
Abstract
Aims
The objective of this study is to determine the status of major risk factors for coronary heart disease in patients with established coronary heart disease in Croatia and whether the Joint European Societies’ recommendations on coronary heart disease prevention are being followed in Croatia and whether secondary prevention practices have improved between 1998 and 2003.
Methods
Five surveys were undertaken in 35 centres covering the geographical area of the whole of Croatia between 1 June, 1998 and 31 March, 2003. Consecutive patients of both sexes were identified after coronary-bypass grafting or a percutaneous transluminal coronary angioplasty or a hospital admission with acute myocardial infarction or ischaemia. Data collection was based on a review of medical records and the methodology used was similar to the one used in the EUROASPIRE study.
Results
Fifteen thousand, five hundred and twenty patients were enrolled (64.6% men); 35% of patients smoked cigarettes, 66% had raised blood pressure, 69% elevated serum total cholesterol, 69% elevated serum low-density lipoprotein (LDL) cholesterol, 42% low high-density lipoprotein (HDL) cholesterol, 37% elevated triglycerides, 30% diabetes and 34% family history of coronary heart disease. More men were smokers and had low HDL cholesterol, but more women had elevated total and LDL cholesterol, hypertension and diabetes. More men had Q wave acute myocardial infarction, but more women had angina. Over 5 years, the prevalence of hypercholesterolemia decreased substantially from 82.7 to 65%. Eighty-three percent of patients received aspirin and this percentage did not change during the study. The use of diuretics, calcium antagonists and nitrates did not change either. The reported use of statins, angiotensin-converting enzyme inhibitors and beta-blockers increased significantly.
Conclusion
This survey shows a high prevalence of modifiable risk factors in Croatian patients with coronary heart disease. Although the higher use of statins, angiotensin-converting enzyme inhibitors and beta-blockers is encouraging, the fact that most coronary heart disease patients are still not achieving the recommended goals remains a concern. There is real potential to reduce the very high coronary heart disease morbidity and mortality in Croatia.
Introduction
Cardiovascular and cerebrovascular diseases, of which ischemic heart disease is the most common, are the world's leading cause of death, being responsible for the death of 16.6 million people annually, with Europe accounting for 5 million of these [1]. Cardiovascular diseases are the main cause of death in Croatia (total population 4437460) as well. Of all the deaths in 2003 in Croatia, 52.8% (27872) were due to such diseases [2].
The standardized cardiovascular death rate (SDR) in Croatia increased from 1980 when it was 344.25 up to 551.74 per 100000 inhabitants in 1990. Since then a moderate decrease has occurred with a rate of 488.0 per 100000 in 1995. It started to increase again in the late 1990s so that it reached 589.72 in 1999 and then it started to decrease again to 482.48 per 100000 in the year 2002. Today, however, it is still slightly worse than the European average, which was 553.34 in 1980 but decreased so that in the year 2002 it was 474.76 per 100000.
Relatively unfavourable trends are seen when analysing SDR for ischaemic heart disease in Croatia as well. In 1985 it was 87.85 per 100000 inhabitants but in 1991 it was 129.73 and in 1998 it was 207.91. Afterwards, a significant decrease was noted so that in 2003 it was 159.48 per 100000. SDR for ischaemic heart disease for the age group 0–64 years increased until 1991 (in this year it was 43.0 per 100000). For several years it remained more or less unchanged and after 1998 it slowly decreased so that in 2003 it was 37.58 per 100000. So, for the last 25 years the SDR for ischaemic heart disease for this age group in Croatia has been lower than the European average but higher than the European Union average [2].
With a share of 13.8% of all hospitalizations, and a hospitalization rate of 1692.1 per 100000 in the year 2002, cardiovascular diseases are also the leading cause of hospitalization in Croatia [2]. As they also cause a significant number of years of life lost, these diseases are definitely the number one public health priority in Croatia today.
Therefore, the Croatian Cardiac Society decided to launch a national survey on current practice - Treatment and Secondary Prevention of Ischemic Coronary Events in Croatia (TASPIC-CRO) - based partially on the experience from EUROASPIRE I and II [3, 4]. The aims of this study were as follows: to determine the status of major risk factors for coronary heart disease (CHD) - cigarette smoking, blood pressure, cholesterol, diabetes and family history of CHD - and their management as recorded in patients’ medical records, as well their prevalence in CHD patients in Croatia as these conventional risk factors play a major role in future risk of CHD [5, 6]; to determine whether the Second Joint European Societies Task Force guidelines on coronary prevention, published in 1998 [7], were being followed, particularly concerning modifiable risk factors such as hyperlipidemia and hypertension, and whether these had changed at discharge compared with admission; and to determine whether the secondary prevention practices in patients with established coronary disease had improved between 1998 and 2003.
Study population and methods
The methodology used in this study was similar to the one used for EUROASPIRE I and II [3, 4], except that there was no systematic interviewing and examination of the patients after their discharge. Therefore, no data concerning patients’ lifestyle and risk factor status at interview 6 months after the discharge can be presented in this paper. The survey was undertaken in 35 centres (seven university hospitals, 25 general hospitals and three rehabilitation hospitals) in 28 Croatian cities covering the geographical area of the whole of Croatia.
In all hospitals doctors were asked to report consecutive patients of both sexes with the following diagnoses or treatments: CHD, coronary artery bypass graft (CABG), percutaneous transluminal coronary angioplasty (PTCA) or percutaneous coronary intervention (PCI), acute myocardial infarction (AMI), International Classification of Diseases (ICD)-9410, and acute myocardial ischaemia ICD-9411–413. The data were provided from diagnostic registers, patients’ records, hospital discharge lists or other medical documents and the criteria for diagnosis and procedures were the same as described in EUROASPIRE II. The dates of the hospitalization of patients ranged for TASPIC-CRO I between 1 June and 31 October, 1998, for TASPIC-CRO II between 1 April and 30 September, 1999, for TASPIC-CRO III between 30 September, 2000 and 14 April, 2001, for TASPIC-CRO IV between 1 September, 2001 and 28 March, 2002, and for TASPIC-CRO V between 30 September, 2002 and 31 March, 2003. A difference from EUROASPIRE was that patients older than 70 years were also included.
The following information was obtained from the patients’ hospital medical records for any time prior to the date of acute hospital admission or procedure, and at the discharge: personal and demographic details; personal history of CHD and interventional procedures (PTCA and CABG); risk factor recordings; history of cigarette smoking, hypertension, hyperlipidemia and diabetes; family history of coronary heart disease in first degree blood relatives; medication.
The difference between the present study and EURO-ASPIRE was that no interview was conducted so breath carbon monoxide was not measured to validate reported smoking habit. Quality assurance was performed as described in EUROASPIRE. In this paper only descriptive statistics are given, which were used to estimate the prevalence of risk factor recording and management by diagnostic category.
Results
All together 15520 patients’ medical records were analyzed. In TASPIC-CRO I 2540, in II 2586, in III 3223, in IV 4051 and in V 3054 medical records were reviewed. Some of the data from TASPIC-CRO I were later lost, however, so the comparisons are made without them.
In TASPIC-CRO I 34% patients were women, 2% of patients were between 21 and 40 years, 37% between 41 and 60 years, 58% between 61 and 80 years and 3% 81 years and older. In TASPIC-CRO II 34.1% were women, 15% of patients were younger than 50 years, 24% were between 51 and 60 years, 35% were between 61 and 70 years and 26% were 71 years and older. In TASPIC-CRO III 35.3% were women, 11% of patients were younger than 50 years, 23% were between 51 and 60 years, 37% were between 61 and 70 years and 29% were 71 years and older. In TASPIC-CRO IV 35.8% were women, 12% of patients were younger than 50 years, 21% were between 51 and 60 years, 35% were between 61 and 70 years and 32% were 71 years and older. In TASPIC-CRO V 36.1% were women, 14% of patients were younger than 50 years, 20% were between 51 and 60 years, 34% were between 61 and 70 years and 32% were 71 years and older.
Table 1 shows the male-female ratio and the mean age of the patients. There were no sex differences concerning hypertriglyceridemia and family history of CHD, but more men were smokers and had low high-density lipoprotein (HDL). More women, however, had hypercholesterolemia, high low-density lipoprotein (LDL) cholesterol, hypertension and diabetes (Table 2).
During the 5 years between TASPIC-CRO II and V the prevalence of hypercholesterolemia decreased from 82.7% in 1998 to 65% in 2003. This is a statistically significant, linear decrease (Fig. 1).
The analysis of hypercholesterolemic patients was performed and their data were compared with those of normocholesterolemic patients (Fig. 2). Hypercholesterolemic patients had increased LDL cholesterol and triglycerides more often but also less often low HDL cholesterol than those with normal plasma cholesterol.
The only significant difference concerning sex and diagnosis was that more men had Q wave AMI in TASPIC-CRO II (X 2 = 8.224; df = 1; P = 0.004), IV (X 2 = 27.603; df = 1; P <0.0001) and V (X 2 = 38.116; df = 1; P <0.0001). Women, however, had stable angina more often in TASPIC-CRO III (X 2 = 9.531; df = 1; P = 0.002), IV (X 2 = 34.083; df = 1; P = 0.0001) and V (X 2 = 12.004; df = 1; P = 0.0001) but also unstable angina in TASPIC-CRO IV (X 2 = 5.051; df = 1; P <0.0001) and V (X 2 = 13.302; df = 1; P = 0.0001). Post-infarction angina occurred significantly more often in men only in TASPIC-CRO IV (X 2 = 9.706; df = 1; P = 0.002) (Table 3).
In TASPIC-CRO I 82.7% of patients had hypercholesterolemia, 28.1% hypertriglyceridemia, 53.0% had hypertension and 33% were smoking. At admission 86.8% of patients were taking aspirin, 29.4% a beta-blocker, 48.2% an angiotensin-converting enzyme (ACE) inhibitor, 94.8% a nitrate and only 1.5% a statin. At discharge 85% of patients were taking aspirin, 34.1% a beta-blocker, 46.4% an ACE inhibitor, 94.5% a nitrate and 4.5% a statin. CABG was performed in 4.4% patients and PTCA in 2.7% patients.
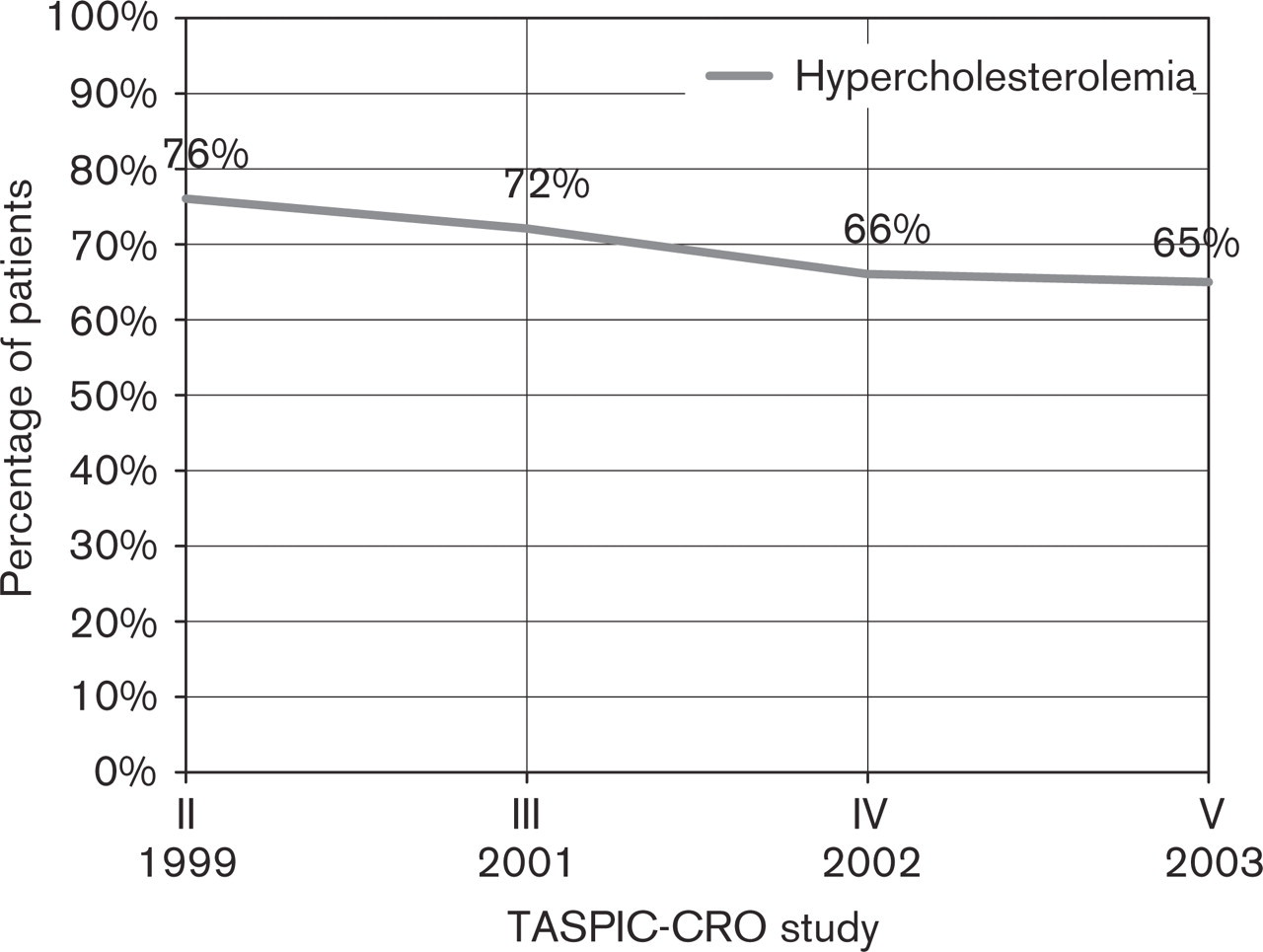
Changes in hypercholesterolemia prevalence 1999-2003.
Sex and age of the patients
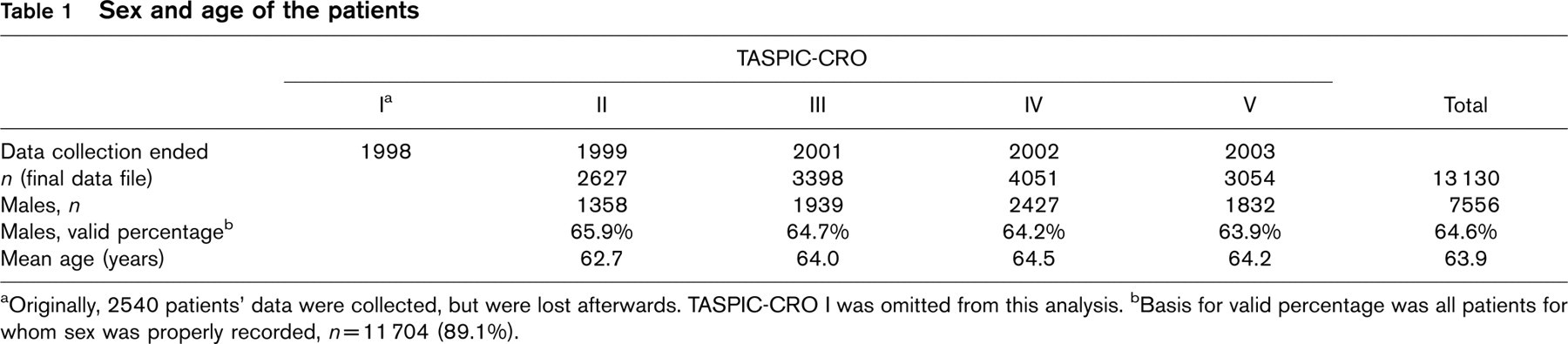
aOriginally, 2540 patients’ data were collected, but were lost afterwards. TASPIC-CRO I was omitted from this analysis. bBasis for valid percentage was all patients for whom sex was properly recorded, n = 11704 (89.1%).
Prevalence of risk factors by sex of the whole TASPIC-CRO sample
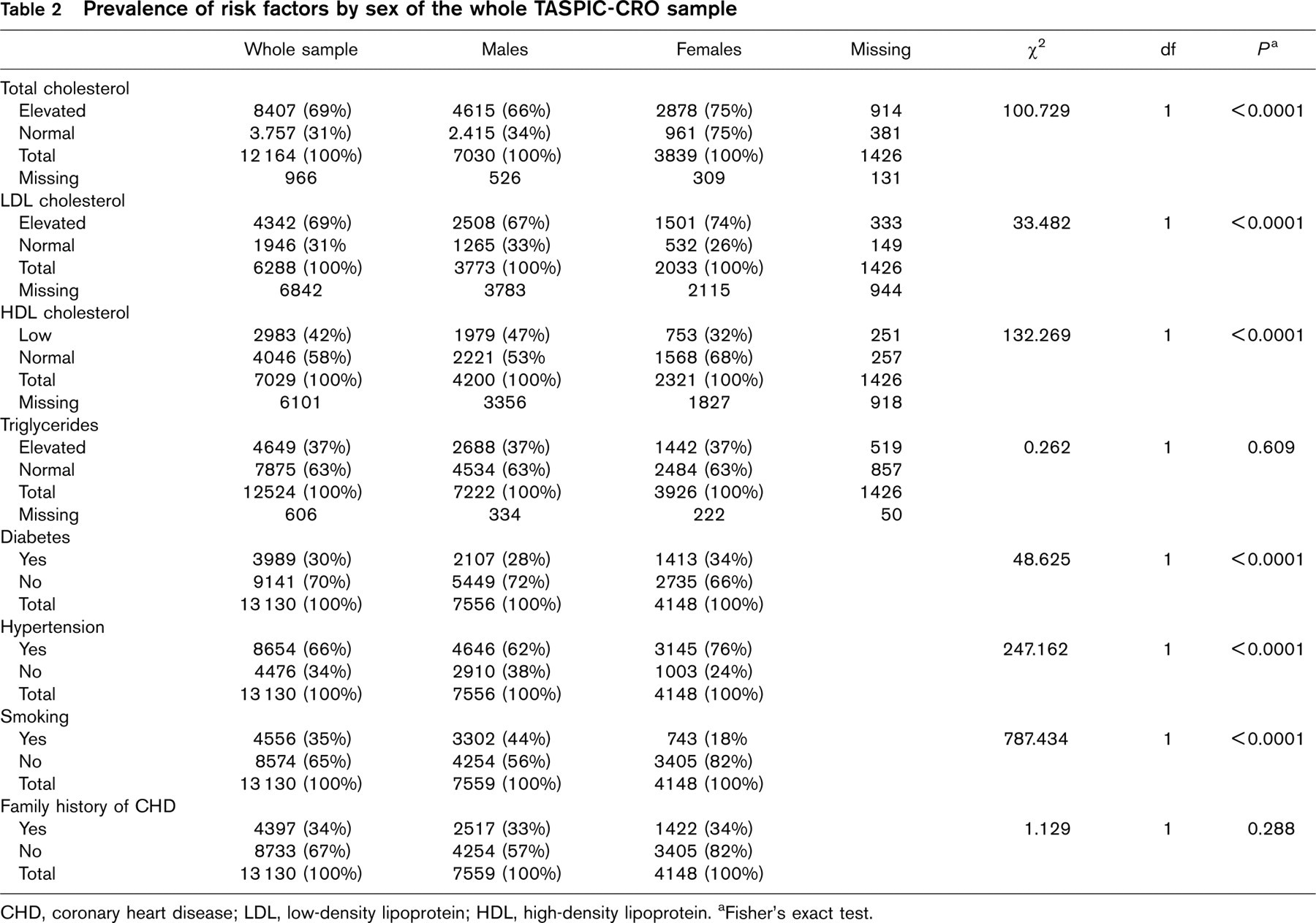
CHD, coronary heart disease; LDL, low-density lipoprotein; HDL, high-density lipoprotein. aFisher's exact test.
In TASPIC-CRO II CABG was performed in 4% of women and 11% of men (P = 0.0001) and PTCA in 2% of women and 3% of men (NS). When the patients with hypercholesterolemia were analysed and compared with others there was no significant difference regarding family history of CHD, hypertension and diabetes, but more hypercholesterolemic patients had hypertriglyceridemia (P = 0.0001) and smoked (P = 0.042).
In TASPIC-CRO III urgent CABG was performed in 1% of women and 1% of men (NS) and urgent PTCA in 4% of men and 2% of women (NS). In 10% of men and 5% of women an elective CABG was performed (P = 0.0001), and an elective PTCA was performed in 13% of men and 7% of women (NS). The analysis of hypercholesterolemic patients was also performed and their data were compared with others. There was no significant difference regarding family history of CHD, diabetes and smoking but more hypercholesterolemic patients had high LDL cholesterol (P = 0.0001), hypertriglyceridemia (P = 0.0001), hypertension (P = 0.006) and low HDL cholesterol (P = 0.0001).
In TASPIC-CRO IV urgent CABG was performed in 1% of women and 2% of men (P = 0.0001) and urgent PTCA in 8.2% of men and 5% of women (P = 0.0001). In 6% of men and 3% of women an elective CABG was performed (P = 0.0001), and an elective PTCA was performed in 8% of men and 5% of women (NS). When hypercholesterolemic patients were compared with others there was no significant difference regarding family history of CHD, diabetes, low HDL cholesterol and smoking but more hypercholesterolemic patients had high LDL cholesterol (P = 0.0001), hypertriglyceridemia (P = 0.0001) and hypertension (P = 0.014).
In TASPIC-CRO V urgent CABG was performed in 0.9% of patients and urgent PTCA in 5.1% of patients. In 4.2% an elective CABG and in 7.8% an elective PTCA were performed. Among hypercholesterolemic patients 94% had increased LDL cholesterol, 33% had low HDL cholesterol, 45% had increased triglycerides, 30% were diabetics, 69% had hypertension, 33% smoked and 35% had family history of CHD.
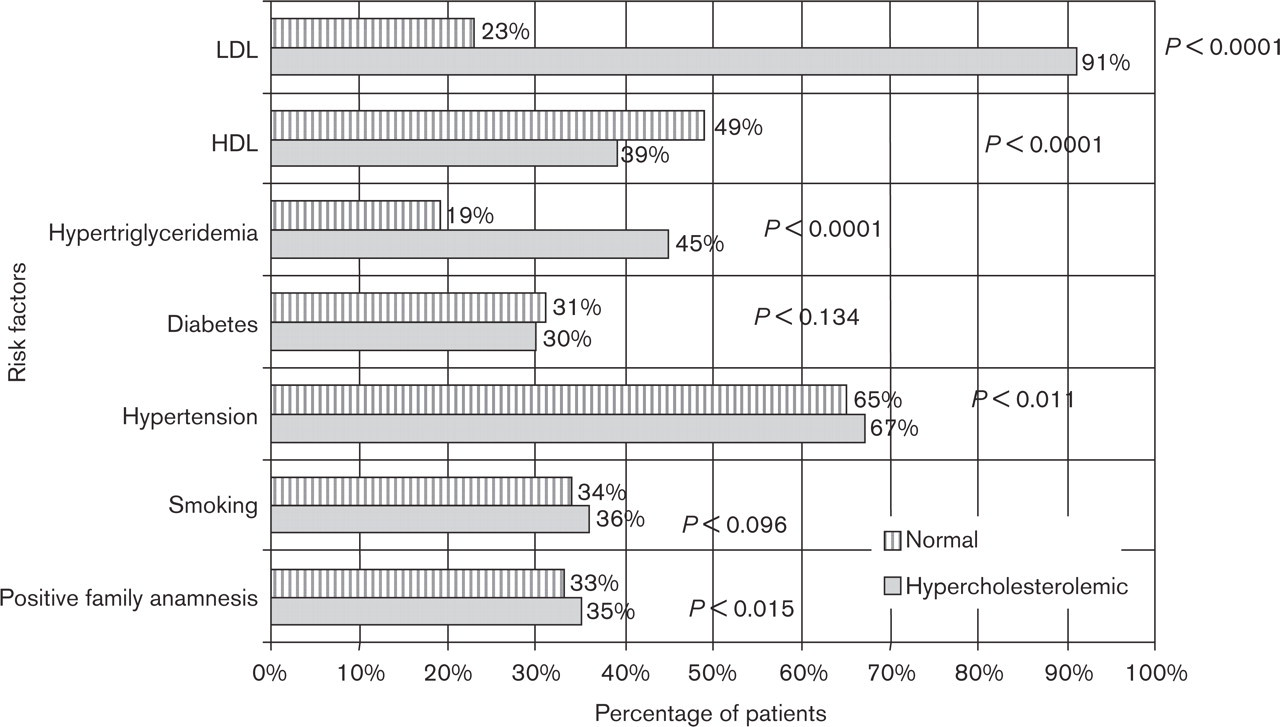
Risk factors prevalence among patients with hypercholesterolemia. LDL, low-density lipoprotein; HDL high-density lipoprotein.
Prevalence of diagnoses in TASPIC-CRO II-V by sex
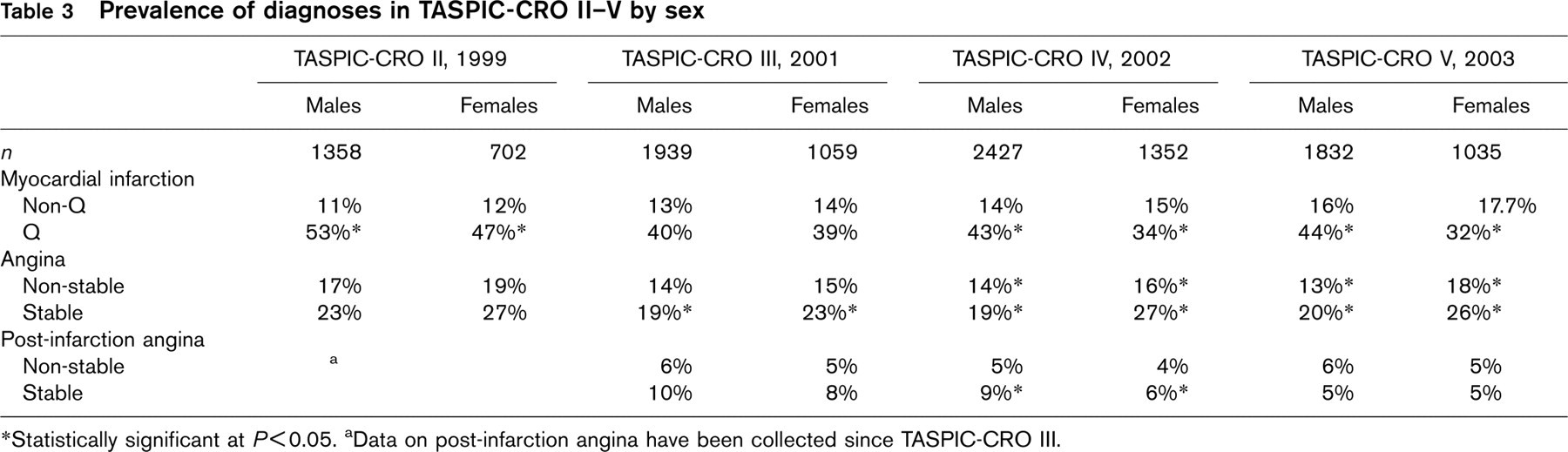
∗Statistically significant at P<0.05. aData on post-infarction angina have been collected since TASPIC-CRO III.
The prevalence of drug therapy at admission and at discharge is shown in Tables 4 and 5. Thrombolysis was given in 15% of AMI patients in TASPIC-CRO II, 21% in TASPIC-CRO III, 29% in TASPIC-CRO IV and 19% in TASPIC-CRO V.
In TASPIC-CRO III heparin was given in 49% of patients (29% low molecular and 20% non-fractioned), in TASPIC-CRO IV in 69% (54% low molecular and 15% non-fractioned) and in TASPIC-CRO V in 58% patients (47 low molecular and 11% non-fractioned) (Table 6).
Discussion
This Croatian survey shows in a large patient population (14523 patients) a high prevalence of modifiable coronary risk factors and under-use of prophylactic drug therapies in patients with established coronary heart disease. It also shows an improvement concerning the use of some prophylactic drug therapies between 1998 and 2003. The lifestyle, risk factor and therapeutic goals set by the Joint European Societies recommendations on prevention of coronary heart disease in clinical practice [7] are still not being realized in a majority of Croatian patients.
The cardiovascular risk factor prevalence at admission in TASPIC-CRO I and II was similar to that in EUROASPIRE I regarding smoking (in TASPIC-CRO I 33%, in II 35% versus EUROASPIRE I 34.4%) and hypertension (in TASPIC-CRO I 53% and in II 57% versus EUROASPIRE I 57.8%) but we had more patients with elevated plasma cholesterol (82.7% in TASPIC-CRO I and 76% in II versus 71.1% in EUROASPIRE I) and diabetics (30% in TASPIC-CRO I and 33% in II versus 21.8% in EUROASPIRE I).
Changes in risk factor prevalence 1999-2003
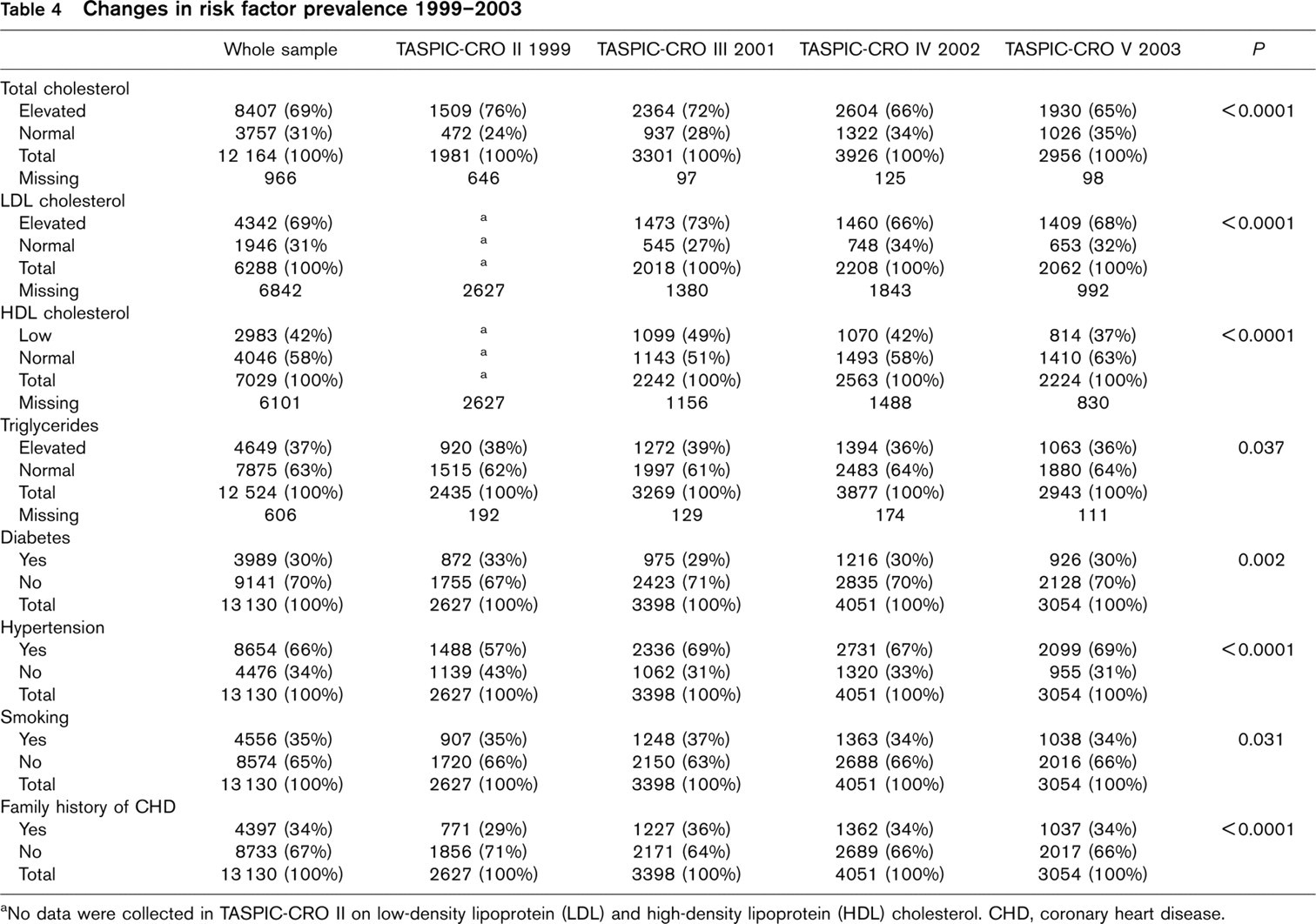
aNo data were collected in TASPIC-CRO II on low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol. CHD, coronary heart disease.
Recorded medication on admission

ACE, angiotensin converting enzyme.
Recorded medication at discharge

ACE, angiotensin converting enzyme.
The comparison of plasma cholesterol requires qualification because in TASPIC-CRO I-III values over 5.2mmol/l were used and in TASPIC-CRO IV and V values over 5.0 mmol/l were defined as increased plasma total cholesterol concentration according to the Second Joint European Societies recommendation on cardiovascular prevention [7]. In EUROASPIRE I the value for cholesterol was 5.5 mmol/l or above.
Since in this survey no interview was performed 6 months after hospitalization, the only possible comparison of drug therapies is between our data at discharge and reported medication at time of interview in EUROASPIRE. We are aware that such a comparison is not completely adequate, but it can indicate some trends. In Croatia the use of antiplatelet medication was very similar (82.7% in TASPIC-CRO I versus 81.2% in EUROASPIRE I). More Croatian patients were given ACE inhibitors (48.2 versus 32% in EUROASPIRE I) and nitrates (84.8 versus 49.2%), but fewer received beta-blockers (29.4 versus 53.7%) and much fewer lipid-lowering drugs (1.5 versus 32%).
When the TASPIC-CRO data are compared with those from EUROASPIRE I, in TASPIC-CRO II there was about the same percentage of patients with elevated plasma cholesterol (76 versus 71% in EUROASPIRE I), and smokers (35 versus 34.4%) but more patients with hypertension (57 versus 57.8%) and diabetes (33 versus 21.8%).
In TASPIC-CRO II there was no significant difference in the use of antiplatelets (81 versus 81.2% in EUROASPIRE I), and ACE inhibitors (30 versus 29.5%), but the use of nitrates was higher (69 versus 49.8%) while much less beta-blockers (25 versus 53.7%) and lipidlowering drugs were used (15 versus 32% in EUROASPIRE I).
When TASPIC-CRO III is compared with EUROASPIRE II, which was performed at the same time, more Croatian patients had hypercholesterolemia (72 versus 58%), hypertension (69 versus 54%), diabetes (29 versus 22%) and smoked (37 versus 21%).
The adverse lifestyle trends among Croatian CHD patients are a cause for concern [8, 9]. Relatively recent war experience and exposure to long-term stress due to these circumstances, however, might also contribute to unfavourable CHD trends in the 1990s in Croatia [10]. It has been shown that psychosocial factors are closely associated with myocardial infarction [11].
At discharge in TASPIC-CRO III less Croatian patients were prescribed aspirin than in EUROASPIRE II (85 versus 90.3%). The same was true for beta-blockers (57 versus 66.2%). The use of anticoagulants was about the same (10% in TASPIC III versus 12.4% in EUROASPIRE II). More Croatian patients, however, were prescribed lipid-lowering drugs (55 versus 42.7%) and ACE inhibitors (53 versus 37.6%).
When TASPIC-CRO IV is compared with EUROSPIRE II, more Croatian patients had hypertension (67 versus 54%), diabetes (30 versus 22%) hypercholesterolemia (66 versus 59%) and smoked (34 versus 21%). At discharge there were no significant differences in prescribed anticoagulants (10 versus 12.4%), fewer Croatian patients received antiplatelets (83 versus 90.3%) and beta-blockers (60 versus 66.2%), but much more received ACE inhibitors (55 versus 37.6%) and lipid lowering drugs (57 versus 42.7%).
When TASPIC-CRO V is compared with EUROASPIRE II, more Croatian patients had hypertension (69 versus 54%), diabetes (30 versus 22%), hypercholesterolemia (65 versus 59%) and smoked (34 versus 21%). At discharge fewer Croatian patients received antiplatelets (84 versus 90.3%), anticoagulants (9 versus 12.4%) and beta-blockers (49 versus 66.2%) and many more received ACE inhibitors (52 versus 37.6%) and lipid-lowering drugs (71 versus 42.7%).
If we analyse the changes from 1998 to 2003, there is a substantial increase in the prescribing of some prophylactic therapies in Croatia to patients hospitalized because of established CHD. This is particularly true for lipid-lowering drugs and ACE inhibitors, but for beta-blockers this was true until 2002. Knowing that a strong and continuous relationship between total and LDL cholesterol concentration and CHD risk has been proven, and that there are no doubts concerning the efficacy of statins in reducing cardiovascular mortality and the risk of recurrent major CHD events as well as total mortality [12, 13], the increase in prescribing statins is not surprising. The data on beta-blockers suggesting reductions in the risk of recurrent cardiovascular events after AMI [14] are probably the reason for increased usage of this drug class. It is unclear why this trend changes in 2002.
Randomized clinical trials and meta-analyses have demonstrated reductions in recurrent cardiovascular events and death after AMI with ACE inhibitors [15–17]. ACE inhibitors also seem to be beneficial in other patients with established CHD, particularly those with angina. These benefits are sustained over several years [18]. Obviously all these data contributed to the increased prescription of ACE inhibitors.
According to our results, about 85% of patients in Croatia receive antiplatelets (the vast majority, 83%, aspirin) and this percentage did not change. Despite some controversies about the place of aspirin in the prevention of CHD [19] its benefit for secondary prevention is established not only from randomized clinical trials but also from large-scale meta-analyses [20]. These analyses have shown that daily use of low-dose aspirin (75–325 mg/day) reduces the risk of recurrent vascular disease such as AMI and stroke by about one-quarter-for at least 1 month. It has also been shown that in patients with previous AMI, risk of re-infarction is reduced by 31%, with a 12% reduction in death and a 42% reduction in risk of non-fatal stroke. Although data show that clopidogrel has a greater effect on cardiovascular events in patients with previous AMI [19], it was not used very often in Croatian patients until recently. This is because it was registered in Croatia much later than in some other European countries and because of much higher drug costs.
The use of diuretics (about one-third of all patients), calcium antagonists (16–19%) or nitrates (9–11%) also did not change. It has been known for many years that thiazide diuretics have similar benefits to beta-blockers in the primary prevention of CHD [21] and their benefits have recently been clearly confirmed [22]. As several trials showed that nitrate treatment did not improve outcomes early after AMI [23, 24], and may be associated with an increase in cardiac events [25] it is surprising that their use did not decrease. This can probably be explained by the fact that in Croatia they are predominantly used for the prevention or relief of symptoms in patients with angina and not in secondary prevention of CHD. There was also a small increase in prescribing anticoagulants (from 10 to 13%) and a marked decrease in use of digitalis glycosides (from 14 to 7%). The increase in anticoagulants can be explained by the fact that it has been shown that anticoagulants, particularly warfarin, are beneficial and even combining treatment of anticoagulants with aspirin is more effective than either treatment alone [26–28].
Our survey shows a high prevalence of modifiable risk factors in patients with CHD in Croatia, even higher than in some other European countries, and therefore substantial potential to reduce the risk of recurrent coronary events and death. Effective treatments for secondary prevention [20–30] in Croatia, as in some other European countries [31], are being under-used.
Appendix
TASPIC-CRO coordinator: Sime Mihatov
TASPIC-CRO investigators: Marija Agostini, Zagreb; Vladimir Ambroz, Pakrac; Debora Anic Kasuto, Krapinske Toplice; Zdravko Babic, Zagreb; Franjo Baborski, Krapinske Toplice; Anica Badanjak, Popovaca; Zeljka Bakliza, Koprivnica; Ljiljana Banfic, Zagreb; Armida Barbic Bonassin, Pula; Mijo Bergovec, Zagreb; Branko Bilic, Sisak; Stanko Biocic, Zagreb; Mirko Blaskovic, Ogulin; Ivo Bozic, Split; Vojtjeh Brida, Zagreb; Irena Bruketa, Opatija; Antun Car, Dubrovnik; Dusko Cerovec, Krapinske Toplice; Nedeljko Ciglenecki, Krapinske Toplice; Dalibor Cukon, Pula; Dubravka Carzavec, Zabok; Katja Catipovic, Osijek; Zlatko Cubranic, Rijeka; Cepic Nedjeljko, Nova Gradiska; Dijana Delic Brkljacic, Zagreb; Zeljka Diklic, Rijeka; Dubravko Dobrovic, Rijeka; Niksa Drinkovic, Zagreb; Drazen Duplancic, Split; Vesna Emih-Pajalic, Opatija; Damir Fabijanic, Split; Jasna Fabijanic, Opatija; Milica Gabor, Cakovec; Darko Gabric, Zagreb; Duska Glavas, Split; Mladen Gostovic, Zagreb; Janko Grman, Karlovac; Robert Grubisic-Cabo, Sibenik; Mirela Gunjevic-Delisimunovic, Pakrac; Marina Halapir, Krapinske Toplice; Josip Halle, Zagreb; Davor Horvat, Karlovac; Nevenka Horvat, Zagreb; Bachir Hoteit, Duga Resa; Rudolf Hranilovic, Cakovec; Neven Istvanovic, Krapinske Toplice; Suzy Ivancic-Vagaja, Opatija; Mario Ivanusa, Bjelovar; Hrvoje Ivekovic, Zagreb; Marijan Jakic, Osijek; Damir Japundzic, Nova Gradiska; Ivan Jelic, Sisak; Jasna Jelic, Knin; Vesna Jelic, Karlovac; Mirjana Jembrek Gostovic, Zagreb; Melita Jeric, Varazdin; Vladimir Jonke, Zagreb; Nediljko Jukic, Pula; Mario Jurin, Sibenik; Silvija Juzbasic, Vinkovci; Aleksandar Knezevic, Zadar; Marijana Knezevic-Pravecek, Slavonski Brod; Slavica Kojundzic, Sibenik; Mladen Komadina, Zagreb; Branko Krajinovic, Popovaca; Dragica Kramaric, Koprivnica; Stjepan Kranjcevic, Zagreb; Goran Krstacic, Zagreb; Zeljko Kupanovac, Rijeka; Ante Kuzmanic, Split; Maja Lopac, Zagreb; Martina Lovric Bencic, Zagreb; Petar Lozo, Split; Josip Lukenda, Zagreb; Tanja Lukenda, Zagreb; Ajvor Lukin, Split; Ksenija Lukin Eskinja, Opatija; Mladen Makitan, Varazdin; Eduard Margetic, Zagreb; Andreja Maric, Cakovec; Marina Marin, Vinkovci; Branimir Markovic, Split; Richard Matasic, Zagreb; Ivanka Mihajlovic, Vukovar; Bernarda Mihalicek Rubes, Krapinske Toplice; Kresimir Milas, Pula; Davor Milicic, Zagreb; Jure Mirat, Zagreb; Dinko Miric, Split; Rajko Miskulin, Rijeka; Marija Mlinaric, Vukovar; Berislav Mostovac, Virovitica; Katarina Novak, Split; Ljerka Nuic, Popovaca; Branko Ostricki, Cakovec; Marjan Padovan, Rijeka; Vesna Pehar-Pejcinovic, Pozega; Ruzica Perkovic-Avelini, Split; Ksenija Pesek, Zabok; Ruza Petras, Sisak; Davorin Pezerovic, Vinkovci; Karmela Piljak-Altabas, Zagreb; Hrvoje Pintaric, Zagreb; Miroslav Plazanin, Nasice; Ljiljana Pleskalt, Bjelovar; Darko Pocanic, Zagreb; Zeljko Popovic, Virovitica; Marija Puharic-Haraslic, Opatija; Davor Puljevic, Zagreb; Kresimir Putarek, Zagreb; Miroslav Raguz, Zagreb; Drago Rakic, Split; Tahir Ramqaj, Krapinske Toplice; Vjekoslava Raos, Zagreb; Ile Rastegorac, Pozega; Davor Richter, Zagreb; Josip Rubes, Krapinske Toplice; Ljerka Rukavina-Prpic, Opatija; Pejo Samardzic, Slavonski Brod; Bosiljka Siuc-Paro, Rijeka; Bosko Skoric, Zagreb; Dragan Slunjski, Varazdin; Ivan Sokol, Zagreb; Drazen Sebetic, Bjelovar; Jadranka Separovic Hanzevacki, Zagreb; Aljosa Sikic, Zadar; Anton Smalcelj, Zagreb; Kresimir Stambuk, Zagreb; Zorislav Susak, Biograd; Kresimir Sutalo, Koprivnica; Dragan Trivanovic, Pula; Dubravko Trsinski, Varazdin; Ljudevit Ulakovic, Zabok; Roman Urek, Zagreb; Kresimir Vidovic, Popovaca; Josip Vincelj, Dubrava; Slobodanka Vuckovic-Rapaic, Opatija; Marija Vujicic, Split; Duro Vukosavic, Zagreb; Tea Zaninovic Jurjevic, Rijeka; Luka Zaputovic, Rijeka; Josip Zorko, Ogulin; Davorka Zagar, Rijeka