
Abstract
Background
Ambulatory electrocardiogram monitoring (Holter) with ST-analysis as a measure of myocardial ichemia has in populations with coronary heart disease been shown to predict major coronary events: death, myocardial infarction or coronary revascularization. There has, however, been conflicting evidence regarding the usefulness of this technique in identification of healthy subjects with increased risk for coronary heart disease. The aim of this study was to assess if Holter monitoring with ST-analysis could be used to predict future major coronary events in asymptomatic middle-aged men with a defined aggregation of traditional risk factors for coronary heart disease.
Methods
One hundred and fifty-five asymptomatic participants from the city of Malmö, Sweden, with known levels of conventional cardiovascular risk factors underwent Holter monitoring for analysis of transient ST-segment depression at the age of 55 years. Fifteen years after the Holter monitoring, hospital records, diagnosis and death registries were revisited for major coronary events.
Results
An ST-segment depression of 1 mm or greater (0.1 mV) was considered significant for myocardial ischemia and was found in 54 of the 155 men. There were no significant differences in risk factors in the two groups at baseline. The 15-year incidence of a first major coronary event was significantly higher in men with ST-segment depression (39%) than in men without ST-segment depression (20%) (P < 0.015). A Holter electrocardiogram could predict future major coronary events with a positive and negative predictive value of 35 and 80%, respectively.
Conclusions
Holter monitoring can be used as a complement to conventional risk factor evaluation in deciding whether or not to treat risk factors for CHD in asymptomatic subjects.
Keywords
Introduction
It is a well-established fact that the risk for coronary heart disease (CHD) is related to factors such as age, sex, hypercholesterolemia, hypertension, and smoking [1,2]. It has also been long-established medical practice to treat these risk factors in high-risk subjects such as those with known CHD or with markedly elevated risk factors [3].
In the healthy, general population, however, there has been greater controversy as to whether or not to treat only moderately increased risk factors for CHD due to the low absolute risk of disease [4]. The Multiple Risk Factor Intervention Trial (MRFIT) failed to show any significant effect on cardiovascular mortality after 7 years of multiple risk factor intervention [5]. In an a priori defined subgroup of subjects with an abnormal ST-segment response to a heart-rate-limited exercise electrocardiogram (ECG), however, the CHD mortality rate was 57% lower with than without risk factor treatment [6].
The view on risk factor management in healthy individuals advocated by the European Society of Cardiology is to calculate the impact of multiple risk factors on cardiovascular mortality. The recently presented Systematic Coronary Risk Evaluation (SCORE) system takes into account the synergistic risk of several risk factors, such as age, sex, smoking status, serum cholesterol and systolic blood pressure, on future cardiovascular mortality [7]. This system does not take into account all known risk factors for disease, however, and consequently can only predict events to a certain amount.
Transient ST-segment depression (STD) is considered a marker for coronary ischemia [8]. The two best-established methods of measuring STD are exercise and ambulatory ECG (Holter monitoring). Exercise ECG testing has been shown to predict cardiovascular mortality not only in patients with coronary artery disease but also in asymptomatic subjects [9–11]. In previous studies, STD as determined with Holter monitoring, has only been able to predict future major coronary events (MCEs) in patients with clinical manifestations of CHD such as stable and unstable angina pectoris or after a myocardial infarction [12–18]. In those groups, the incidence of coronary artery disease has been sufficient for the Holter method to identify subgroups at significantly increased risk of cardiac events. There has been conflicting evidence, however, as to whether or not STD determined with the Holter technique is of prognostic value in populations such as asymptomatic middle-aged men without markedly elevated risk factors [19–22].
The aim of this study was to investigate whether Holter ST-analysis as a complement to multiple risk factor analysis yields further predictive information regarding future MCEs in a cohort of asymptomatic, middle-aged men with a defined accumulation of risk factors for cardiovascular disease.
Methods
Between the years 1983 and 1986, a total of 2785 men comprising the two cohorts born in 1928 and 1931, at an age of 55 years, were invited to participate in a health-screening program in the city of Malmö in southern Sweden. Seventy-one percent (n = 1977) accepted and underwent cardiovascular risk factor screening. Subjects with serum cholesterol of 7.8 mmol/l or higher, serum triglycerides 4.0 mmol/l or higher, or diastolic blood pressure 105 mmHg or higher were recommended treatment and further follow up. Intervention was also offered to those with multiple risks (14 or more points) in a multiple risk scoring system used in this program. This was an arbitrary, non-validated system in which quintile distribution was obtained from the distribution of serum cholesterol and serum triglyceride concentrations in previous health screenings of five age cohorts of men aged 45-50 years. Self-reported smoking habits and diastolic blood pressure were rated one to four on arbitrary scales (Table 1). From this population of 1977 subjects, all men with aggregated risk scores of 10-13 but without any single risk factor requiring treatment were screened for participation in this study (n = 542). Of these, 237 subjects were found to be without any history of cardiovascular disease, treatment for hypertension, hyperlipidemia or diabetes and were invited to participate. One hundred and fifty-five (65%) accepted and constituted the study population. They were all investigated for two consecutive 24-h periods using an FM ECG tape recorder, and evaluated regarding ST-segment depression. At the day of Holter monitoring smoking status, blood pressure, fasting blood glucose, hemoglobin A1c, total, low-density lipoprotein (LDL) and high-density lipoprotein (HDL)-cholesterol levels, serum triglycerides, and serum γ-glutamyltransferase (GGT) were measured. Smoking habits were self-reported. Systolic and diastolic blood pressure was obtained using a sphygmomanometer after 15 min of rest in a supine position. Total cholesterol, HDL-cholesterol, serum triglycerides, blood glucose, haemoglobin A1c and GGT were sampled in a fasting state and analysed according to standardized procedures of the local laboratory. LDL-cholesterol was calculated according to Friedewald's formula. No subject had serum triglycerides over 4.0 mmol/l. No information was given on the results of the Holter monitoring.
After 15 years, the time to first MCE, defined as death, myocardial infarction (MI), coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI), that had occurred in the 155 participants were determined by screening of hospital records and diagnosis and death registries. The hospital is the only one treating patients for MI and performing PCI in the city of Malmoö. CABG is performed at the nearby University Hospital in the city of Lund but records of operations are kept in the patient's files in Malmöo. The death registry is national and covers all inhabitants of Sweden. The endpoint MI was defined according the revised American College of Cardiology and European Society of Cardiology criteria as elevated markers of cardiac injury (CK-MB or troponin I or T) coupled with either ischemic symptoms with a duration of at least 15 min or ECG changes consistent with MI [23]. The study was approved by the ethical committee of the Faculty of Medicine, University of Lund, Sweden.
The arbitrary risk score system used to classify participants in the study

Holter analysis
An ECG tape recorder, Oxford Medilog II FM type (Oxford Medilog Inc. Abington, UK), was used for continuous 48-h two-channel ECG-recordings, with two pairs of bipolar electrodes in the CM-V1 and the CM-V5 locations. The negative electrode was placed under the middle part of the right clavicle. The frequency response with this equipment is 0.05-100 Hz [24]. This method has previously been described and used in another Malmö cohort investigation [19]. A calibration signal (10 mm = 1 mV) was included at the beginning of each tape. Every STD detected was recorded on an ECG-strip at a rate of 25 mm/s. The two markers for the ST-segment analysis were set manually at the isoelectric interval between the P and Q waves, and between the S and T waves at 60 ms after the junction point. Only ST-segment depressions of the ischemic type were included in the analysis. Significant ischemic-type STD was defined as one or more episodes of planar or downsloping shift of 1 mm (0.1 mV) or more from the isoelectric baseline, occurring at least 0.06s after the J-point and with a duration of at least 1 min [25].
Statistical analysis
A log-rank test was used to assess differences in MCE-free fraction between the two groups. The two-tailed Student's t-test for independent samples was used to assess differences between normally distributed continuous variables. Hemoglobin A1c, GGT, triglycerides and SCORE calculations were not normally distributed and were log-transformed prior to statistic calculations.
Mann-Whitney's U test was used when continuous variables were not normally distributed. The χ2 test was used to assess differences in variables with binary responses. No adjustments were made for multiple comparisons. P values under 0.05 were considered statistically significant. The software used was STATISTICA (StatSoft, Inc., Tulsa, Oklahoma, USA) for Windows version 5.1 and SPSS 12.0.1 (SPSS Inc., Chicago, Illinois, USA) for Windows.
Retrospective evaluation of coronary heart disease risk
The scoring system used at the initiation of the study was a non-validated local approach to obtain a holistic view on the accumulated risk. All patients were retrospectively analysed using the SCORE system in order to obtain an up to date estimation of their cardiovascular risk, using age, systolic blood pressure, smoking habits and serum cholesterol at the time of Holter monitoring.
Results
Risk factors
Due to the study design, age and sex were the same in both groups. Baseline levels regarding major risk factors for CHD and predicted risk for fatal CHD calculated by the SCORE system were not statistically different as is shown in Table 2. Information on alcohol consumption was not available but the levels of GGT were similar in both groups, which to a certain degree can indicate the level of alcohol consumption to be fairly equal in the study population [26].
Holter monitoring
STD was found in 54 of the 155 men (35%) during the 48-h Holter monitoring. Ten men had STD during only one of the two 24-h periods, four of them (7.4% of the 51 men) only during the second 24-h period. The median number of periods with STD was 3 (range 2-8) during the first day and 2 (range 2-6) during the second day, and the corresponding median durations were 18 (range 11986) and 17 (range 2-1033) min, respectively. The diurnal distribution of STD manifested a peak between 6 a.m. and 9 a.m. and another between 9 p.m. and 11 p.m.
Major coronary events
During the 15-year follow-up period, in total 40 of the 155 men suffered their first MCE (26%). Of the total number of MCEs, 20 (39%) occurred in the STD group (n =54), and 20 (20%) in the group without STD (n =101). Event-free time to first MCE was significantly longer in the subjects without STD compared with those with STD (P < 0.015) (Fig. 1). The mean time to first MCE was 103 months in the non-STD group and 87 months in the STD group.
Baseline characteristics determined at the time of Holter monitoring
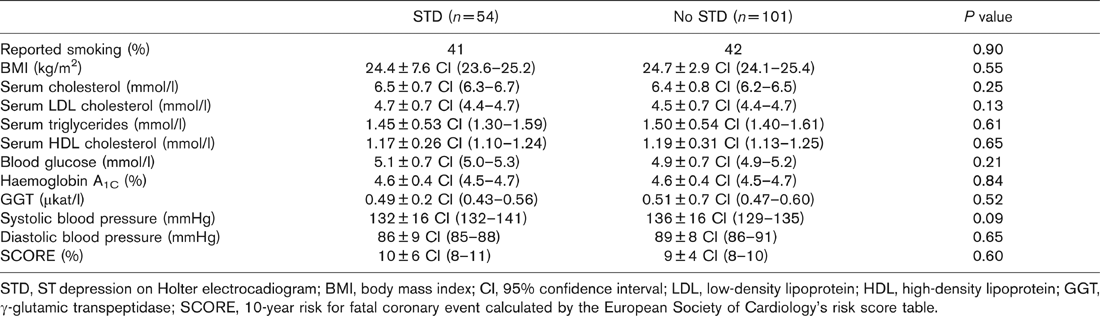
STD, ST depression on Holter electrocadiogram; BMI, body mass index; CI, 95% confidence interval; LDL, low-density lipoprotein; HDL, high-density lipoprotein; GGT, γ-glutamic transpeptidase; SCORE, 10-year risk for fatal coronary event calculated by the European Society of Cardiology's risk score table.
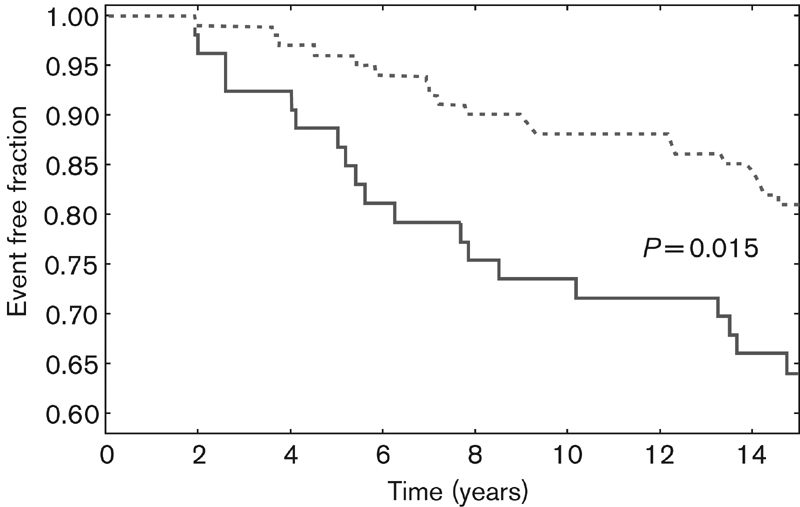
Fraction of subjects free from major coronary events in the ST-segment depression (STD; filled line) and no STD (dotted line) groups over 15 years.
Distribution and classification of first major coronary event in the study population
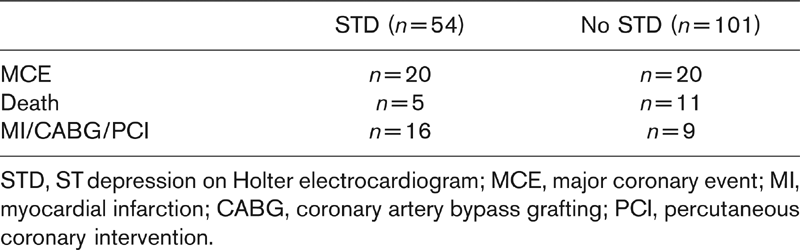
STD, STdepression on Holter electrocardiogram; MCE, major coronary event; MI, myocardial infarction; CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention.
The distribution and classification of MCEs in the study group is shown in Table 3. The sensitivity and specificity for STD to predict a future MCE was 51 and 71%, respectively. In this study, Holter monitoring had a positive predictive value of 39% and a negative predictive value of 80% to predict a first MCE during the 15-year follow-up period.
Discussion
This study has shown that Holter monitoring can identify a low and high-risk subgroup for subsequent MCEs among asymptomatic middle-aged men with a defined risk factor accumulation. In the present study the prevalence of Holter-detected STD was 35%, a figure of the same order as those previously obtained among healthy 68-year-old men and patients with non-Q wave myocardial infarction [9,10] In this kind of population, STD has been found to be of prognostic value for subsequent cardiovascular events. This study has shown that Holter ECG, as a complement to traditional risk factor analyses, could aid in the decision making on whether or not to start preventive therapy for CHD. Absence of STD during Holter monitoring proved to be connected to reduced risk for MCEs during a 15-year follow-up period. During the 15-year follow-up time it is reasonable to presume that several of the subjects will have been offered medical risk factor treatment, as guidelines regarding prevention of CHD have been issued during this period. There is, however, no reason to believe that either group have benefited more than the other in this respect.
Since risk factors have synergistic effects on the development of CHD, a holistic approach to intervention is warranted. There will always be limitations to any system aiming at predicting future risk, however, because, for practical reasons, not all risk factors can be taken into account. Ideally, we seek methods for determining risk in order to treat the correct patients correctly and to avoid life-long treatment in subjects for whom the benefit of treatment is relatively low and the economic burden and risk of side effects of medication has to be taken into account. Another problem is that it can be difficult to persuade asymptomatic patients to adhere to long-term medication and other preventive measures [27]. Studies have shown that lay people and clinicians have different attitudes to start preventive treatment [28]. If hard evidence for future CHD is lacking, we believe that Holter ECG could be used in aiding the clinician to persuade healthy subjects to adhere to preventive measures.
In the SCORE system, recently developed by the ESC, a 10-year risk of a fatal cardiovascular event of 5% warrants treatment [7]. All participants in our study were retrospectively scored according to this system and there were no significant differences in baseline risk between the groups with and without STD. Even though, by modern guidelines, a significant number of these subjects should be given preventive treatment, it seems that Holter monitoring is able to identify a subgroup with a relatively low risk of MCEs when used as a complement to conventional risk factors.
For ethical reasons we excluded those participants from the original health screening program who had high aggregated risk scores (14 or higher), and those with high single risk factors, serum cholesterol over 7.8 mmol/l, serum triglycerides over 4.0 mmol/l, and diastolic blood pressure over 105 mmHg. These cut-off levels for treatment are high by modern standards but were considered acceptable at the start of the study and reflect the views on risk factor treatment in the mid-1980s.
Apart from exercise ECG and Holter monitoring, several other methods for increasing the power to predict coronary events have been suggested. C-reactive protein was shown to correlate with future coronary events in both men and women in a primary prevention setting [29,30]. B-type natriuretic peptide is a predictor of future coronary events in patients with acute coronary syndromes [31]. Another way of predicting future coronary events is to estimate the coronary plaque burden, either indirectly, measuring carotid intima-media thickness or more directly with electron-beam computerized tomography [32]. It is hitherto not clear how well these methods work in clinical practice. The future will tell how these tools will fit into the diagnostic and prognostic armamentarium for CHD.
Limitations of the study
Several limitations to this study have to be taken into account. The study population was selected as those with the highest combined risk among those who were left without risk factor intervention. Thus our study population was, by selection, asymptomatic men with, what was considered at the time, only moderately increased risk factors for CHD. It is not known if the results can be extrapolated to women, subjects of other age categories or with a different risk factor profile. The method for calculating high risk was not validated but was based more on the widespread knowledge of the synergistic interactions between risk factors for CHD. We used 48-h Holter monitoring as opposed to the 24-h monitoring which is common practice today. Thus, we cannot exclude that this study would have been inconclusive with a shorter recording time although, only a relatively small number of patients had STD in only one of the two consecutive 24-h periods. Modern techniques using computer memories rather than cassette tapes could probably overcome the drawbacks of changing tapes after 24 h enabling longer monitoring. The classification of MCEs is based on registries and patients' files where available. Death registries and coronary intervention registries can be considered to be accurate but there is a possibility that subjects have been treated for an MI in another hospital and thus not been registered in the hospital records in Malmö. The University Hospital, however, is the only emergency hospital serving the city of Malmoö.
Conclusion
In conclusion, Holter monitoring can be used as a complement to conventional risk factor evaluation in deciding whether or not to treat risk factors for CHD in asymptomatic subjects.
Footnotes
Acknowledgements
The authors would like to thank the staff of the Holter monitoring laboratory at the University Hospital in Malmoö for performing the recordings and analyses and Jan Åke Nilsson for expert statistical advice.