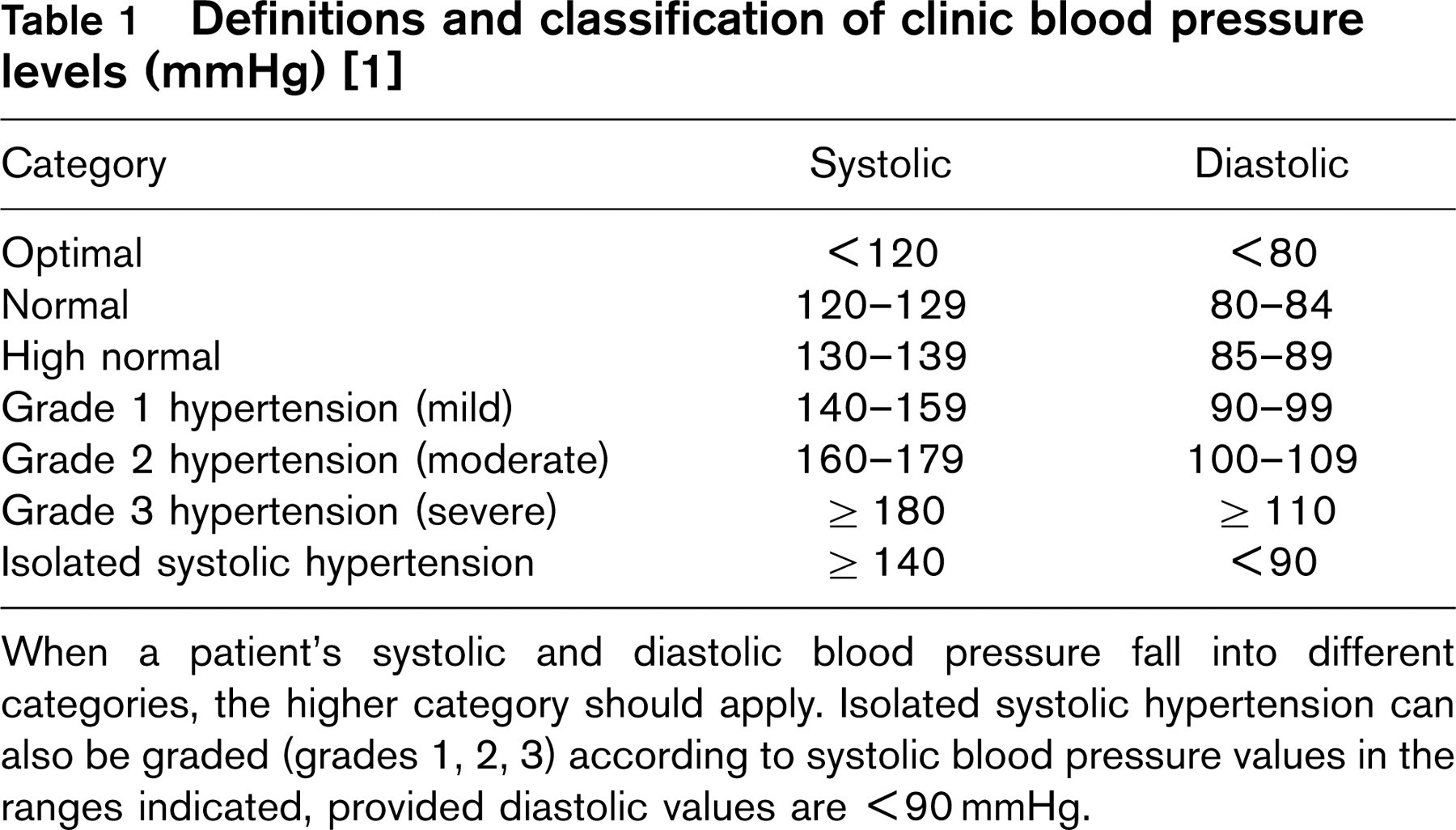
When a patient's systolic and diastolic blood pressure fall into different categories, the higher category should apply. Isolated systolic hypertension can also be graded (grades 1, 2, 3) according to systolic blood pressure values in the ranges indicated, provided diastolic values are <90 mmHg.
Assessment of the severity of hypertension and risk stratification
The severity of hypertension does not only depend on the blood pressure level (Table 1), but also on the presence of other cardiovascular risk factors, target organ damage and cardiovascular and renal complications. Table 2 summarizes the classification based on the overall cardiovascular risk [1, 12]. The terms low, moderate, high and very high added risk, in comparison with healthy normotensives without risk factors, are calibrated to indicate an approximate absolute 10-year risk of cardiovascular disease of < 15%, 15–20%, 20–30% and > 30%, respectively, according to the Framingham criteria, or an approximate absolute risk of fatal cardiovascular disease < 4%, 4–5%, 6–8% and > 8% according to the European SCORE system [17].
The risk stratification is based on the accumulated number of selected risk factors, on the presence of target organ damage and/or of associated clinical conditions, as outlined in Table 2. With regard to left ventricular hypertrophy, it should be noted that sports activity itself might induce hypertrophy; the type of hypertrophy and assessment of diastolic left ventricular function may help to distinguish between hypertensive heart disease and athlete's heart [18–21]. Athlete's heart typically shows maintained diastolic function, and is considered a physiological adaptation to training, in contrast to the hypertrophy secondary to hypertension. Hypertensive patients usually have concentric left ventricular hypertrophy but eccentric hypertrophy has also been described [22]. Whether or not hypertension in an athlete will trigger or accentuate the cardiac hypertrophy, or athletic exercise in a person with hypertrophy secondary to hypertension will worsen the hypertrophy, is not known.
The importance of the risk stratification is that patients at high or very high risk should be treated promptly with antihypertensive drugs, whereas patients at low or moderate added risk are only treated when hypertension persists despite lifestyle measures. An alternative way to estimate risk in those who are not at high or very high risk according to Table 2, is to use the European SCORE system [17].
Stratification of risk to quantify prognosis in patients with hypertension [1]
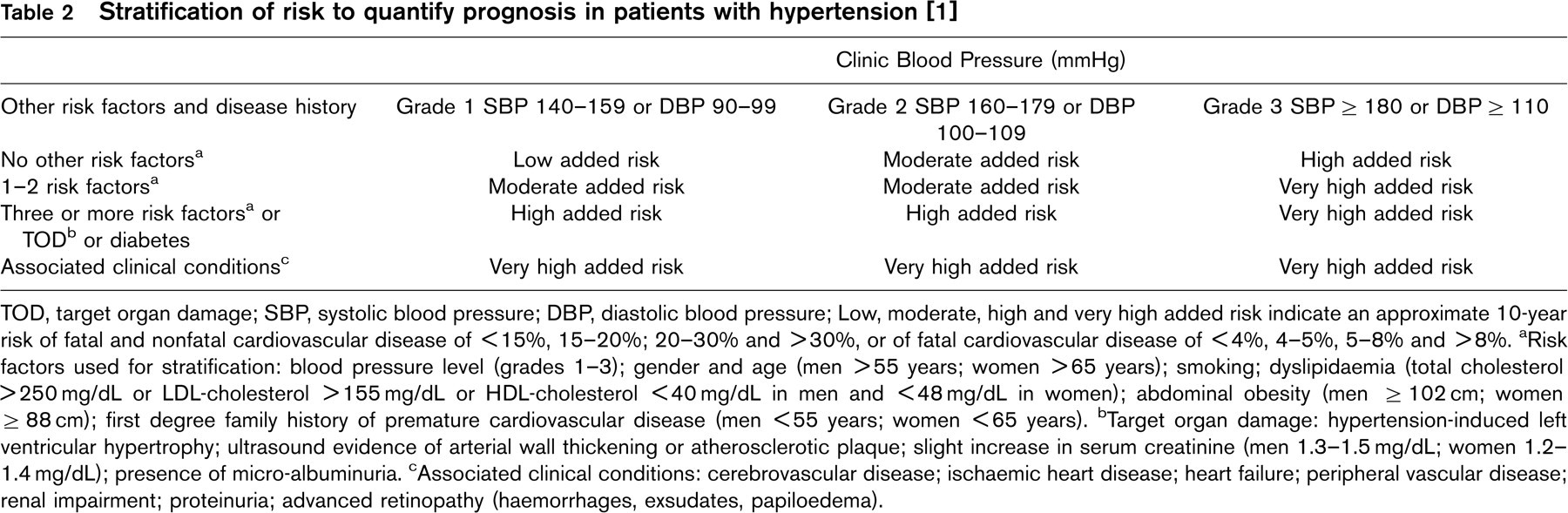
TOD, target organ damage; SBP, systolic blood pressure; DBP, diastolic blood pressure; Low, moderate, high and very high added risk indicate an approximate 10-year risk of fatal and nonfatal cardiovascular disease of <15%, 15–20%; 20–30% and >30%, or of fatal cardiovascular disease of <4%, 4–5%, 5–8% and >8%.
a Risk factors used for stratification: blood pressure level (grades 1–3); gender and age (men >55 years; women >65 years); smoking; dyslipidaemia (total cholesterol >250 mg/dL or LDL-cholesterol >155 mg/dL or HDL-cholesterol <40 mg/dL in men and <48 mg/dL in women); abdominal obesity (men ≥102 cm; women ≥88 cm); first degree family history of premature cardiovascular disease (men <55 years; women <65 years).
b Target organ damage: hypertension-induced left ventricular hypertrophy; ultrasound evidence of arterial wall thickening or atherosclerotic plaque; slight increase in serum creatinine (men 1.3–1.5 mg/dL; women 1.2–1.4 mg/dL); presence of micro-albuminuria.
c Associated clinical conditions: cerebrovascular disease; ischaemic heart disease; heart failure; peripheral vascular disease; renal impairment; proteinuria; advanced retinopathy (haemorrhages, exsudates, papiloedema).
Assessment of the risk associated with exercise
Exercise-related sudden death at a younger age is mainly attributed to hypertrophic cardiomyopathy, anomalies of the coronary arteries or arrhythmogenic right ventricular dysplasia [23–25], and is unlikely to be related to hypertension. On the other hand, coronary heart disease has been identified in approximately 75% of victims of exercise-related sudden death above the age of 35 years [26]. Whether or not high blood pressure is a cause of exercise-related sudden death on its own is not known, but hypertension is certainly a major risk factor for the development of coronary artery disease. In addition, hypertension-induced left ventricular hypertrophy may cause life threatening ventricular arrhythmias [27]. It is likely that the risk associated with exercise can be derived from the overall risk stratification (Table 2). Therefore, the general approach of the hypertensive patient should also apply to the exercising patient.
Diagnostic evaluation
Diagnostic procedures are aimed at: (1) establishing blood pressure levels; (2) identifying secondary causes of hypertension; and (3) evaluating the overall cardiovascular risk by searching for other risk factors, target organ damage and concomitant diseases or accompanying clinical conditions [1, 12]. Diagnostic procedures comprise a thorough individual and family history, physical examination, including repeated blood pressure measurements according to established guidelines, and laboratory and instrumental investigations, of which some should be considered part of the routine approach in all subjects with high blood pressure, some are recommended, and some are indicated only when suggested by the core examinations. Routine tests include: haemoglobin and haematocrit; serum potassium, creatinine and uric acid; plasma glucose; serum cholesterol and triglycerides; urine analysis; and standard electrocardiography. In addition, echocardiography and exercise testing with ECG and blood pressure monitoring are indicated as routine tests in the competitive athlete with hypertension [28].
Recommended tests include: carotid ultrasound; microalbuminuria; quantitative proteinuria; fundoscopy and high sensitive C-reactive protein. Extended evaluation may be necessary based on the findings from these investigations [1, 12]. The indication for exercise testing depends on the patient's risk and on the sports characteristics [29]. In patients with hypertension about to engage in hard or very hard exercise (intensity ≥ 60% of VO2max), a medically supervised peak or symptom-limited exercise test with ECG and blood pressure monitoring is warranted. In asymptomatic men or women with low or moderate added risk (Table 2), who engage in light-to-moderate dynamic physical activity (intensity < 60% of VO2max), there is generally no need for further testing beyond the routine evaluation. Asymptomatic individual patients with high or very high added risk may benefit from exercise testing before engaging in moderate-intensity exercise (40–60% of VO2max) but not for light or very light activity (< 40% of VO2max). Patients with exertional dyspnoea, chest discomfort or palpitations need further examination, which includes exercise testing, echocardiography, Holter monitoring, or combinations thereof.
A major problem with exercise testing in a population with a low probability of coronary heart disease and in subjects with left ventricular hypertrophy is that the majority of positive tests on electrocardiography are falsely positive. Stress myocardial scintigraphy or echo-cardiography, and ultimately coronarography, may be indicated in cases of doubt. There is currently insufficient evidence that the blood pressure response to exercise should play a role in the recommendations for exercise in addition to blood pressure at rest [30]. However, subjects with an excessive rise of blood pressure during exercise are more prone to develop hypertension and should be followed-up more closely [29]. Finally, physicians should be aware that high blood pressure may impair exercise tolerance [31].
Effects of exercise on blood pressure
Dynamic exercise
Blood pressure increases during acute dynamic exercise in proportion to the intensity of the effort. During longer-term stable exercise, the blood pressure tends to decrease after an initial increase of short duration. The increase is greater for systolic than for diastolic blood pressure, which only slightly increases or even remains unchanged. For the same oxygen consumption, the rise is more pronounced in older subjects and when exercise is performed with smaller than with larger muscle groups. Acute exercise is usually followed by post-exercise hypotension, which may last for several hours and is generally more pronounced and of longer duration in patients with hypertension than in normotensive subjects [29].
Cross-sectional and longitudinal epidemiological studies indicate that physical inactivity and low fitness levels are associated with (a) higher blood pressure levels and (b) increased incidence of hypertension in the population [32]. Recent meta-analyses of randomized controlled intervention studies concluded that regular dynamic training at moderate intensity significantly reduces blood pressure [33, 34]. Overall net changes averaged − 3.4/ − 2.4 mmHg, that is, after adjustment for control observations and after weighting for the number of participants. In normotensives the training-induced decrease in blood pressure averaged 2.6/1.8 mmHg, and in hypertensives 7.4/5.8 mmHg. There was no convincing evidence that the blood pressure response depended on training intensity when this was between ∼ 40% and ∼ 80% of maximal aerobic power [33].
Static exercise
Blood pressure increases during acute static exercise and the increase is more pronounced than with dynamic exercise, particularly with heavy static exercise at an intensity of > 40–50% of maximal voluntary contraction. In a recent meta-analysis of randomized controlled trials, ‘resistance’ training at moderate intensity was found to decrease blood pressure by 3.5/3.2 mmHg [35]. The meta-analysis included nine studies designed to increase muscular strength, power and/or endurance, and all but one study involved dynamic rather than purely static exercises. In fact, few sports are characterized by purely static efforts. However, only three trials in the meta-analysis reported on patients with hypertension.
Recommendations
General recommendations
Athletes with hypertension should be treated according to the general guidelines for the management of hypertension [1, 12]. Appropriate non-pharmacological measures should be considered in all patients, that is moderate salt restriction, increase in fruit and vegetable intake, decrease in saturated and total fat intake, limitation of alcohol consumption to no more than 20–30g ethanol/day for men and no more than 10–20 g ethanol/day for women, smoking cessation and control of body weight. Antihypertensive drug therapy should be started promptly in patients at high or very high added risk for cardiovascular complications (Table 2). In patients at moderate added risk, drug treatment is only initiated when hypertension would persist after several months despite appropriate lifestyle changes. Drug treatment is currently not considered mandatory in patients at low added risk. The goal of antihypertensive therapy is to reduce blood pressure to at least below 140/90 mmHg and to lower values if tolerated in all hypertensive patients, and to below 130/80 mmHg in diabetics.
Current evidence indicates that patients with white-coat hypertension do not have to be treated with antihypertensive drugs, unless they would be at high or very high risk (Table 2), but regular follow-up and non-pharmacological measures are recommended [1]. Also subjects with normal blood pressure at rest and exaggerated blood pressure response to exercise should be followed-up more closely.
Choice of drugs
Several drug classes can be considered for the initiation of antihypertensive therapy: diuretics; beta-blockers; calcium channel blockers; angiotensin converting enzyme inhibitors and angiotensin II receptor blockers [1, 12]. However, diuretics and beta-blockers are not recommended for first-line treatment in patients engaged in competitive or high-intensity endurance exercise [31]. Diuretics impair exercise performance and capacity in the first weeks of treatment through a reduction in plasma volume, but exercise tolerance appears to be restored during longer-term treatment; nevertheless diuretics may cause electrolyte and fluid disturbances, which are not desirable in the endurance athlete. Beta-blockers reduce maximal aerobic power by on average 7% as a result of the reduction in maximal heart rate, which is not fully compensated by increases of maximal stroke volume, peripheral oxygen extraction, or both. Furthermore, the time that submaximal exercise can be sustained is reduced by ∼ 20% by cardioselective beta-blockers and by ∼ 40% by non-selective beta-blockers, most likely as a result of impaired lipolysis [31, 36, 37]. In addition, diuretics and beta-blockers are on the doping list for some sports, in which weight loss or control of tremor are of paramount importance. Diuretics are also banned because they may be used to conceal the use of other doping agents, such as anabolic steroids, by diluting the urine samples. The hypertensive athlete who has to use a diuretic and/or a beta-blocker for therapeutic purposes should follow the ‘International Standard for Therapeutic Use Exceptions’ of the World Anti-Doping Agency (WADA).
Recommendation for strenuous leisure time physical activity and competitive sports participation in athletes with systemic hypertension (and other risk factors) according to the cardiovascular risk profile [28]
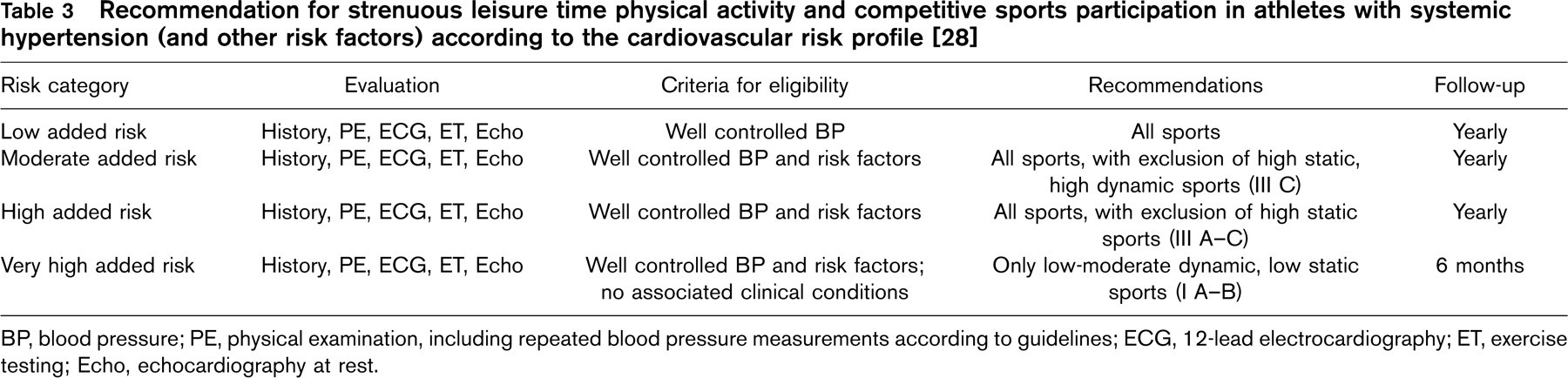
BP, blood pressure; PE, physical examination, including repeated blood pressure measurements according to guidelines; ECG, 12-lead electrocardiography; ET, exercise testing; Echo, echocardiography at rest.
Calcium channel blockers and blockers of the renin-angiotensin system are currently the drugs of choice for the hypertensive endurance athlete [31, 38] and may be combined in case of insufficient blood pressure control. However, the combination of an angiotensin-converting enzyme inhibitor and an angiotensin II receptor blocker is currently not advocated for the treatment of hypertension because of lack of proof of benefit of the combination for blood pressure control. If a third drug is required, a low dose thiazide-like diuretic, possibly in combination with a potassium-sparing agent, is recommended. There is no unequivocal evidence that antihypertensive agents would impair performance in ‘resistance’ sports.
Recommendations for sports participation
Recommendations for participation in competitive sports in athletes with hypertension are based on the results of the evaluation and on the risk stratification (Table 2), and with the understanding that the general recommendations for the management of hypertension are observed as described above and provided that the clinical condition is stable. Table 3 summarizes the recommendations with regard to competitive sports participation [28]. The same recommendations may apply to patients who aim to engage in hard or very hard leisure-time sports activities in order to substantially enhance performance. However, most recreational physical activities are performed at low-to-moderate intensity. Dynamic sports activities are to be preferred, but also low-to-moderate resistance training is not harmful and may even contribute to blood pressure control [35]. In case of cardiovascular or renal complications, the recommendations are based on the associated clinical conditions.
Finally, all patients should be followed-up at regular intervals, depending on the severity of hypertension and the category of risk. In addition, all exercising patients should be advised on exercise-related warning symptoms, such as chest pain or discomfort, abnormal dyspnoea, dizziness or malaise, which would necessitate consulting a qualified physician.
Footnotes
Acknowledgements
The authors gratefully acknowledge the secretarial assistance of N. Ausseloos.